Designing a Scalable Robotic Exoskeleton and Tablet Gaming Suite for Hand Function Rehabilitation (Georgia Institute of Technology)
Brittney English, Jennifer Hunter, Jonathan Tuck, and Gueorgui Tzintzarov
ABSTRACT
Cerebral palsy and stroke are debilitating neurological disorders that reduce motor function (1-2); however, patients who participate in physical therapy sessions, a common treatment for these disabilities, may be able to regain, or retain, some motor function. Unfortunately, many physical therapy patients become bored with therapeutic exercises and reduce their participation, which lengthens recovery time (3). The focus of this project is to extend previous efforts of robotic assisted wrist physical therapy by increasing engagement and the population who could benefit from this technology. We created a scalable, light-weight robotic exoskeleton that functions as a video game controller and a tablet gaming suite with games that facilitate therapeutic exercises. Our system has been validated with healthy subjects and has shown that engagement was increased by a factor of four as compared with traditional exercises. Results also showed that exercise sessions are more productive with the availability of a fitted, lighter weight exoskeleton.
BACKGROUND
Both cerebral palsy and stroke are debilitating neurological disorders that have the potential to permanently damage a person’s body movements and muscle coordination (1-2); however, cerebral palsy and stroke patients who participate in physical therapy sessions, a common treatment for these disabilities, may be able to regain, or retain, some motor function. Patients undergoing physical therapy commonly exhibit pain and boredom with their rehabilitation regimen, which studies have shown decrease a patient’s participation in physical therapy and therefore lengthen recovery time. Furthermore, these studies demonstrate that physical therapy that keeps the patient engaged is more likely to shorten patient recovery time by helping that patient maintain motivation to participate in physical therapy sessions (3-5).
Robotic aided therapy is a new technology that has shown promising results facilitating motor learning in stroke patients (6-9). However, existing systems are large, heavy, and expensive. Another problem with these systems is that they are created to be one-size-fits-all. Most are created to fit the average adult male, but allow for some adjustment to tighten or loosen the device. Unfortunately, children are significantly smaller than the average adult male, which does not allow these therapy options to be feasible for children. Furthermore, significantly more women suffer from strokes than men (2). Since women are smaller than men, on average, many of them are also not able to benefit from these new therapeutic technologies. Currently, there is no known exoskeleton arm with these therapeutic capabilities available to smaller women and children.
PROBLEM STATEMENT
The focus of this project is to extend previous efforts of robotic assisted wrist physical therapy sessions by increasing engagement and the population who could benefit from this technology. We aim to create a scalable arm exoskeleton that allows our design to provide gaming rehabilitation systems to a larger population of individuals, including female stroke survivors and children with cerebral palsy.
DESIGN
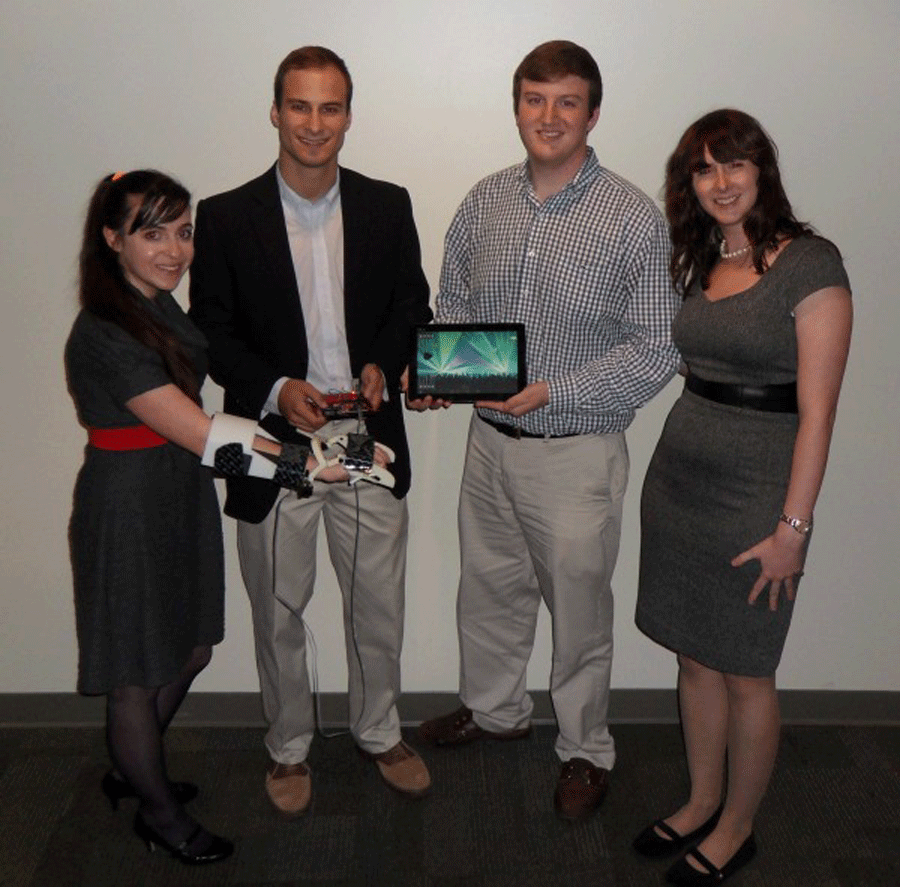
Figure 1. The scalable robotic exoskeleton.
The goal of this project is to design a robotic exoskeleton and tablet gaming suite that promotes engagement and productivity in at-home therapeutic exercises. To achieve this goal, we created a robotic exoskeleton that communicates via Bluetooth with a tablet and acts as a video game controller. We also created fun and engaging tablet games that facilitate therapeutic wrist exercises.
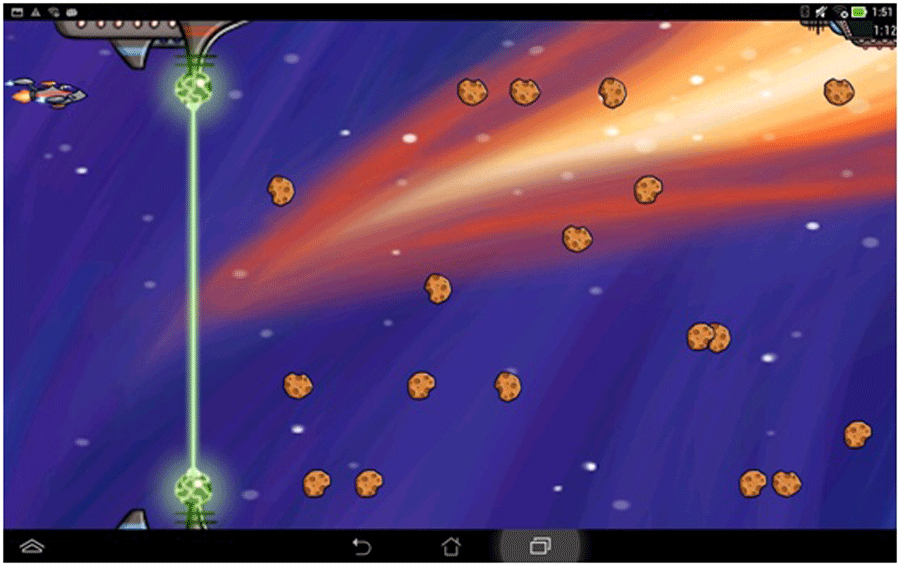
Figure 2. RoboBlaster tablet game.
Our goal for developing robotic hardware was to design a robotic exoskeleton to be easily scalable, light-weight, and able to fit patients of all sizes and ages. As such, we developed a process that uses rapid-prototyping methods to 3D print parts that are assembled into a robotic arm exoskeleton (Figure 1). To facilitate this process, a 3D CAD model and an interface to the model was created. This interface is used to adjust the size of the printed device to fit a specific patient. Our rapid-prototyping process allows for exoskeletons to be easily and inexpensively fit to a patient by simply measuring and then procuring the correct size, similarly to buying shoes. When a person buys shoes, they simply go to the store, stand on a mat that measures their feet, and then buy the size that corresponds to their measurement. However, since the market for robotic exoskeletons is much smaller than the market for shoes, it is not economical for a large variety of sizes to be fabricated and kept in stock in order to meet the needs of each individual patient, which is where our rapid-prototyping process comes in. For our robotic exoskeleton, a patient visits a clinician who has our software and a 3D printer. Their arm, wrist, and hand are measured. The clinician types these measurements into our interface software and hits print. The 3D printer then prints the pieces, which takes about 7 hours and uses less than $1 of plastic. Then, the clinician assembles the pieces, which takes about 30 minutes. So, the patient could come back the next day to pick up their personalized exoskeleton which only cost the clinician about 1 hour of time, $1 of plastic, and 7 hours of powering the 3D printer.
Figure 3. RoboRockNRoll tablet game.
Our goals for our software were creating a variety of games to permit patients to select the game types they prefer, generating games that were enjoyable and habit-forming, constructing games with adjustable difficulty to engage participants at all levels of recovery, and providing different games to offer patients the option to switch programs when they become bored. These games facilitate therapeutic wrist exercises by using the custom fit exoskeleton as a video game controller, allowing the patients motions to control their game characters. To capture data associated with the range of motion of the patient’s wrist while doing exercises, a potentiometer is placed at the wrist joint of the exoskeleton and transferred via Bluetooth as a raw input to an interactive game system. The patient is then able to communicate with a computer solely by moving his/her wrist. Two games, RoboBlaster and RoboRockNRoll, were created for this purpose. In RoboBlaster, the user controllers a spaceship and destroys asteroids by shooting them with lasers (Figure 2). In RoboRockNRoll, the user controls a pick and catches music notes that correspond to popular songs that are being played during the gaming session (Figure 3). The mechanics for playing each of these games are the same. The patient moves their wrist up to move the character up and vice versa.
VALIDATION
Figure 4. Participants were engaged with a video game facilitated exercise session four times longer than they were with an unaided exercise session.
To validate the ability of the robotic exoskeleton and tablet gaming suite to increase engagement, 14 able bodied participants were asked to complete two tasks while wearing a robotic exoskeleton. For one of the tasks, the participants were asked to complete rehabilitative wrist exercises until they became bored. For the other task, the participants were asked to play the RoboBlaster tablet game, which encouraged the same rehabilitation wrist exercises, until they became bored. The participants were instructed that they could stop exercises anytime they wanted, which we associate with feeling boredom. Participants completed the two tasks in a random order. The amount of time that each participant participated in each activity before becoming bored was recorded. The results, shown in Figure 4, show that participants became bored four times faster when exercising without the tablet games. These values are statistically different with p < 0.01.
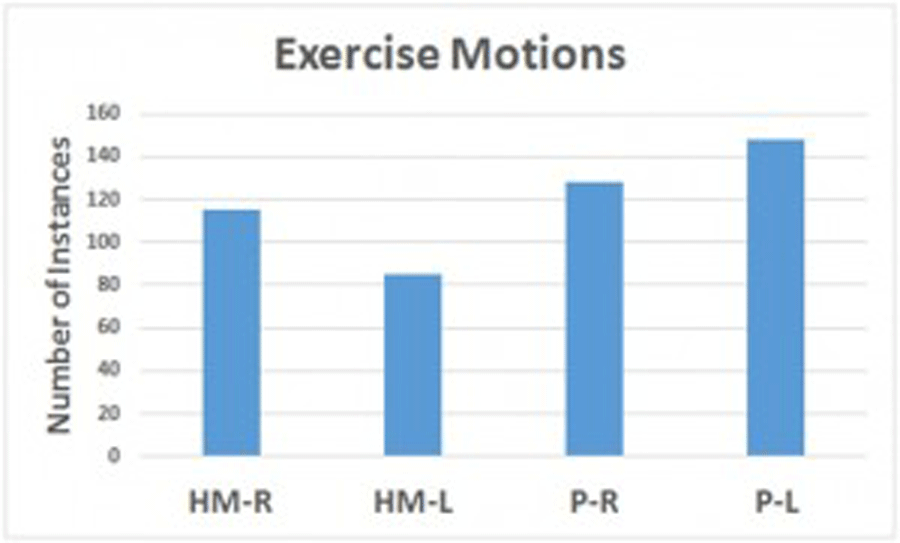
Figure 5. The amount of exercises that a participant was able to complete during 5 minute sessions with their arm suspended in the air with the HandMentor on their right arm (HM-R), Hand-Mentor on left arm (HM-L), prototype on right (P-R), and prototype on left (P-L).
To validate the increased comfort of a properly fitted robotic exoskeleton, we measured and 3D printed a custom fit robotic exoskeleton for one able bodied participant. The participant was asked to wear the custom fit robotic exoskeleton and repeatedly alternate between their maximum dorsiflexion and maximum palmarflexion points a comfortable speed for 5 minutes. The participant was asked to repeat this session with a commercially available one-size fits all robot, the HandMentor. The participant completed two sessions for each exoskeleton, one on the right arm and one on the left arm. During these sessions, the participant was asked to keep their arm 6 inches above the table, as marked on a poster board, while completing these exercises and to only take breaks when they were too tired to continue.
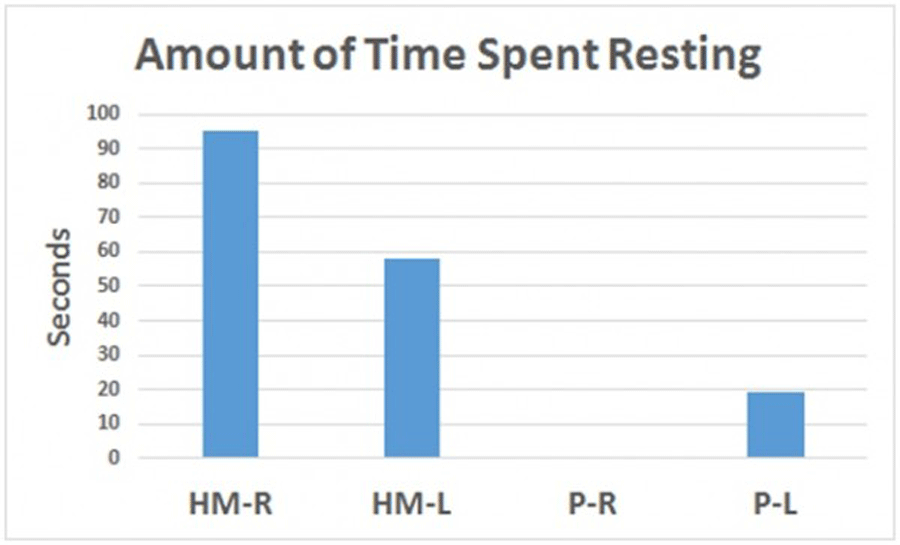
Figure 6. The amount of time that a participant spent resting during 5 minute exercise sessions with the HandMentor on their right arm (HM-R), Hand-Mentor on left arm (HM-L), prototype on right (P-R), and prototype on left (P-L).
Video was recorded of the participant during each session. The video was analyzed to count the number of exercise motions (defined by a motion from maximum palmarflexion to maximum dorsiflexion and back to maximum palmarflexion) and the amount of time the participant spent taking breaks during each session was recorded. As seen in Figure 5, the participant was able to complete more exercises with the custom fit prototype than the one size fits all HandMentor. This was partially due to the fact that the participant spent much less time taking breaks during the exercise sessions with the prototype, as seen in Figure 6, and partially because the participant was able to move at a faster pace due to being less encumbered by a large, heavy device. The participant was able to complete these exercises with the same range of motion with both robotic exoskeletons.
CONCLUSIONS AND FUTURE WORK
The developed system has been shown to increase engagement time by a factor of four with healthy subjects in the short term. The reduced weight and proper fit of the system was also shown to allow participants to have more productive exercise sessions by allowing them to complete more exercise motions and reduce the number of breaks that need to be taken. We plan to continue human subjects testing to include stroke and cerebral palsy patients to validate our results on the target users as well as in the long term.
REFERENCES
NINDS Cerebral Palsy Information Page. (2014) National Institute of Neurological Disorders and Stroke. National Institute of Health.
NINDS Stroke Information Page. (2014) National Institute of Neurological Disorders and Stroke. National Institute of Health.
Zimmerman, M.A., and S. Warschausky. (1998). Empowerment Theory For Rehabilitation Research: Conceptual And Methodological Issues. Rehabilitation Psychology, 43.1, 3-16.
(4) Dunn, D.S., and S.B. Dougherty. (2005). Prospects for a positive psychology of
Paolucci, S., et al. (2012). Impact Of Participation On Rehabilitation Results: A
Multivariate Study. European Journal Of Physical And Rehabilitation Medicine,
48.3, 455-466.
Nancy G. Kutner, Rebecca Zhang, Andrew J. Butler, Steven L. Wolf, Jay L.
Alberts. (2010). Quality-of-life change associated with robotic-assisted therapy to improve hand motor function in patients with subacute stroke: a randomized clinical trial. Physical therapy, 90.4, 493-504.
E. J. Koeneman, R. S. Schultz, S. L Wolf, D. E. Herring and J. B. Koeneman. (). A pneumatic muscle hand therapy device,” Proc., IEEE/EMBS Int, Conf, pp 2711-2713.
Colombo, R., Pisano, F., Mazzone, A., Delconte, C., Micera, S.,Carrozza, M., Dario, P., and Minuco, G. (2006). Design strategies to improve patient motivation during robot-aided rehabilitation. Journal of NeuroEngineering and Rehabilitation.
V. Squeri et al. (2014). Wrist rehabilitation in chronic stroke patients by means of adaptive, progressive robot-aided therapy. IEEE Transactions on Neural Systems and Rehabilitation Engineering, vol. 22, no. 2, pp. 312 – 325.
ACKNOWLEDGEMENTS
Thanks go to our faculty advisor, Dr. Ayanna M Howard for her guidance on this project. We would also like to thank Dr. Andrew Butler of Georgia State University for providing his insight on the use of rehabilitation robots for stroke survivors. We would like to thank Jill Auerbach, Julie Ridings, and the Opportunity Research Scholars (ORS) program at Georgia Tech for providing an undergraduate research experience that matched our team. This work was partially supported by the National Science Foundation under Grant 1208287, the ORS program, Intel, SRC, and Education Alliance. Any opinions, findings, conclusions, or recommendations expressed do not necessarily reflect the views of our sponsors.