Chase M. Pfeifer, PhD1, Judith M. Burnfield, PhD, PT1, Srinivas Kota, PhD1, Thad W. Buster, MS1, Sonya L. Irons, PT, DPT, CCS1, Cassandra Sulski1, Carl A. Nelson, PhD, PE2
1Institute for Rehabilitation Science & Engineering, Madonna Rehabilitation Hospital, Lincoln, NE
2Mechanical & Materials Engineering, University of Nebraska - Lincoln
ABSTRACT
Cardiovascular exercise is essential for health and function, yet many children with disabilities experience difficulty engaging in traditional exercise programs at a level that promotes cardiovascular benefits. Recently, a prototype motor-assisted elliptical (the Pedi-ICARE) was created to promote intensive practice of walking and cardiovascular exercise for children. Lacking was a tool to automate Pedi-ICARE training speed adjustments to promote exercise within a target heart rate training zone. Through use of a micro-controller, heart rate receiver, and stepper motor, this study designed a custom heart rate control system for the Pedi-ICARE. Preliminary testing has shown promising results in the laboratory. Future testing with children and clinicians across a range of therapeutic settings will provide beneficial feedback on functionality and hard coded variables for speed manipulation.
Keywords:
heart rate, control system, gait
BACKGROUND
Walking and fitness are goals for many children so they can keep up with their friends and family during school and play activities. Yet many children with a physical disability face barriers to sustaining an active lifestyle. Barriers can include the cost and accessibility of exercise technology (Rimmer, 2007). The lack of usable exercise equipment is unfortunate, because engagement in moderate levels of physical exercise helps not only build strength and function, but also cardiovascular fitness (Alpert, 1990).
The ICARE (an Intelligently Controlled Assistive Rehabilitation Elliptical) was developed to provide rehabilitation settings and fitness facilities with an affordable technology that individuals with physical disabilities and chronic conditions could use to improve walking and fitness (Burnfield, 2011; Nelson, 2011). The ICARE addresses some of the limitations (e.g., cost and labor demands) with existing physical therapy devices such as partial body-weight support treadmill (PBWST) (Hesse, 1995), conventional over-ground training (COGT) (Bogataj, 1995), functional electrical stimulation (Bogataj, 1995), and robotic technologies such as the Lokomat (Hidler, 2009). The biomechanical patterns (joint kinematics, muscle activation) generated while using the ICARE closely emulate walking in healthy adults (Burnfield, 2010). More recently, a pediatric version of the technology was created to address the walking and fitness needs of children with physical disabilities and chronic conditions (Pedi-ICARE) (Nelson, 2015).
A unique feature of the ICARE and Pedi-ICARE is that the motor helps individuals move their legs by introducing propulsive force to the foot pedals in an “active assist” (AA) condition. In the “active assist plus” (AAplus) condition, the motor disengages when the user exerts sufficient effort to make the machine go faster than his/her selected comfortable speed. An ICARE or Pedi-ICARE therapy session does not require as much external manual assistance as would be required in typical gait training, such as COGT and PBWST, because the ICARE’s motor moves the pedals so that therapists do not have to assist with lower limb movement.
Some exercise devices include integrated technology that adjusts work load (resistance and/or speed) to ensure a user’s heart rate remains within a predetermined training range. Although the ICARE and Pedi-ICARE can monitor heart rate, as initially designed there was no capacity for therapists to input target HR ranges that could be used by the device to customize training parameters (e.g., speed, step length, body weight support) and challenge users appropriately.
PURPOSE
The purpose of this research was to design and create a prototype custom HR control system for the ICARE. Such a system should continually read the HR of the user and adjust the speed (in revolutions per minute or RPM) of the elliptical to maintain an inputted HR range. The presented system was installed and tested with the new Pedi-ICARE.
METHODS
Hardware Design
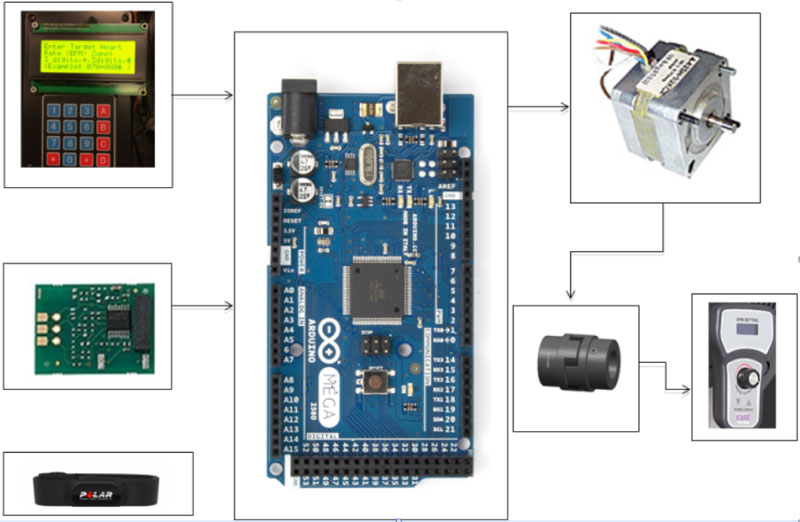
A stepper motor (six wires, 60 Ohm, 3.75 deg) was connected to the Arduino, and coupled with a shaft on a wired remote control with a flexible coupling and coupling spare. The wired remote control was used for speed setting of the Pedi-ICARE. The Arduino monitored heart beats through the HR receiver, measured the over time , and compared it with the target HR zone. If the exceeded for consecutive measurements, the stepper motor rotated to decrease the Pedi-ICARE’s speed by RPM. If the was less than for time seconds, consecutively for measurements, the stepper motor rotated to increase the Pedi-ICARE’s speed by RPM. This dynamic process continued until was in the target HR zone entered by a therapist. The overall goal was to ensure a user trains on the Pedi-ICARE within the target HR zone, neither lower than nor greater than . The block diagram of the custom heart rate control system is shown in Figure 1.
Operation
The display unit showed instructions to enter the user’s target HR zone in a valid format (example: three digits, *, three digits, # i.e. 070*080#) through a 4-row, 4-column keypad matrix. The Arduino script contained hard-coded initial values for the slowest and fastest HR (50 and 200 BPM) and for the time used for calculating average HR. The Arduino script checked for a valid target HR zone; thus and should be greater than or equal to 50 BPM and less than or equal to 200 BPM.
The first line in the display unit showed the user’s target zone (Example: Target HR 140-160). The second line showed ‘Cannot read’ if the HR receiver does not detect a heartbeat. As the HR receiver detects a heartbeat, the second line showed ‘Wait for few seconds’ for seconds until the Arduino computes . The second line showed the (Example: Current HR 78); this line updates every seconds. The third line showed ‘HR in Target Zone’ when the was within the target HR zone or ‘Reducing Speed’ if the was greater than or ‘Increasing Speed’ if the current was less than . Then, the third line showed ‘Speed Reduced Sec’ or ‘Speed Increased Sec’ immediately after reducing or increasing the speed, and finally the fourth line showed ‘NewEntry-PressAnyKey’ to enter a new HR zone. The text is tailored to 20 characters per the display capability. The target HR zone could be changed on this unit at any time by holding any key on the keypad matrix during the Pedi-ICARE training session if a therapist wished to train a patient in a new target HR zone.
Clinical Evaluation
Pilot testing was performed with the system, which included 22 children with disabilities and 20 children without disabilities. The variables hard-coded into the system were at 10 sec, at 3, and at 4 RPM. That is, if exceeded for 30 seconds, the ICARE’s speed was decreased by 4 RPM, or if was lower than for 30 seconds, the ICARE’s speed was increased by 4 RPM. The speed was unchanged if was in the target HR zone. Testing revealed that the Custom Heart Rate control system was able to detect when the participant’s HR was out of the desired zone and manipulate the speed of the elliptical accordingly 100% of the time. One drawback to these conditions was the time it took the system to confirm a HR outside of the suggested range. Future testing will adjust the hard-coded variables to reduce this time window.
CONCLUSION
The primary goal of this study was to design a system for the Pedi-ICARE that allows for clinicians to set a HR range and have the Pedi-ICARE automatically adjust training speed to maintain a participant’s HR in the given range. Hardware was assembled to interact with the speed controls on the Pedi-ICARE, and state-of-the-art micro-controllers and sensors were coded to effectively calculate the participant’s HR and manipulate the speed of the Pedi-ICARE. This system has been successfully tested in the laboratory setting with children at a 100% success rate but has yet to be included in an official clinical study to assess the impact on training outcomes.
FUTURE WORK
This system will be tested in the patient/clinician population for feedback on functionality. Currently an external stepper motor is used to manipulate the speed of the Pedi-ICARE. Future work with the manufacturers may lead to implementation of this system into the overall ICARE control system.REFERENCES
- Alpert, B., Field, T. M., Goldstein, S., & Perry, S. (1990). Aerobics enhances cardiovascular fitness and agility in preschoolers. Health Psychology, 9(1), 48.
- Bogataj, U., Gros, N., Kljajić, M., Aćimović, R., & Maležič, M. (1995). The rehabilitation of gait in patients with hemiplegia: a comparison between conventional therapy and multichannel functional electrical stimulation therapy. Physical Therapy, 75(6), 490-502.
- Burnfield, J. M., Shu, Y., Buster, T. W., Taylor, A. P., & Nelson, C. A. (2011). Impact of elliptical trainer ergonomic modifications on perceptions of safety, comfort, workout, and usability for people with physical disabilities and chronic conditions. Physical Therapy, 91(11), 1604-1617.
- Burnfield, J. M., Shu, Y., Buster, T., & Taylor, A. (2010). Similarity of joint kinematics and muscle demands between elliptical training and walking: implications for practice. Physical Therapy, 90(2), 289-305.
- Hesse, S., et al (1995). Treadmill training with partial body weight support compared with physiotherapy in nonambulatory hemiparetic patients. Stroke, 26(6), 976-981.
- Hidler, J., et al (2009). Multicenter randomized clinical trial evaluating the effectiveness of the Lokomat in subacute stroke. Neurorehabilitation and Neural Repair, 23(1), 5-13.
- Nelson C. A., Stolle CJ, Burnfield JM, Buster TW (2015). Modification of the Intelligently Controlled Assistive Rehabilitation Elliptical (ICARE) system for pediatric therapy. ASME Journal of Medical Devices, 9, 041010. DOI: 10.1115/1.4030276.
- Nelson, C. A., Burnfield, J. M., Shu, Y., Buster, T. W., Taylor, A. P., & Graham, A. (2011). Modified elliptical machine motor-drive design for assistive gait rehabilitation. Journal of Medical Devices, 5(2), 021001.
- Rimmer, J.H., Rowland, J.L., & Yamaki, K. (2007). Obesity and secondary conditions in adolescents with disabilities: addressing the needs of an underserved population. Journal of Adolescent Health, 41(3), 224-229.