Qussai M. Obiedat, Maysam M. Ardehali, Roger O. Smith
Rehabilitation Research Design & Disability (R2D2) Center, Department of Occupational Science & Technology, University of Wisconsin-Milwaukee, Milwaukee, WIAbstract
Recently, there has been an increasing interest in developing brain-computer interface (BCI) technology. BCI technology is a promising venue to overcome the shortcomings of the available rehabilitation methods of restoring normal motor function in people with disabilities. BCI have the potential to improve the quality of life and aid motor recovery of people with severe motor impairments through the development of both adaptive control and therapeutic intervention BCI systems. This paper reviews several affordable EEG systems that have been developed recently, provides an example of an EEG-BCI-FES system, and discusses several factors that both rehabilitation engineers and therapists have to fulfill in order to facilitate the adoption of BCI systems in the rehabilitation field and clinical practice.Introduction
In the past couple of decades, there has been an increasing interest in developing brain-computer interface (BCI) technology in gaming, military control of equipment, and in biofeedback systems. In the rehabilitation field, BCI technology was developed to improve the quality of life and aid motor recovery of individuals with various types of disabilities (Daly & Wolpaw, 2008). The need for such innovative technology comes from the shortcomings of the available rehabilitation methods to restore motor function for individuals suffering progressive diseases, such as multiple sclerosis (MS), amyotrophic lateral sclerosis (ALS), or Parkinson’s disease, or for many individuals with severe motor impairments due to stroke, cerebral palsy, or injuries to the brain or spinal cord. The applications of BCI technology in rehabilitation can be classified into two main categories: Adaptive control and Therapeutic intervention. The first category focuses on enabling people with disabilities (PWD) to control and interact with their surrounding environment. Communication programs, such as P300 speller (Cecotti, 2010), are good examples of BCI systems in this category. The second category aids in restoring impaired motor functions of both upper and lower extremities, such as the restoration of motor function through using brain guided functional electrical stimulation (FES) (Teo & Chew, 2014).
The purpose of this paper is to review the different components of BCI systems and their working process. Compare some of the available electroencephalography (EEG) systems, provide an example of a BCI system to guide the delivery of functional electrical stimulation (FES), and discuss additional requirements that need to be implemented in order to facilitate adoption of BCI systems in clinical practice.
A review of BCI Systems
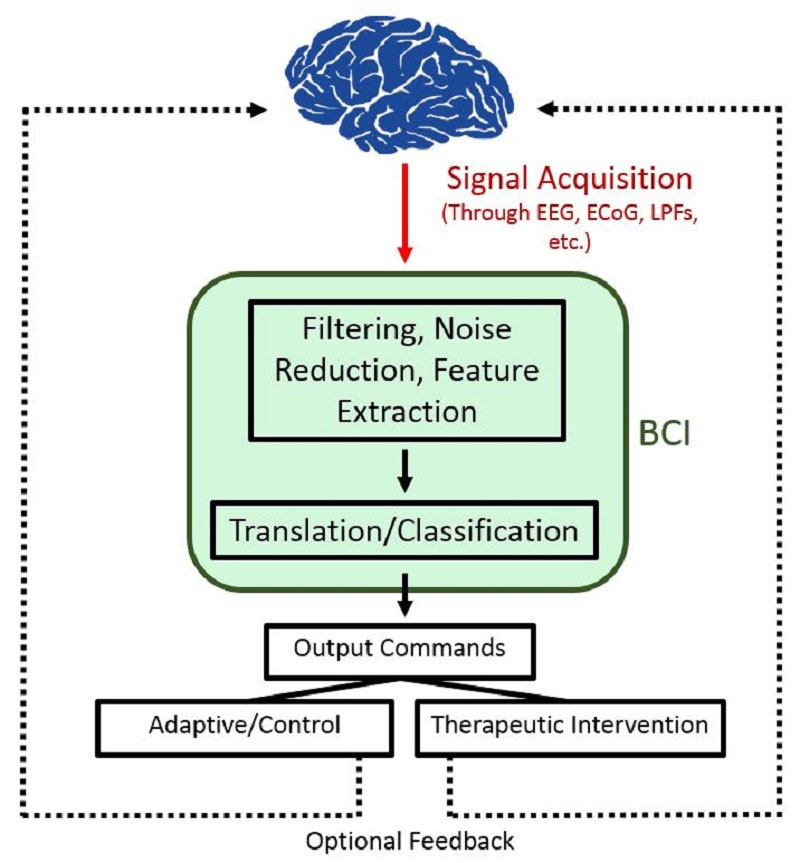
Generally, BCI systems are responsible for translating brain-generated electrophysiological signals to control signals, which in turn are used to drive external devices or applications. The general working process of a BCI system can be broken down into steps shown in Figure 1. Acquiring brain electrophysiological signals via proper electrodes is the first step. Then the signal is processed and classified. Finally, the signal classification component which is composed of the brain signal feature extraction and the translation of these signals into output commands for a certain device or application (Schalk, McFarland, Hinterberger, Birbaumer, & Wolpaw, 2004).
Electrophysiological Brain Signals
EEG systems
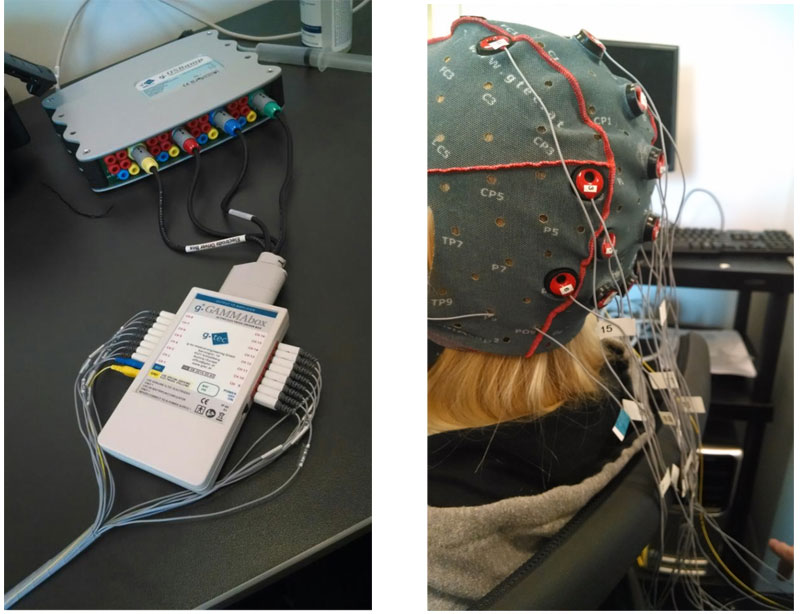
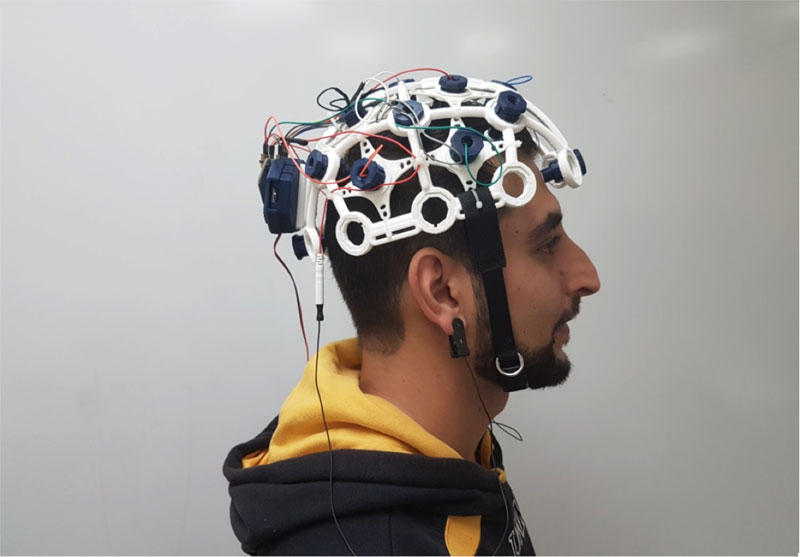
Wide variety of EEG systems have been developed recently. G.tec® Medical Engineering is one of the leading companies that provides advanced, research grade EEG systems (Figure 1). However, these systems are expensive. Emotive, Inc. (Figure 2) and OpenBCI group (Figure 3) recently developed an affordable and portable EEG acquisition system. Such systems provide the ability to study brain activities while the individual engages in daily activities, and a practical solution for operating different BCI applications in different contexts and settings. Different characteristics of the three systems are described in Table 1.
EEG-BCI system process

In order for the BCI system to be able to train itself, the EEG signal must be processed first, and in real-time in most cases. Signal processing usually entails 1) noise reduction, 2) feature extraction, and 3) classification (Roman-Gonzalez, 2012). Noise reduction phase utilizes filters (low-pass, high-pass, mid-pass, and notch) to provide a “clean” signal to its output.
After the EEG signal is devoid of contamination to the best possible extent, the feature extraction phase begins. In this phase, the goal is to separate useful values (features) of the signal from the rest. Sometimes noise reduction is also embedded in this phase. These values or features should be representative of different mental states. Usually, after the features are extracted, they are arranged in a vector, known as a feature vector (Lotte, 2014). Classification phase is concerned with assigning a class to a feature vector, corresponding to the identified mental state. Algorithms responsible for classification are called “classifiers”. In other words, this step acts as an interface between features and commands. Classifiers use pattern recognition and machine learning in order to learn how to classify different feature vectors (Lotte, 2014; Lotte, Congedo, Lécuyer, Lamarche, & Arnaldi, 2007). This means that classification methods are unique and tailored for each subject, as the same mental tasks do not usually evoke the same responses in different individual’s brains. The patterns by which the classifier learns how to classify different feature vectors, are usually acquired during the training phase.
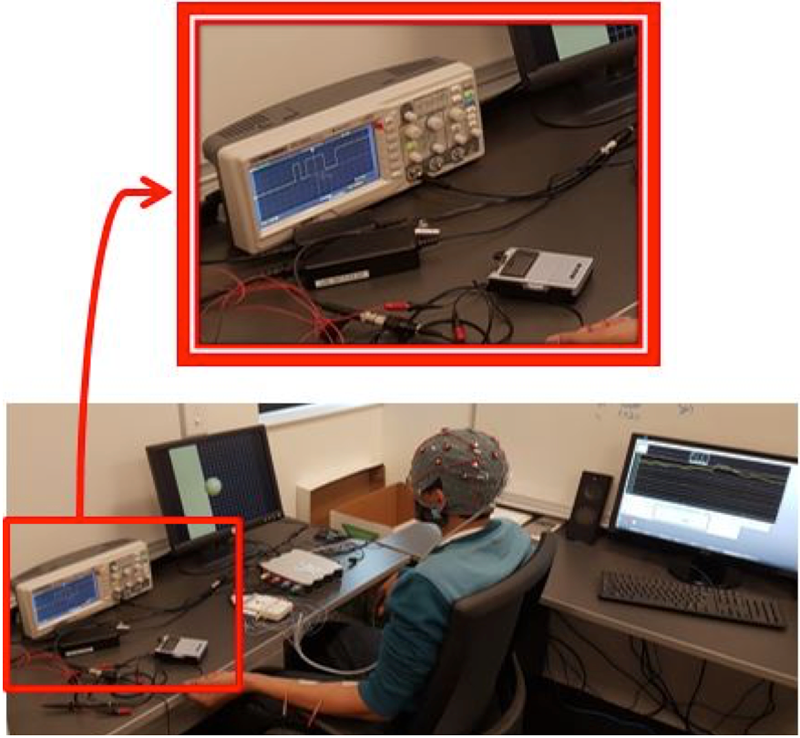
EEG-BCI Guided FES
FES provides muscular contraction and produces a functionally useful movement via providing electrical stimulation for muscles deprived of nervous control (Liberson, Holmquest, Scot, & Dow, 1961). It has been found that this method enhances post-stroke motor recovery (Kralj, Aˇmović, & Stani, 1993), reduces spasticity (Alfieri, 1981), strengthen muscles, and increases the range of motion of affected joints (Baker, Yeh, Wilson, & Waters, 1979). FES has been found to be most effective when combined with MI (Reynolds, Osuagwu, & Vuckovic, 2015). Such combination can lead to an increase in neuroplasticity, which in turn, improves motor learning (Celnik & Cohen, 2004; McDonnell & Ridding, 2006). Mental imagination of movement can be detected using a BCI system, and, if detected, in combination with FES, can provide a solid means to influence brain plasticity processes that could induce recovery of normal motor functions.
| EEG System | Channels | Electrodes | Connection | Portability | Cap | Cost |
| G.tec® Medical Engineering g.USBamp & g.GAMMAbox | 16 | Wet/gel | Wired | No | Fabric | ~ $30,000 |
| Emotive Inc. EPOC+ | 14 | Saline soaked felt pads | Wireless | Yes | Headset | $799 |
| OpenBCI | 8-16 | Dry | wireless | Yes | 3D printable | ~ $1,300 |
In EEG-BCI-FES application, imagination of a particular movement is the task for which the features need to be extracted and then classified to translate the intention of movement to trigger electrical stimulation. Electrodes are placed on and around the motor cortex area to detect sensorimotor rhythms from both hemispheres.
Discussion
References
Alfieri, V. (1981). Electrical treatment of
spasticity. Reflex tonic activity in hemiplegic patients and selected specific electrostimulation. Scandinavian journal of rehabilitation medicine, 14(4), 177-182.
Baker, L. L., Yeh, C., Wilson, D., & Waters, R. L.
(1979). Electrical stimulation of wrist and fingers for hemiplegic patients. Physical Therapy, 59(12), 1495-1499.
Cecotti, H. (2010, August). Spelling with brain-
computer interface-current trends and prospects. In Cinquième conférence plénière française de Neurosciences Computationnelles," Neurocomp'10" (pp. 215-220).
Celnik, P. A., & Cohen, L. G. (2004). Modulation
of motor function and cortical plasticity in health and disease. Restorative neurology and neuroscience, 22(3-5), 261-268.
Daly, J. J., & Wolpaw, J. R. (2008). Brain–
computer interfaces in neurological rehabilitation. The Lancet Neurology, 7(11), 1032-1043.
Kralj, A., Aˇmović, R., & Staniˇ, U. (1993).
Enhancement of hemiplegic patient rehabilitation by means of functional electrical stimulation. Prosthetics and Orthotics International, 17(2), 107-114.
Liberson, W. T., Holmquest, H. J., Scot, D., &
Dow, M. (1961). Functional electrotherapy: stimulation of the peroneal nerve synchronized with the swing phase of the gait of hemiplegic patients. Archives of physical medicine and rehabilitation, 42, 101-105.
Lotte, F. (2014). A tutorial on EEG signal-
processing techniques for mental-state recognition in brain–computer interfaces. In Guide to Brain-Computer Music Interfacing (pp. 133-161). Springer London.
Lotte, F., Congedo, M., Lécuyer, A., Lamarche,
F., & Arnaldi, B. (2007). A review of classification algorithms for EEG-based brain–computer interfaces. Journal of neural engineering, 4(2), R1.
McDonnell, M. N., & Ridding, M. C. (2006).
Afferent stimulation facilitates performance on a novel motor task. Experimental Brain Research, 170(1), 109-115.
Pfurtscheller, G., & Neuper, C. (2001). Motor
imagery and direct brain-computer communication. Proceedings of the IEEE, 89(7), 1123-1134.
Pfurtscheller, G., Müller-Putz, G. R., Scherer, R.,
& Neuper, C. (2008). Rehabilitation with brain-computer interface systems. Computer, 41(10).
Reynolds, C., Osuagwu, B. A., & Vuckovic, A.
(2015). Influence of motor imagination on cortical activation during functional electrical stimulation. Clinical Neurophysiology, 126(7), 1360-1369.
Roman-Gonzalez, A. (2012). Eeg signal
processing for bci applications. In Human–Computer Systems Interaction: Backgrounds and Applications 2 (pp. 571-591). Springer
Schalk, G., McFarland, D. J., Hinterberger, T.,
Birbaumer, N., & Wolpaw, J. R. (2004). BCI2000: a general-purpose brain-computer interface (BCI) system. IEEE Transactions on biomedical engineering, 51(6), 1034-1043.
Subasi, A. (2007). EEG signal classification using
wavelet feature extraction and a mixture of expert model. Expert Systems with Applications, 32(4), 1084-1093.
Teo, W. P., & Chew, E. (2014). Is motor-imagery
brain-computer interface feasible in stroke rehabilitation?. PM&R, 6(8), 723-728.