The Effects of Grab bar presence on independent wheelchair transfer height and technique
Hailee Kulich1, 2, Sarah Bass1, 3, and Alicia M. Koontz, Ph.D, RET1, 3
- Human Engineering Research Laboratories, VA Pittsburgh Healthcare System, Pittsburgh, PA
- Department of Bioengineering, University of Pittsburgh, Pittsburgh, PA
- Department of Rehabilitation Science and Technology, University of Pittsburgh, Pittsburgh, PA
Abstract
The ability to transfer independently is an essential skill for wheeled mobility device users. However, improper transfer technique can lead to upper extremity pain and injury. Certain physical factors can facilitate transfers, improving transfer quality and accessibility. Grab bars have been shown to be helpful to wheeled mobility device users in the environment, but little research has been done on how grab bars affect the success of non-level transfers and the quality of transfers. The study enrolled 73 wheeled mobility device users who performed level, uphill, and downhill transfers in the absence and presence of grab bars. Attainable transfer height was found to be significantly higher and lower in the presence of grab bars (p<0.001 and p=0.015 respectively). Additionally, the presence of grab bars was found to significantly impact level, uphill, and downhill transfer quality (p=0.023, p=0.006, and p=0.024, respectively). The results of this study show that the presence of grab bars in the environment may improve accessibility and reduce the risk of developing upper limb injuries during both level and non-level transfers.
Introduction
For full time wheeled mobility device (WMD) users, the ability to perform transfers is an essential part of maintaining an active and independent lifestyle. Wheelchair users will perform on average between 15 and 20 sitting pivot transfers per day (Toro, Koontz, Cooper, 2013). Transferring has been shown to be one of the most physically demanding activities for WMD users (Koontz, Toro, Kankipati, Naber, Cooper, 2012). During transfer activities, individuals are supported partially or entirely by their upper extremities, increasing the internal forces applied to the shoulder, elbow, and wrist joints. Upper extremity joints are designed primarily for mobility, not stability, and the application of high forces in a repetitive manner due to transfer activities can impact long-term upper extremity health (Rice, Smith, Kelleher, Greenwald, Hoelmer, Boninger, 2013). For this reason, pain and overuse injuries from independent transferring are prevalent in WMD users. Transfer-related pain and injury can be detrimental for WMD users, leading to increased health care expenses, activity limitations, decreased community participation, and reduced quality of life (Koontz, Lin, Kankipati, Boninger, Cooper, 2011).
Transfer technique that reduces joint forces and moments may reduce upper extremity pain and injury. Poor transfer technique involves extreme combinations of shoulder flexion, rotation, and abduction (Rice, L. A., Smith, I., Kelleher, A. R., Greenwald, K., Hoelmer, C., & Boninger, M. L, 2013). Improper technique has also been shown to produce potentially dangerous angular displacement patterns in the shoulders, and elbows, as well as high vertical forces in the hands (Koontz, Lin, Kankipati, Boninger, Cooper, 2011). Previous research has shown that transferring with the trunk leaning forward, arms as close to the body as possible when weight lifting, wrists in a neutral position, and fingers flexed may reduce the risk of sustaining upper extremity injuries when transferring (Boninger, 2013). Safe transfer techniques reduce the moment and force distribution at the shoulders, the pressure in the carpal tunnel, and the vertical forces at the hands (Boninger, et al, 2005).
The Transfer Assessment Instrument (TAI) provides clinicians with an objective way to evaluate transfer quality. It can be used to identify dangerous techniques that may lead to upper limb pain or injury (Rice, L. A., Smith, I., Kelleher, A. R., Greenwald, K., Hoelmer, C., & Boninger, M. L, 2013). The TAI was designed to evaluate independent transfers and assesses several transfer aspects, including upper limb positioning and safety, WMD and body set up, and movement control. The TAI has been rigorously tested for validity and reliability on multiple levels (McClure, Boninger, Ozawa, Koontz, 2011), (Tsai, Rice, Hoelmer, Boninger, 2013).
While transfer technique is essential to preventing upper extremity injuries, physical factors may also affect transfer quality. Previous studies have indicated that transfer surface height, gaps, and obstacles may pose accessibility issues that impact transfer performance (Toro, Koontz, Cooper, 2013). Another physical factor that may affect the quality of transfer is the absence or presence of grab bars. Surprisingly few studies have been conducted to examine how grab bars affect wheelchair transfers (Koontz, Toro, Kankipati, Naber, Cooper, 2012). Prior research suggests that the presence of grab bars may aid in uphill and downhill transfers, which require more exertion due to increased ground reaction forces and muscle effort (Toro, Koontz, Cooper, 2013). Grab bars may also reduce the forces at the hand and wrists, reducing the risk of wrist impairments and increasing the quality of the transfer (Boninger, 2013). The purpose of this study was 1) to determine how the presence or absence of grab bars affects attainable transfer heights during uphill and downhill transfers and 2) to determine how the presence or absence of grab bars affects transfer quality, as defined by the TAI. Findings from this study will help to define the relationship between grab bar presence and transfer ability and quality.
METHODS
Subjects
The study received approval from the University of Pittsburgh’s Institutional Review Board. Seventy three subjects were recruited for the study and signed informed consent forms before any testing procedures occurred. Inclusion criteria were defined as: 1) owning a wheeled mobility device 2) using the wheeled mobility device for at least one year prior to the study 3) eighteen years or older and 4) the ability to independently transfer with or without a transfer board. Subjects were excluded from the study if they had active pressure sores, had a history of pressure sores, and if they had pain or injury to their arms that would affect transfer ability.
Experimental Protocol
 Figure 1: Transfer station set up
Figure 1: Transfer station set up
Subjects were asked to perform transfers from their personal wheeled mobility device to a custom- designed transfer station, as seen in Figure 1. The station was able to raise and lower via hydraulic scissor lift. Subjects were able to position their wheelchair next to the station in the orientation that they felt most comfortable. A successful transfer was defined as an unassisted transfer from the wheeled mobility device to the platform and then back to the wheeled mobility device.
 Figure 2: Transfer station set up with grab bars
Figure 2: Transfer station set up with grab bars
Two separate protocols were performed: a set of transfers where grab bars were absent and a set of transfers where grab bars were present. For each grab bar protocol, two grab bars were placed on each side of the seat. Figure 2 shows the transfer station with grab bars.
Subjects were given a choice between using 6 and 2.75 inch grab bars. Figure 3 shows the two types of grab bars. The 6 inch grab bar was based on American Disabilities Act (ADA) standards while the 2.75 inch bar was based on a recommendation by the United States Access Board. Grab bars had circular handles with a diameter of 1.25 inches to reflect current ADA standards.
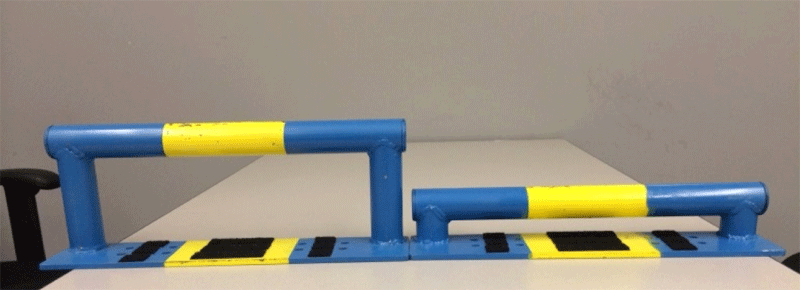 Figure 3: 6 inch (left) and 2.75 inch (right) grab bars
Figure 3: 6 inch (left) and 2.75 inch (right) grab bars
For each grab bar condition (e.g. no grab bars or with grab bars) three transfers were performed to the platform at level with the wheelchair user's seat to floor height, uphill, and downhill. For the uphill and downhill transfers, the platform was raised or lowered depending on the subject’s ability and transfer skills. After an uphill or downhill transfer, the subjects were asked if they could do a higher or lower transfer, with three attempts to reach their maximum and minimum transfer height. The maximum differences in heights obtained were recorded. During transfers, the TAI was completed for all the transfers by a trained clinician who was blinded to the study goals. One TAI score was completed for each type of transfer (e.g. level, uphill and downhill).
Data Analysis
Relative transfer heights were obtained for uphill and downhill transfers by subtracting the subject’s seat to floor height from the absolute maximum and minimum transfer heights. TAI score calculations were made for level, uphill, and downhill transfers. Scoring consists of two parts. During the first part, the transfer is broken down into components that make up good transfer technique, and each component is evaluated separately. Part one consists of 15 items, scored with a “Yes”, “No”, or “Not applicable”. “Yes” received a score of one, “No” a zero, and “Not applicable” removes the item from the final calculation. The second part looks at the transfer as a whole, grading on quality, technique, and safety of the transfer. Part two consists of 12 items and is scored on a scale of zero to four, where four represents “strongly agree” and zero represents “strongly disagree”. The final TAI score is an average of part one and part two scores. The calculation for the TAI score can be seen in Figure 4. The TAI score ranges from zero to ten, where ten indicates the best quality transfer possible and zero indicates the worst quality transfer possible.
A paired t-test was performed to examine intra-subject changes for both the relative height of transfer and the TAI scores. Values were grouped by grab bar condition (presence or absence) as well as transfer type (level, uphill, or downhill). All statistical analysis was performed using SPSS Version 21 (SPSS Inc, Chicago). The level of significance was set at a p-value of 0.05 or less.
RESULTS
Of the 73 subjects enrolled in the study, 1 was withdrawn due to being unable to independently transfer to the platform. The remaining 72 subjects consisted of 55 males and 17 females. The average age, weight, and height of participants (± standard deviation) were 45.2 ± 15.1 years, 174.2 ± 53.2 pounds, and 67.2 ± 5.7 inches, respectively. The average reported level and non-level transfers performed per day were 11.6 ± 14.1 and 8.3 ± 14.3 respectively. The study included 46 manual chair, 19 power chair, 3 scooter, and 4 manual power assist users. Participants had a wide range of disabilities, including but not limited to spinal cord injury, amputation, spina bifida, multiple sclerosis, and cerebral palsy. When given a choice between grab bars, 76.1% of subjects chose 6 inch grab bars while the remaining 23.9% chose 2.75 inch grab bars.
The mean, maximum, and minimum relative transfer heights for uphill and downhill transfers for the protocol without grab bars and the protocol with grab bars (± standard deviation) can be seen in Table 1, where relative transfer height is the difference in WMD floor to seat height and maximum or minimum attainable transfer height. Subjects could transfer significantly higher and lower with the presence of grab bars, with p<0.001 and p=0.015 respectively.
| Uphill Transfer | Downhill Transfer | |||
|---|---|---|---|---|
| Grab bars absent | Grab bars present | Grab bars absent | Grab bars present | |
| Mean (in) | 6.72 ±3.98 | 7.41 ±4.32 | 7.70 ±4.16 | 8.38 ±3.97 |
| Max (in) | 21.50 | 21.50 | 14.0 | 14.0 |
| Min (in) | 0.50 | 0.50 | 0.50 | 1.00 |
| p-value | <0.001* | 0.015* | ||
The average Part 1 TAI scores for level, uphill, and downhill transfers for the protocol without grab bars and the protocol with grab bars (± standard deviation) can be seen in Table 2. Part 1 TAI scores improved significantly for all protocols when grab bars were on the station compared to when no grab bars were present, with p-values of p=0.040, p=0.012, and p=0.024 for level, uphill, and downhill transfers respectively.
| Level | Uphill | Downhill | ||||
|---|---|---|---|---|---|---|
| Grab bars absent | Grab bars present | Grab bars absent | Grab bars present | Grab bars absent | Grab bars present | |
| Mean | 6.80 ±1.79 | 7.08 ±1.78 | 6.73 ±1.87 | 7.09 ±1.74 | 6.85 ±1.94 | 7.12 ±1.73 |
| Max | 10.00 | 10.00 | 10.00 | 10.00 | 10.00 | 10.00 |
| Min | 2.50 | 2.50 | 2.50 | 2.50 | 2.50 | 2.50 |
| p-value | 0.040* | 0.012* | 0.024* | |||
The average total TAI scores for level, uphill, and downhill transfers for the protocol without grab bars and the protocol with grab bars (± standard deviation) are shown in Table 3. TAI scores improved significantly when grab bars were added to the station, with values of p=0.023, p=0.006, and p=0.024 for changes in level, uphill, and downhill TAI Scores.
| Level | Uphill | Downhill | ||||
|---|---|---|---|---|---|---|
| Grab bars absent | Grab bars present | Grab bars absent | Grab bars present | Grab bars absent | Grab bars present | |
| Mean | 7.15 ±1.61 | 7.43 ±1.55 | 6.99 ±1.67 | 7.34 ±1.54 | 7.09 ±1.69 | 7.38 ±1.56 |
| Max | 9.55 | 10.00 | 9.55 | 9.40 | 9.55 | 9.41 |
| Min | 2.68 | 3.54 | 2.68 | 3.25 | 2.68 | 3.54 |
| p-value | 0.023* | 0.006* | 0.024* | |||
DISCUSSION
The results of this study indicate that WMD users can transfer significantly higher and lower with the presence of grab bars. Previous studies have shown that height differentials of more than 2 inches can pose serious accessibility issues in regards to transfers (Toro, Koontz, Cooper, 2013). Our study suggests that for individuals who have difficulty with uphill transfers, adding grab bars may make a difference in being able to access or not access a surface. Changes in height between protocols were statistically significant although the mean group differences between grab bar use and non-use were small (<1 inch). While the benefits may not be as evident when looking at the population as a whole, larger differences were observed on an individual level. Therefore, the presence of grab bars may improve accessibility for some WMD users for non-level transfers. Non-level transfers are a common activity for WMD users, specifically for those who do not have adjustable seating options. While they are less than ideal, non-level transfers are often unavoidable, especially in the community where the environment cannot be customized to one particular wheeled mobility device height. An increase in the amount of grab bars available in the community to WMD users may allow for increased participation in work, recreational and social activities.
The study also shows that the presence of grab bars improves transfer quality for level, uphill, and downhill transfers. Similar to the changes observed with height, differences in the TAI mean scores were small (<1 point) however, larger individual differences were observed. By improving quality, the presence of grab bars in the environment has the potential to reduce transfer-related injuries to the upper extremities, especially during non-level transfers. All transfers produce exceptionally high muscle forces in the upper extremities. However, transfers to non-level surfaces produce higher muscle forces in the arms and shoulders than transfer to level surfaces, increasing risk of pain and injury (McClure, Boninger, Ozawa, Koontz, 2011). The TAI data suggests that grab bars may promote a more biomechanically favorable arm position regardless of transfer height. Grab bars may help subjects to keep their arms close to their body and position their wrists and fingers in a more flexed position. This effect is most evident in Part 1 of the TAI Score, which breaks down the transfer into small components, specifically focusing on transfer biomechanics and upper limb positioning. All transfer types showed significant change in Part 1 scores, indicating that the safety and biomechanics of each transfer type was improved with the presence of grab bars. By significantly improving upon the unfavorable positioning that level, uphill, and downhill transfers create on the upper extremities, the presence of grab bars may allow for increased safety and reduced risk of injury for both level and non-level transfers.
Limitations and Future Work
In general, the subjects that participated in the study had excellent transfer technique, with average TAI scores of approximately 7 out of 10. High TAI Scores may have resulted in ceiling effects. The transfer station had a minimum height of 10 inches above the ground. Several subjects were able to easily transfer to the minimum height of the transfer station. The grab bars used during this study were only placed in one position on the transfer station. Several participants commented that while grab bars are helpful, they can either help or hinder transfer ability depending on placement. Future studies may want to examine how positioning of grab bars on or near a transfer surface affects transfer ability.
CONCLUSION
The study found that the presence of grab bars allows for WMD users to successfully transfer to higher and lower surfaces than in the absence of grab bars. Additionally, the study demonstrated that individual transfer technique improves with the presence of grab bars for level, uphill, and downhill transfers, as indicated by TAI score. As a result, adding grab bars in the environment may improve accessibility and safety issues during both level and non-level transfers for WMD users.
REFERENCES
Boninger, M.L., et al. (2005). Preservation of upper limb function following spinal cord injury: a clinical practice guideline for health-care professionals. J Spinal Cord Med, 28(5): p. 434-70.
Koontz, AM, Lin, YS, Kankipati, P, Boninger, ML, & Cooper, RA. (2011) Development of custom measurement system for biomedical evaluation of independent wheelchair transfers. J Rehabil Res Dev. 48(8), 1015-28. doi:10.1682/JRRD.2010.09.0169
Koontz, AM. Toro, M. Kankipati, P. Naber, M. & Cooper, RA (2012). An expert review of the scientific literature on independent wheelchair transfers. Disabil Rehabil Assist Technol, 7(1), 20-29. doi: 10.3109/17483107.2011.553983
Rice, L. A., Smith, I., Kelleher, A. R., Greenwald, K., Hoelmer, C., & Boninger, M. L. (2013). Impact of the Clinical Practice Guideline for Preservation of Upper Limb Function on Transfer Skills of Persons with Acute Spinal Cord Injury. Arch Phys Med Rehabil. doi: S0003-9993(13)00240-2
Toro, ML., Koontz, AM., & Cooper, RA. (2013). The Impact of Transfer Set up on the Performance of Independent Wheelchair Transfers. Hum. Factors. 55, 567-80. Doi: 10.1177/0018720812460549.
Tsai, CY., Rice, LA., Hoelmer, C., Boninger,ML. & Koontz, AM. (2013). Basic Psychometric Properties of the Transfer Assessment Instrument. Arch Phys Med
ACKNOWLEDGMENTS
Funding for this study was provided by the National Science Foundation, ASPIRE Grant #1262670 and the Department of Education (NIDRR), United States Access Board grant H133E070024 and Project #84.133E. The contents of this paper do not represent the views of the Department of Veterans Affairs or the United States Government.