Differences in the Upper Limb Mechanical Demands between Wheelchair to Bench and Bench to Wheelchair Sitting-Pivot Transfers
Lin Wei, Chung-Ying Tsai, Sarah R. Bass, and Alicia M. Koontz
Human Engineering Research Laboratories, VA Pittsburgh Healthcare System, University of Pittsburgh, Pittsburgh, PA 15206, USA
Department of Rehabilitation Science and Technology, University of Pittsburgh, Pittsburgh, PA 15260, USA
Abstract
The mechanical loads generated during wheelchair transfers predispose wheelchair users to upper limb joint pain and injuries. All the transfer biomechanics research to date focuses on describing one-directional transfers (e.g. wheelchair to a target surface). The purpose of the current study is to compare the mechanical joint loads on the shoulder, elbow, and wrist between a wheelchair-to-bench (WC-B) and bench-to-wheelchair (B-WC) transfer. Fifteen full time wheelchair users performed sitting pivot transfers to and from a level-height bench and personal wheelchair while a series of forces plates, load cells, and a motion capture system recorded the biomechanics of their natural transfer techniques. The trailing arm supported significantly more peak joint force and moment during the B-WC transfer (p < .001). Transfers back to the wheelchair may be more detrimental to the upper extremities than transfers out of the wheelchair due to the greater mechanical loads placed on the trailing arm.
Introduction
The number of people using wheelchairs for mobility is expanding each year. There were about 1.6 million people living with a spinal cord injury in 2010 (National Spinal Cord Injury Statistical, 2010). Persons with lower limb paralysis rely on their upper extremities to lift and transfer their body for the completion of activities of daily living (ADLs) (Fliess-Douer, Vanlandewijck, & Van der Woude, 2012). A full-time wheelchair user will perform on average 14 to 18 transfers per day (Finley, McQuade, & Rodgers, 2005). During the performance of transfers, the wheelchair user often applies excessive loads on their arms, leading to upper extremity pain and injuries (Finley & Rodgers, 2004). Extreme combinations of shoulder flexion, internal rotation, and abduction are known to create high internal joint forces and are difficult to avoid during transfers (Gagnon, Nadeau, Noreau, Dehail, & Piotte, 2008). The high superior forces generated during transfer are believed to contribute to pain and secondary impairments at the elbow (Koontz, Lin, Kankipati, Boninger, & Cooper, 2011). Moreover, the extreme wrist extension angles and forces generated during transfers may increase the pressure of carpal tunnel and exacerbate carpal tunnel syndrome (Keir, Wells, Ranney, & Lavery, 1997; Sie, Waters, Adkins, & Gellman, 1992).
The previous studies on transfers have described mechanical loading for one directional transfers such as from a wheelchair to a platform bench (Koontz, Kankipati, Lin, Cooper, & Boninger, 2011) (Tsai, Hogaboom, Boninger, & Koontz, 2014) or transfers between two platform surfaces (Finley et al., 2005) (Gagnon et al., 2008). The differences in upper limb loading when moving to a platform versus moving to a wheelchair are largely unknown. The transfer back to the wheelchair involves landing on a target surface (e.g. cushion) that may be smaller, softer, and harder to navigate (due to obstacles in the way such as arm rests or the rear wheel) than when moving to a platform bench or similar type of surface.
The purpose of this study is to compare the joint forces and moment on the upper extremities between WC-B and B-WC transfers. We hypothesized that a wheelchair user sustains larger maximum resultant joint loads on the shoulders, elbows, and wrists when preforming B-WC transfer compared to when performing a WC-B transfer.
Methods
Participation
The study was approved by the Department of Veterans Affairs Institutional Review Board. All testing occurred at the Human Engineering Research Laboratories in Pittsburgh, PA. Each subject met the following inclusion criteria: (1) older than 18 years old, (2) one year after injury or diagnosis, (3) use a wheelchair for at least 40 hours/week, and (4) unable to stand up without support. The exclusion criteria were (1) pressure sores within the past year, (2) history of angina or seizures.
Texting Protocol
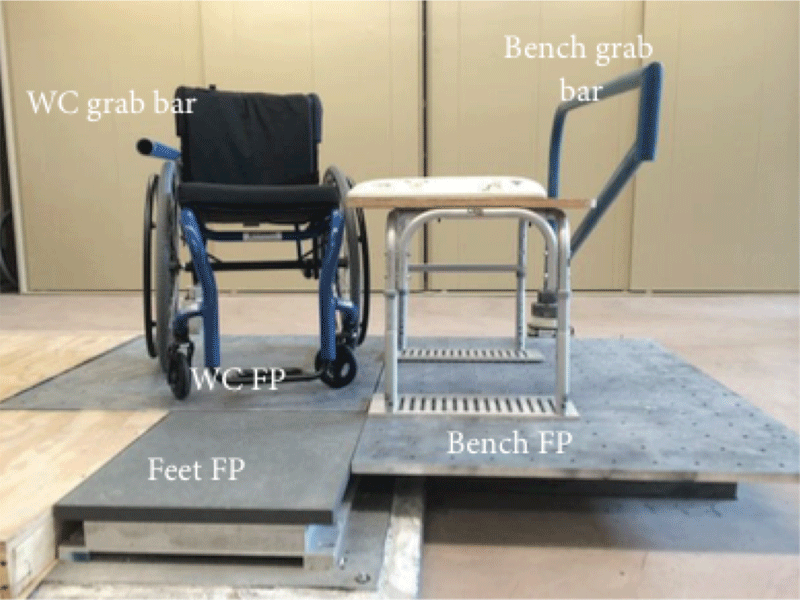
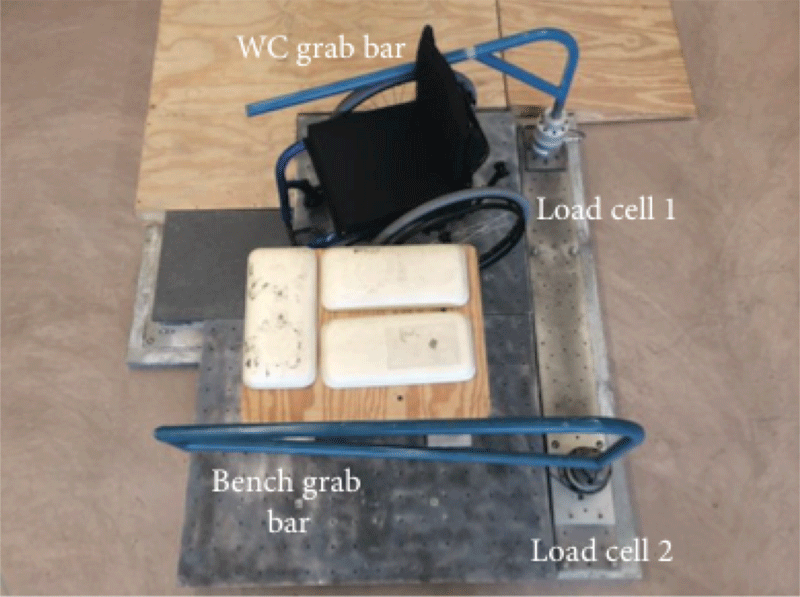 Figure 1: Front (top) and top (bottom) views of the transfer station. WC: wheelchair; FP: force plate.
Figure 1: Front (top) and top (bottom) views of the transfer station. WC: wheelchair; FP: force plate.
After subjects provided informed consent, subjects were asked to naturally position themselves next to a bench, which was set at a height level to their own wheelchair seats on a custom-built transfer station (Figure 1) (Koontz, Lin, et al., 2011). There were three force plates in the transfer station under the wheelchair, level bench, and subject’s feet, respectively. Their wheelchairs were secured onto a 3x3 square foot (91.44 cm by 91.44 cm) aluminum platform that covered the wheelchair force plate. The subjects were asked to choose where they wanted to position their wheelchair and bench on the other 3x4 square foot aluminum platform (91.44 cm by 121.92 cm) that covered the bench force plate (Figure 1). The station also contained two 6-component load cells (Model MC5 from AMTI, Watertown, MA; Model Omega 160 from ATI, Apex, NC) attached to two steel beams used to simulate an armrest and grab bar (Figure 1).
The position of the grab bar was also adjusted based on the subjects’ preferences.
Subjects were asked to perform up to five trials of level-height bench transfers to and from their own wheelchairs in a natural way. They were provided an opportunity to adjust their wheelchair position and familiarize themselves with the setup prior to data collection. Subjects had time to rest in between trials and additional rest was provided as needed. They were asked to use their own approaches to transferring so their transfer movement pattern and techniques would be as natural as possible. Subjects were asked to use the wheelchair grab bar (Figure 1) when they transferred to and from the bench so the reaction forces at the hand could be accurately recorded on the wheelchair side.
Reflective markers were placed on subjects’ heads, trunks, and upper extremities to build local coordinate systems (Wu et al., 2005) for each segment. The moving trajectories of the markers during transfer were collected at 100 Hz using a ten-camera three-dimensional motion capture system (Vicon, Centennial, CO.) Kinetic data from all the force plates and load cells were collected at 1000 Hz.
Data analysis
The biomechanical variables were computed using MATLAB (Mathworks, Inc., Natick, MA, USA). A zero-lag low-pass 4th order Butterworth filter with cutoff frequency of 7 and 5 Hz was used to filter the kinetic and kinematic data, respectively (Koontz, Kankipati, et al., 2011). A transfer was determined to begin when a vertical reaction force was detected by the load cell on the wheelchair side grab bar (Figure 1) for both the WC-B and B-WC transfers. The transfer ended before a landing spike was detected by the force plate underneath the bench (WC-B transfer) or the wheelchair (B-WC transfer). Hanavan’s model was used to calculate center of mass and moment of inertia using the subjects’ segment lengths and circumferences (Hanavan, 1964). Three-component forces and moments measured by the load cells and the force plates (Figure 1), the marker data of the trunk and upper extremities, and the inertial properties of each body segment were inputs into an inverse dynamic model (Cooper, Boninger, Shimada, & Lawrence, 1999). Each segment was assumed as a rigid body and linked together by the inverse dynamic model included upper extremity net joint forces and moments. The kinetic variables included maximum resultant forces and moments at the shoulders, elbows, and wrists on the leading (left arm in the WC-B and right arm in the B-WC transfer) and trailing (right arm in the WC-B and left arm in the B-WC transfer) sides. Each kinetic variable was normalized by body mass (in kilogram) (Gagnon et al., 2008) (Desroches, Gagnon, Nadeau, & Popovic, 2013). Descriptive statistics (means and standard deviations (SD)) were calculated for each variable. Kinetic variables were averaged over a minimum of three and a maximum of five trials. A paired t-test was used to compare the kinetic variables between the WC-B and B-WC transfers on the leading arm and trailing arm. The level of significance was set to 0.05. All the statistical analyses were performed in SPSS 21 (SPSS Inc., Chicago, IL).
Results
| Subjects, n=15 | Mean ± standard deviation (range) |
|---|---|
| Age (years) | 37.34±11.26 (21-55) |
| Height (m) | 1.65±0.28 (0.99-2.03) |
| Weight (kg) | 68.61±18.64 (29.96-95.93) |
| BMI (kg/m2) | 26.62±11.71 (17.51-65.46) |
| Average duration of WC use (years) | 14.99±8.56 (2-27) |
Participants
Fifteen subjects including fourteen men and one woman participated in this study (Table 1). Twelve subjects had a spinal cord injury (SCI); eight subjects reported a complete SCI and four subjects an incomplete SCI (three with American Spinal Injury Association (ASIA) Grade B, one with ASIA Grade C). Three subjects had tetraplegia (C4 to C6), five had high paraplegia (T2 to T7), and five had low paraplegia (T8 to L3) (John, Cherian, & Babu, 2010). The remaining three participants had double above knee amputation (𝑛 = 1), osteogenesis imperfecta (𝑛 = 1), and myelopathy (𝑛 = 1).
Kinetic Variables
Maximum resultant joint moments on the leading arm were significantly lower at the shoulder and higher at the elbow during the B-WC transfer compared to the WC-B transfer (Table 2; p ≤ .012). Higher maximum resultant joint forces and moments occurred at the trailing shoulder, elbow and wrist during the B-WC transfer compared to the WC-B transfer (Table 3; p < .001).
Discussion
| Leading Arm | |||||
| Joint Section | Direction |
Max Resultant Force (N/kg) |
Max Resultant Moment (Nm/kg) |
||
|---|---|---|---|---|---|
Mean (± SD) |
p-value |
Mean (± SD) |
p-value |
||
Shoulder |
W-BC |
4.33 (± 1.02 ) |
0.548 |
1.03 (± 0.24 ) |
0.006 |
B-WC |
4.09 (± 1.34 ) |
0.78 (± 0.31 ) |
|||
Elbow |
W-BC |
4.32 (± 1.06 ) |
0.293 |
0.38 (± 0.10 ) |
0.012 |
B-WC |
3.90 (± 1.30 ) |
0.58 (± 0.21 ) |
|||
Wrist |
W-BC |
4.33 (± 1.08 ) |
0.232 |
0.28 (± 0.15 ) |
0.611 |
B-WC |
3.84 (± 1.30 ) |
0.31 (± 0.12 ) |
|||
The B-WC transfer is the most common type of transfer performed daily. Wheelchair users transfer from their wheelchair to a variety of surfaces over the course of a day (e.g. commode seats, car seats, couches, bed, floor, etc.) but always transfer back into their wheelchair in between tasks. Our study shows that unfortunately transfers back into the wheelchair may be the most detrimental to the upper extremities due to the greater mechanical load placed on the trailing arm and to a lesser degree the leading arm.
The primary reason for the increased joint loads in the trailing arm during the B-WC is likely due to an increased difficulty in navigating the body back into a wheelchair versus moving it onto a flat ‘hard’ surface. The bench used in this study may have been easier to move to because it had a larger landing area and a firmer surface than the seat and cushion used in a user’s wheelchair. The rear wheel or other parts of the wheelchair frame may also hinder the ability to navigate the trunk and buttocks back into the wheelchair seat. The major function of the trailing arm is to help maintain dynamic balance and support the upper body and trunk while it pivots about the feet. More force would be required by the trailing arm to balance and maneuver the body during the B-WC transfer under the additional constraints presented on the wheelchair side of the equation. The general impact of surface related factors such as firmness, positioning and size of the area on transfer performance and mechanical loading are poorly understood. Our study suggests that wheelchair characteristics may influence the loading and interventions such as alternative wheelchair designs that facilitate the transfer process should be investigated in future work.
| Trailing Arm | |||||
| Joint Section | Direction | Max Resultant Force (N/kg) | Max Resultant Moment (Nm/kg) | ||
|---|---|---|---|---|---|
| Mean (± SD) | p-value | Mean (± SD) | p-value | ||
| Shoulder | W-BC | 4.37 (± 1.14 ) | <0.001 | 0.76 (± 0.38 ) | <0.001 |
| B-WC | 8.49 (± 0.79 ) | 1.74 (± 0.48 ) | |||
| Elbow | W-BC | 4.18 (± 1.12 ) | <0.001 | 0.54 (± 0.21 ) | <0.001 |
| B-WC | 8.43 (± 0.78 ) | 1.39 (± 0.41 ) | |||
| Wrist | W-BC | 4.12 (± 1.12 ) | <0.001 | 0.34 (± 0.10 ) | <0.001 |
| B-WC | 8.41 (± 1.78 ) | 0.62 (± 0.18 ) | |||
and trailing arm sides carry equal amounts of loading (Koontz, Kankipati, et al., 2011). A similar high degree of imbalance in the moments across the elbow and wrist joints occurred with the B-WC transfer as well when compared to the WC-B transfer.
One of the limitations of our study is that a majority of subjects were men. Also while we tried to provide an environment that mimicked transfers in a realistic sense, subjects were limited on the wheelchair side to where to place their hand so that accurate force readings could be obtained.
CONCLUSIONS
The results demonstrate that wheelchair users sustain greater maximum resultant joint loads at the shoulder, elbow, and wrist loads when performing a level transfer to a wheelchair than when performing a level transfer to a bench. The results provide evidence to support the innovation of new wheelchair designs that help make transfers easier or movement strategies (such as alternative hand and feet placement) that help to balance the joint loading better during transfers back into the wheelchair.
References
Cooper, R. A., Boninger, M. L., Shimada, S. D., & Lawrence, B. M. (1999). Glenohumeral joint kinematics and kinetics for three coordinate system representations during wheelchair propulsion. Am J Phys Med Rehabil, 78(5), 435-446.
Desroches, G., Gagnon, D., Nadeau, S., & Popovic, M. R. (2013). Effects of sensorimotor trunk impairments on trunk and upper limb joint kinematics and kinetics during sitting pivot transfers in individuals with a spinal cord injury. Clin Biomech (Bristol, Avon), 28(1), 1-9. doi: 10.1016/j.clinbiomech.2012.11.001
Finley, M. A., McQuade, K. J., & Rodgers, M. M. (2005). Scapular kinematics during transfers in manual wheelchair users with and without shoulder impingement. Clin Biomech (Bristol, Avon), 20(1), 32-40. doi: 10.1016/j.clinbiomech.2004.06.011
Finley, M. A., & Rodgers, M. M. (2004). Prevalence and identification of shoulder pathology in athletic and nonathletic wheelchair users with shoulder pain: A pilot study. J Rehabil Res Dev, 41(3B), 395-402.
Fliess-Douer, O., Vanlandewijck, Y. C., & Van der Woude, L. H. (2012). Most essential wheeled mobility skills for daily life: an international survey among paralympic wheelchair athletes with spinal cord injury. Arch Phys Med Rehabil, 93(4), 629-635. doi: 10.1016/j.apmr.2011.11.017
Gagnon, D., Nadeau, S., Noreau, L., Dehail, P., & Piotte, F. (2008). Comparison of peak shoulder and elbow mechanical loads during weight-relief lifts and sitting pivot transfers among manual wheelchair users with spinal cord injury. J Rehabil Res Dev, 45(6), 863-873.
Hanavan, E. P., Jr. (1964). A Mathematical Model of the Human Body. Amrl-Tr-64-102. AMRL TR, 1-149.
John, L. T., Cherian, B., & Babu, A. (2010). Postural control and fear of falling in persons with low-level paraplegia. J Rehabil Res Dev, 47(5), 497-502.
Keir, P. J., Wells, R. P., Ranney, D. A., & Lavery, W. (1997). The effects of tendon load and posture on carpal tunnel pressure. J Hand Surg Am, 22(4), 628-634. doi: 10.1016/S0363-5023(97)80119-0
Koontz, A. M., Kankipati, P., Lin, Y. S., Cooper, R. A., & Boninger, M. L. (2011). Upper limb kinetic analysis of three sitting pivot wheelchair transfer techniques. Clin Biomech (Bristol, Avon), 26(9), 923-929. doi: 10.1016/j.clinbiomech.2011.05.005
Koontz, A. M., Lin, Y. S., Kankipati, P., Boninger, M. L., & Cooper, R. A. (2011). Development of custom measurement system for biomechanical evaluation of independent wheelchair transfers. J Rehabil Res Dev, 48(8), 1015-1028.
National Spinal Cord Injury Statistical, C. (2010). Spinal cord injury facts and figures at a glance. J Spinal Cord Med, 33(4), 439-440.
Sie, I. H., Waters, R. L., Adkins, R. H., & Gellman, H. (1992). Upper extremity pain in the postrehabilitation spinal cord injured patient. Arch Phys Med Rehabil, 73(1), 44-48.
Tsai, C. Y., Hogaboom, N. S., Boninger, M. L., & Koontz, A. M. (2014). The relationship between independent transfer skills and upper limb kinetics in wheelchair users. Biomed Res Int, 2014, 984526. doi: 10.1155/2014/984526
Wu, G., van der Helm, F. C., Veeger, H. E., Makhsous, M., Van Roy, P., Anglin, C., . . . International Society of, B. (2005). ISB recommendation on definitions of joint coordinate systems of various joints for the reporting of human joint motion--Part II: shoulder, elbow, wrist and hand. J Biomech, 38(5), 981-992.