Design and Evaluation of A Temperature Controlled air Cell based wheelchair cushion
David Smeresky1, Andrew Malkiewicz2, Patricia Karg1, David Brienza1
1Department of Rehabilitation Science & Technology, University of Pittsburgh, Pittsburgh, PA; 2Omnyx IDP, Pittsburgh, PA
Abstract
Skin protection wheelchair cushion design typically focuses on pressure redistribution and shear reduction. Elevated skin temperature is another known pressure ulcer risk factor, but few, if any, products are available capable of simultaneously controlling temperature at therapeutic levels and providing adequate pressure redistribution. Our project goal was to develop a cushion with this unique combination of performance specifications. A prototype was developed and evaluated. Evaluation included measurement of temperature and pressure using human subjects and ISO 16840-7 heat and water vapor dissipation testing. The prototype was able to consistently maintain the targeted temperature of 25°C on humans. ISO testing demonstrated the advantage of active temperature control. These results demonstrate the potential for this design concept to be used in an air-cell based wheelchair cushion to reduce pressure ulcer risk by preventing elevated skin temperature.
Introduction
Preventing pressure ulcers is critically important. Pressure ulcers are a costly and common condition with an annual cost of $1.68-6.8 billion per year.(Bader, Bouten, Colin, & Oomens, 2005) Among wheelchair users, pressure ulcers are exceptionally prevalent in individuals with spinal cord injury where there is a 33.5% chance of developing an ulcer and the rates increase with years post injury.(National Spinal Cord Injury Statistical Center, 2005) Individual’s health and function consequences can be devastating. While prevention strategies are necessarily multifaceted, a wheelchair user’s first line of defense is his or her cushion.
Sustained, external forces that deform soft tissue over bony prominences cause pressure ulcers in people in high-risk groups. Deformation can cause injury to tissue by reduction in blood flow (ischemia), disruption of cellular transport function, and inhibiting lymphatic flow. The primary function of a cushion is to redistribute pressure away from the bony prominences thereby reducing the deformation. Effective cushions allow the user to be immersed and enveloped to achieve an even distribution of forces, which has less tendency to deform the soft tissue. While sitting, the bony areas where deformation is often highest are the areas surrounding the ischial tuberosities (IT) and the sacrum.
Temperature is an important factor because it has a proportional relationship to metabolic rate and consumption of oxygen, the tissues’ most critical nutrient. (Ruch, Patton, Ruch, & Patton, 1965) Preventing an increase in skin temperature when it comes into contact with insulating cushioning materials can increase pressure tolerance. Kokate et al. found that when equivalent pressures were placed on the tissue, damage would occur in the higher temperature areas prior to the lower temperature areas.(Kokate et al., 1995) Skin surface temperatures in the range of 25-27°C protected the tissue from damage from forces that caused damage at higher temperatures.
Our goal was to implement temperature control in a wheelchair cushion design as a secondary preventive measure. Our biggest challenge was to achieve the temperature control in a design that also provided pressure redistribution as a primary preventive measure.
Design
Design Criteria

The general design criteria determined through this methodology can be summed up as temperature and treatment, integration and accommodation, and safety and robustness. While all of these goals are important in order for the final design to be considered a success, if the device is unable to maintain the therapeutic temperature of 25°C then the device will be of little use.
Design Iterations
The criteria chosen were then taken and integrated into the discussion and design process. Specifically the quality function deployment method was used in order to combine these criteria with integration of both group member specialties and client needs. (Eggert, 2005; Malkiewicz, 2006)

The water-cooled foam technology was based on circulating water controlled to a temperature between 15.5 and 25.6°C in flexible tubes embedded in the foam. (Malkiewicz, 2006) Various iterations of this design were attempted with the thickness of the foam cushioning material and the flexible tubing being adjusted.
We also considered an adaptation of established air cell based cushion technology. Air cell based cushions have been shown to manage pressure redistribution. (Brienza et al., 2010) We adapted a ROHO high profile cushion (ROHO Inc, Belleville, IL, USA) by inserting temperature controlled gel elements into the bottom of the air cells. Positioning the gel at the bottom of the cells and only in those cells near where the ischial tuberosities would protrude deeply into the cushions had the added advantage of only affecting temperature around the high-risk areas of the buttocks (Figure 1). The temperature of the gel inserts was controlled using thermoelectric cooling devices (TECs) on the bottom side and a proportional-integral-derivative (PID) control scheme with a thermistor inserted into the gel element. The gel temperature was maintained at 15°C to achieve and maintain 25°C at the interface.
Finalizing the Design
The foam and air cell based design were compared using human subjects in laboratory testing. These tests consisted of subjects sitting on the devices for 45 minutes on the foam cushion and 60 minutes on the air cell cushion. The air cell cushion was set up by overinflating the cushion, sitting the subject on the cushion and reducing the volume of air until cells near the ischial tuberosities collapsed to the point where the top rubber surface was in contact with the 12 mm thick gel elements. This is consistent with the recommended procedure for setting up a ROHO cushion.
Testing showed that the skin temperature for the subjects seated on the air cell cushion was maintained at 25°C for 60 min. (Figure 2) The water-cooled foam system was ineffective at maintaining the targeted temperature of 25°C. The air cell based design was selected for further development and evaluation.
Evaluation Methods and results
Pressure Redistribution Characterization
Pressure redistribution was characterized for the air cell cushion. Our modified cushion with temperature controlled gel inserts was compared to an unmodified high profile ROHO cushion. Two subjects sat on each device for five trials lasting five minutes each. Pressure was measured using a pressure mapping device (FSA, Vista Medical Ltd., Winnipeg, CA). Peak pressure index (PPI) was used for analysis. (Sprigle, Dunlop, & Press, 2003)
Pressure data was recorded at the end of the five minute test period. The results showed no significant difference in PPI between the modified and unmodified cushions (p = 0.77).
Heat Dissipation Characterization
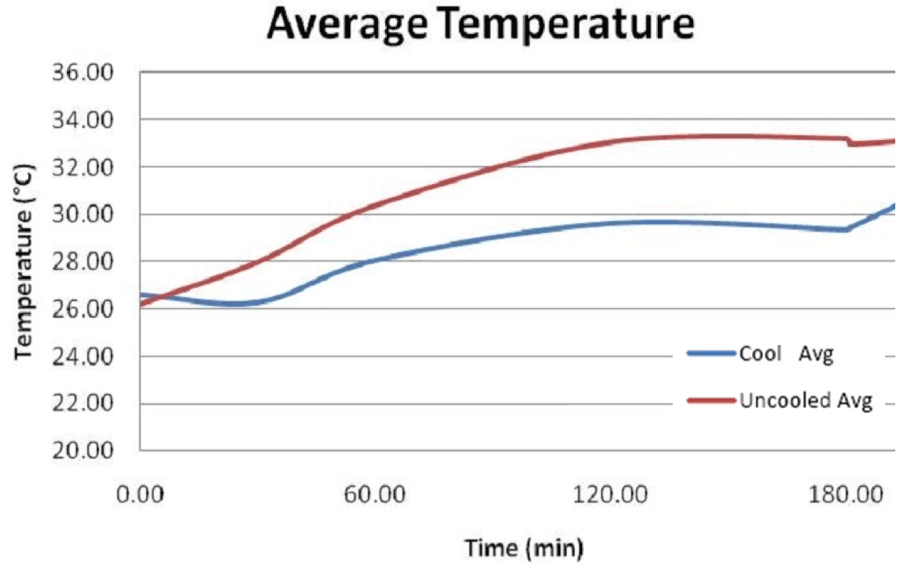
The final characterization test was for heat and water vapor transmission. ISO standard draft protocol (CD 16840-7 Wheelchair seating, The determination of heat and water vapor dissipation characteristics of seat cushions intended to manage tissue integrity) was used in this testing. (International Organization for Standardization, 2003) This testing was conducted on the air cell cushion with one side actively cooling and the other side not cooled. Testing occurred in a standardized environment of 23±2°C and 50% relative humidity and conducted over 3 hours and 15 minutes. Temperature and humidity data were recorded on the test jig’s two IT sensors at the following time intervals: 0, 30, 60, 120, 180, 181, and 196 minutes during the trials.
Statistical Methods
For all testing, normality was determined through the use of Kolmogorov-Smirnov tests and through graphing. The alpha for the study was chosen to be 0.05. The pressure data were analyzed using a two-tailed t-test. The heat and water vapor transmission testing was analyzed through the use of paired t-tests when data was normally distributed and the Wilcoxon signed rank test when data had nonparametric distributions.
Discussion and Summary
Our evaluation was aimed at choosing a temperature control technology and evaluating that technology to determine its ability to control temperature and redistribute pressure. With consideration to temperature we established that the air cell cushion with embedded temperature controlled gel elements was able to maintain skin temperature at the targeted 25°C.
The pressure and humidity were found to not be significantly different from an unmodified air cell cushion, suggesting that the modifications to the cushion would have minimal detrimental effects to the established desirable performance characteristics
References
Bader, D. L., Bouten, C., Colin, D., & Oomens, C. W. (2005). Pressure ulcer research: current and future perspectives: Springer.
Brienza, D., Kelsey, S., Karg, P., Allegretti, A., Olson, M., Schmeler, M., . . . Holm, M. (2010). A randomized clinical trial on preventing pressure ulcers with wheelchair seat cushions. Journal of the American Geriatrics Society, 58(12), 2308-2314.
Eggert, R. (2005). Engineering design: Pearson/Prentice Hall.
International Organization for Standardization. (2003). Wheelchair seating, in The determination of heat and water vapour dissipation characteristics of seat cushions intended to manage tissue integrity CD 16840-7. Geneva, Switzerland: International Organization for Standardization.
Kokate, J. Y., Leland, K. J., Held, A. M., Hansen, G. L., Kveen, G. L., Johnson, B. A., . . . Iaizzo, P. A. (1995). Temperature-modulated pressure ulcers: a porcine model. Archives of physical medicine and rehabilitation, 76(7), 666-673.
Malkiewicz, A. J. (2006). Development of a Wheelchair Seat Cushion With Site-Specific Temperature Control For Pressure Ulcer Prevention. University of Pittsburgh. Pittsburgh, PA.
National Spinal Cord Injury Statistical Center. (2005). Annual report for the model spinal cord injury care systems. Birmingham: National Spinal Cord Injury Statistical Center.
Ruch, R., Patton, H., Ruch, R., & Patton, H. (1965). Energy metabolism. Physiology and biophysics, 19th ed. Philadelphia, PA: Saunders Pr, 1064.
Sprigle, S., Dunlop, W., & Press, L. (2003). Reliability of bench tests of interface pressure. Assistive Technology, 15(1), 49-57.
Acknowledgements
This work was funded by the National Institute on Disability and Rehabilitation Research, Rehabilitation Engineering Research Center on Spinal Cord Injury at the University of Pittsburgh, Grant No. H133E070024.