VISUAL COGNITIVE PROCESSING DEMANDS OF ABC AND QWERTY ONSCREEN KEYBOARDS: A PRELIMINARY INVESTIGATION OF INDIVIDUALS WITH SCI/TBI AND TYPICAL INDIVIDUALS
Susan Koch Fager PhD CCC-SLP, Jessica Gormley MS CCC-SLP, David R. Beukelman PhD CCC-SLP
Institute for Rehabilitation Science & Engineering, Madonna Rehabilitation Hospital, Lincoln, NE
ABSTRACT
Individuals who have sustained a spinal cord injury (SCI) and traumatic brain injury (TBI) may be offered a range of onscreen keyboard interfaces to generate text using assistive technologies to support home, vocational, educational, and medical communication needs. Limited objective information is available regarding the visual-cognitive processing demands of different onscreen keyboard interfaces to guide clinicians in the recommendations of these interfaces. This preliminary investigation examines the visual-cognitive processing demands of using an ABC and QWERTY onscreen keyboard accessed with a standard mouse by individuals who have sustained a SCI/TBI and typical individuals (with no neurologic impairment). Results indicate differences in the visual-cognitive processing demands between the two keyboards in that the QWERTY keyboard had lower fixation counts and fixation durations for all participants. All participants reported extensive experience with QWERTY onscreen keyboards through their personal smart phones. Additionally results indicate potential differences in the way that individuals with acquired injuries visually process interfaces compared to typical individuals warranting future research to better understand the impact of neurologic injuries on visual-cognitive processing.
Keywords: Onscreen keyboards, assistive technology, visual-cognitive processing demands, eye tracking
BACKGROUND
After acquired injuries, many literate individuals who require augmentative and alternative communication (AAC) and assistive technology to support communication, use onscreen keyboards in their specialized communication software to generate text (Beukelman & Mirenda, 2013; Britton & Baarslag-Benson, 2007; Fager, Doyle, & Karantounis, 2007; Fager, Hux, Beukelman, & Karantounis, 2006). A range of layouts are available (e.g., alphabet or ABC, QWERTY, and other optimized layouts). Limited objective information on the visual-cognitive processing demands of these layouts exists to guide clinical decision-making for keyboard selection. Individuals with acquired injuries, particularly those who have sustained a head injury, may have changes in their visual and cognitive capabilities (e.g., diplopia, decreased speed of processing, memory impairments) that can impact their ability to efficiently use different keyboard designs (Fager, Doyle, & Karantounis, 2007).
Eye tracking analysis can provide objective information on the processing demands of interface content and is being used increasingly to investigate the visual processing demands of displays and interfaces designed to support communication (Thiessen, Beukelman, Ullman, Longenecker, 2014; Wilkinson & Light, 2011; Light & McNaughton, 2014; Wilkinson & Mitchell, 2014; Wilkinson & Light, 2014; Brady, Anderson, Hahn, Obermeier, & Kapa, 2014; Gillespie-Smith & Fletcher-Watson, 2014). Providing objective information on the visual-cognitive processing demands of interfaces could guide clinical intervention and increase efficiency of access for individuals with acquired injuries.
PURPOSE
The purpose of this single subject, repeated measure design was to investigate whether there was a difference in the visual-cognitive processing demands between ABC (alphabet) and QWERTY onscreen keyboard layouts using standard mouse access for individuals with SCI/TBI as well as typical individuals.
METHODS
Participants
Participants included 3 male individuals (ages 27, 48 and 58) who had sustained spinal cord injuries (SCI) with co-occurring traumatic brain injuries (TBI). These participants were currently undergoing inpatient rehabilitation at the time of the study. All demonstrated cognitive abilities sufficient to complete the study tasks (Ranchos Los Amigos Scale of Cognitive Functioning- RLA 8-10) (Hagan, Malkmus, & Durham, 1979).Ten typical (neurologically intact) participants (6 females and 4 males between the age of 22-35) were also recruited for the study. All participants were literate and able to use their right hand to control a typical mouse.
Hardware/Software
The keyboard layouts used for the investigation were the ABC and QWERTY onscreen keyboards available in Tobii/Dynavox’s Compass4 software program. Compass is a commercially available augmentative and alternative communication software program. During the study all participants typed stimulus sentences using a typical computer mouse to access individual letters and punctuation.
The Tobii X2-601 eye-tracking system is specifically designed to study eye movements (saccades) and pauses (fixations) around visual stimuli presented on a computer screen. The Tobii X2-601 consists of a small eye-tracking camera that can be affixed to a range of computer monitors. For this study, the Tobii X2-601 was affixed to a Lenovo2 Thinkpad Ultrabook laptop. Tobii Studio3 analysis software was used to record and analyze participant eye movements. Because the objective of the study was to capture the visual search strategies used by participants finding letters on different onscreen keyboards, the fixations captured were set to 40 ms to increase sensitivity to views on areas of interest (Wilkinson & Light, 2011; Thiessen, Beukelman, Ullman, & Longenecker, 2014).
The sentence stimuli were taken from the Hearing In Noise Test (HINT) (Nilsson, Soli, & Sullivan, 1994). This sentence set was chosen as the sentences are comprised of 5-6 words and are relatively easy for the participant to remember while dictating. The HINT consists of sets of 10 sentence lists. All participants were assigned to two difference sentence sets (20 sentences total: 10 for ABC keyboard layout and 10 for QWERTY keyboard layout). Sentences from the lists were also randomly assigned to each condition (ABC or QWERTY keyboard layout).
Procedures
Following informed consent, all participants were seated in front of the Tobii X2-601 eye-tracker and calibrated using a 5-point calibration. All participants passed initial calibration and this calibration setting was used for all stimuli presented.
Individual target stimuli (sentences) were presented verbally and visually to the participants. After each sentence was presented, the participant used a standard mouse to select the letters of each word of each sentence on the specified onscreen keyboard layout. Each sentence was individually recorded using the screen recording feature of the Tobii Studio software for subsequent analysis.
After completing all sentences, the participants were asked about their personal experiences using onscreen keyboards on their personal cell phones, what their keyboard preference was, and any qualitative comments regarding the study were captured. Participants were allowed breaks as needed. Sessions for the participants without disability averaged 30-40 minutes in duration and sessions for the participants with disabilities averaged 60 minutes in duration.
Data Analysis
Using Tobii Studio3, areas of interest were drawn around each keyboard for each participant recording. Tobii Studio3 analysis software calculates the points of eye fixation on areas of interest. The fixation counts and total fixation durations for each sentence and each participant was analyzed for this project.
Mean fixation counts and standard deviations as well as mean total fixation durations and standard deviations were calculated for each participant across all sentences. Paired t-tests were used to statistically analyze results.
RESULTS
Fixation Count
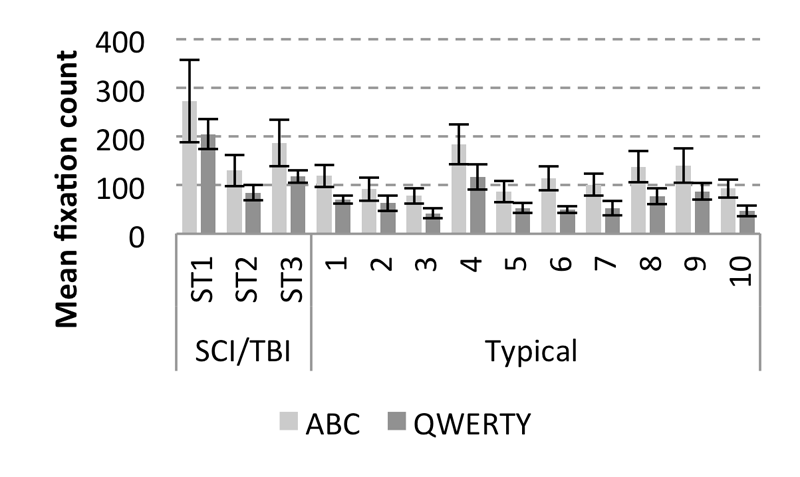
The mean fixation count and standard deviation for each participant is shown in figure 1.
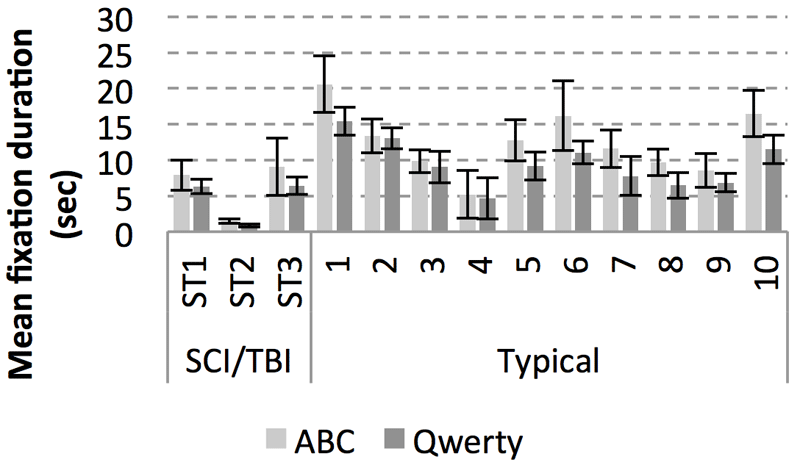
Total Fixation Duration
For the participants with SCI/TBI, the mean total fixation duration was 6.15 seconds (SD = 4.08) for ABC layout and 4.55 seconds (SD = 1.83) for QWERTY layout. The difference between layout type was not significant, t(2) = 2.73, p = 0.112. For non-disabled participants, the mean total fixation duration was 12.43 (SD = 4.48) seconds for ABC layout and 9.50 (SD = 3.29) seconds for QWERTY layout. The difference between the layout type was significant, t(9) = 4.80, p = 0.001.
Experience Using Onscreen Keyboards and Qualitative Comments
All participants reported experience using QWERTY onscreen keyboards on their personal smart phones to support texting communication. Of the participants with SCI/TBI, 1 reported texting hourly, 2 reported texting 10-15 times per day, and 1 reported texting a few time per week. Of the non-disabled participants, 7 reported texting hourly, 2 reported texting 12-20 times per day, and 1 reported texting 5-10 times per day. All participants indicated that they preferred the QWERTY keyboard over the ABC keyboard layout and they all commented that they had difficulty locating the letters on the ABC keyboard. For example, the participants with disabilities had the following comments:
Participant ST1: “I don’t like this alphabet style thing. It’s too hard to find the letter.”
Participant ST2: “You switched up on me. I was kinda having to hunt and peck with alphabet board.”
The typical participants had similar comments:
Participant 7: “I felt lost using the alphabet keyboard and had to retrace my steps.”
Participant 10: “I was slower using the alphabet keyboard.”
CONCLUSION
Mean fixation counts were significantly lower for QWERTY layout compared to ABC layout for all participants indicating a lower visual-cognitive processing demand imposed by using the QWERTY keyboard. While a statistical group comparison was not made with this data due to the low number of SCI/TBI participants compared to typical participants, the participants with SCI/TBI tended to have higher counts of fixations than the typical participants.
Mean total fixation durations were not significant between keyboards for the participants with SCI/TBI but were for the typical participants in that the QWERTY keyboard yielded shorter total fixation durations. However, the total fixation durations were generally shorter (and for participant ST2 substantially shorter) for the participants with SCI/TBI compared to most of the typical participants. Preliminary analysis of these results indicates that the participants with SCI/TBI demonstrated more fixations and shorter total fixation durations compared to the typical participants. This may potentially indicate an inefficiency in visual-cognitive processing (more searching = more fixations, less time spent focusing = shorter fixations) that may not be evident in individuals without neurologic injury. However, as this is preliminary data from three individuals further data on more individuals with SCI/TBI is needed to substantiate the notion of inefficiency.
The eye tracking data in the study corroborates with the qualitative comments for all participants indicating a preference for use of the QWERTY keyboard as well as more difficulty finding the target letter while using the ABC keyboard compared to the QWERTY keyboard. All participants also had extensive experience using QWERTY onscreen keyboards to text on their smart phones prior to the experiment and prior to their injuries. For individuals with acquired disabilities, consideration of their pre-injury experience with keyboard interface options would be clinically relevant. Attempts to utilize interfaces that are similar to standard, commercially available technologies may influence their efficiency, decrease frustration, and increase acceptance.
Further investigations of larger groups of individuals with disabilities as well as different levels of interface familiarity and utilization is needed to more fully understand the visual-cognitive processing demands of different keyboard types.
FOOTNOTES
1Tobii X2-60 by Tobii Pro, Tobii Technology, Inc., 510 N., Washington Street, Suite 200, Falls Church, VA, 22046, 1-703-738-1300. http://www.tobiipro.com
2Lenovo, 1-855-253-6686, http://www.lenovo.com/us
3Tobii Studio by Tobii Pro, Tobii Technology, Inc., 510 N., Washington Street, Suite 200, Falls Church, VA, 22046, 1-703-738-1300. http://www.tobiipro.com
4Compass by Tobii/Dynavox, 1-800-344-1778, http://www.tobiidynavox.com
REFERENCES
- Brady, N.C., Anderson, C.J., Hahn, L.J., Obermeier, S.M., & Kapa, L.L. (2014). Eye tracking as a measure of receptive vocabulary in children with autism spectrum disorders. Augmentative and Alternative Communication, 30, 147-159.
- Britton, D., & Baarslag-Benson, R. (2007). Spinal cord injury. In Beukelman, Garrett, & Yorkston (Eds.) Augmentative communication strategies for adults with acute or chronic medical conditions (pp. 91-130). Baltimore: Paul H. Brookes Publishing Co.
- Fager, S., Doyle, M., & Karantounis, R. (2007). Traumatic brain injury. In Beukelman, Garrett, & Yorkston (Eds.) Augmentative communication strategies for adults with acute or chronic medical conditions (pp. 131-162). Baltimore: Paul H. Brookes Publishing Co.
- Fager, S., Hux, K., Beukelman, D.R., & Karantounis, R. (2006). Augmentative and alternative communication use and acceptance by adults with traumatic brain injury. Augmentative and Alternative Communication, 22,37-47.
- Gillespie-Smith, K., & Fletcher-Watson, S. (2014). Designing AAC systems for children with autism: Evidence from eye tracking research. Augmentative and Alternative Communication, 30, 160-171.
- Hagan, C., Malkmus, D., & Durham, P. (1979). Rehabilitation of the head injured adult: Comprehensive physical management. Downey, CA: Professional Staff Association of Ranchos Los Amigos Medical Center.
- Light, J., & McNaughton, D. (2014). From basic to applied research to improve outcomes for individuals who require augmentative and alternative communication: Potential contributions of eye tracking research methods. Augmentative and Alternative Communication, 30, 99-105.
- Nilsson, M., Soli, S.D., & Sullivan, J.A. (1994). Development of the hearing in noise test for the measurement of speech reception thresholds in quiet and in noise. Journal of the Acoustical Society of America, 95(2), 1085-1099.
- Thiessen, A., Beukelman, D.R., Ullman, C., & Longenecker, M. (2014). Measurement of the visual attention patterns of people with aphasia: A preliminary investigation of two types of human engagement in photographic images. Augmentative and Alternative Communication, 30, 120-129.
- Wilkinson, K.M. & Light, J. (2011). Preliminary investigation of visual attention to human figures in photographs: Potential considerations for the design of aided AAC visual scene displays. Journal of Speech Language & Hearing Research, 54(6), 1644-1657.
- Wilkinson, K.M. & Light, J. (2014). Preliminary study of gaze toward humans in photographs by individuals with autism, down syndrome, or other intellectual disabilities: Implications for design of visual scene displays. Augmentative and Alternative Communication, 30, 130-146.
- Wilkinson, K.M. & Mitchell, T. (2014). Eye tracking research to answer questions about augmentative and alternative communication assessment and intervention. Augmentative and Alternative Communication, 30, 106-119.
ACKNOWLEDGEMENT
The preparation of this paper was supported by funding from the U.S. Department of Health (Grant H133E140026, NIDILRR).