Handheld PC/ Web-based Task Reminder for Brain-Injured Adults
ABSTRACT
Reminding systems for individuals with traumatic brain injury provide a compensatory approach to cognitive rehabilitation therapy. Programming and operation of most off-the-shelf planners/schedulers is too complex for effective use by individuals with TBI. This study explored the use of remote programming of messages downloaded to a hand-held PC. Users with TBI responded to alarms, received messages and indicated level of task completion through the hand-held device. Performance was uploaded to a website for review and modification by the therapist. Analysis showed significant improvement in task completion with handheld PC message delivery as opposed to note taking. Users responded favorably to remote task programming and modifications.
KEYWORDS
Memory devices, cognitive rehabilitation, cognitive prostheses
BACKGROUND
Computer-assisted cognitive retraining (CACR) has been in existence since the early 1970's (Lynch, 2002). Much of the early work centered on the use of videogames or specifically written software aimed at improving attention, concentration and memory skills to restore damaged cognitive systems. Most studies had difficulty demonstrating the efficacy of these electronic work book style tasks as they had little functional application and did not generalize to everyday activities. In the past seven years, the development of hand-held PDA's have provided scheduling, organizing, and reminding functions that provide compensatory functions for individuals with TBI. Use of off-the-shelf PDA's with standard Palm and Windows CE-based professional management software has presented further difficulties for TBI patients and their families. Programming and multiple complex displays frequently serve to confuse users with decreased memory and learning abilities. Software for hand-held PC's, such as PEAT (Levinson, 1997) and Pocket Coach (Ablelink, 2003) have been developed to address some of these needs. These programs provide simplified displays and use visual or spoken directions to assist users with TBI or mental retardation in managing their schedule or in following steps to complete everyday activities.
The application of telehealth delivery of rehabilitation services has great potential for the TBI population. Routinely individuals with TBI spend years or the remainder of their lives in dealing with the consequences of their injuries. While outpatient rehabilitation services are being limited, individuals with TBI frequently require longer and more complex therapy regimens than individuals recovering from stroke or other neurological conditions. Provision of telerehabilitation services offers potential for individuals in both rural and urban areas to receive ongoing cognitive rehabilitation.
RESEARCH QUESTION
We were interested in determining if remote programming of user-defined tasks delivered through a hand-held PC (Compaq Ipaq) would provide a means of reducing the burden of user management of a reminding system, while providing a therapist with monitoring and adjusting of performance through a website. Specific objectives of the clinical testing of a hand-held PC/Web-based memory aid (The Jogger) were to: 1) determine the reliability of electronic task prompt delivery, response recording, data storage and transfer, 2) measure the effects on performance of selected tasks relevant to independent living, and 3) collect qualitative evaluations from users.
METHOD
Subjects
Subjects included 12 adult outpatients with a history of traumatic brain injury and cognitive impairment and their caregivers (N=12). Criteria for subject enrollment included: between ages 21-55; history of TBI >3 months prior to enrollment with clear history of concussion or more severe complications (e.g. intracerebral edema or hemorrhage, skull fracture); impairment of short-term memory documented by result of screening assessment (Rivermead Behavioral Memory Test score <21); no visual impairment that would prevent use of the screen display of the hand-held PC; reading ability for sentences; no hearing impairment that would prevent use of the sound alarms; intact receptive language ability; no sensory or movement disorder to prevent correctly depressing keys on the touch screen; and a caregiver living with or nearby the patient. Caregiver criteria for enrollment included: age > 21; currently living with or nearby eligible TBI patient, ability to monitor TBI subjects performance during study period; currently provides directions or supervises task performance by TBI patient; no significant cognitive impairment to prevent accurate reporting of task performance; and no sensory or movement disorder to prevent use of the hand held PC, battery charger or modem.
Reminding System
 |
|---|
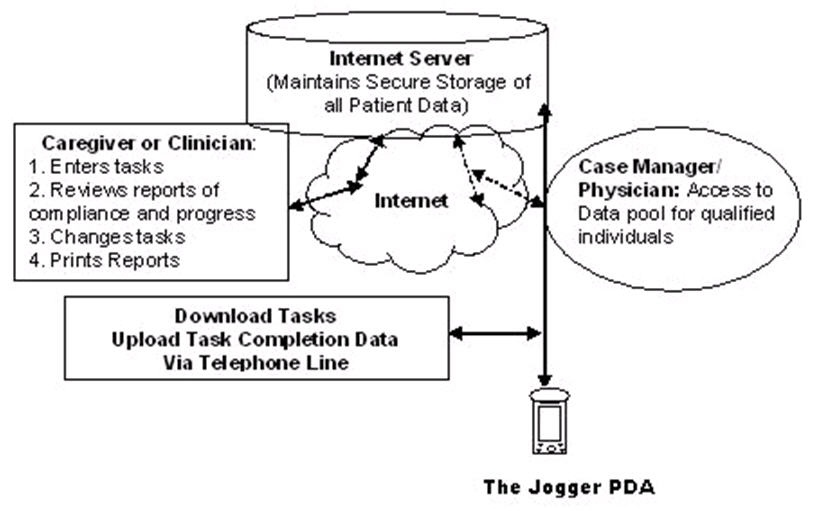
The Jogger is a device to remind individuals of significant events, and the actions to be taken related to these events. The device uses a website for transmission of information, The system has four primary functions: 1) to provide therapists and caregivers the ability to download tasks their patients need to complete via a website; 2) to signal the patient through the handheld PC that a scheduled task needs to be completed; 3) to present a message describing the task; and 4) to record the patient's response to the message. The hand-held device prompts the patient of an impending task through one or more modalities (voice, chimes, flashing light). The hand-held device records the patient's response to a prompt, and records the time it takes to complete the task. If the patient takes no action, an "ignored" response is recorded. At the end of the day, the Jogger is docked and responses are uploaded to the web server. New messages are then downloaded for the following day. The therapist or caregiver uses their computer to monitor the responses on the website, and to enter new tasks. Case managers and physicians could also have access to the information if authorized.
Procedures
 |
|---|
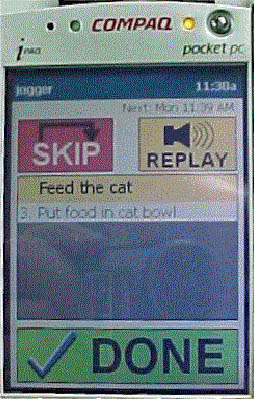
Subjects and their caregivers participated in the study over a 4-week period. They met with the therapist on 4 occasions (initial, after 1 week, 3 weeks, and final). During the first week of the study, subjects and their caregivers established 5-10 daily tasks that they needed reminding to complete. A list of sample tasks was provided to assist with recall. Tasks and expected time of completion were logged on a "caregiver journal" tracking sheet. This sheet was returned at the end of week 1.At the second meeting with the therapist, current or additional tasks were identified for programming to The JoggerT website. Subjects and their caregivers were trained in operation of The Jogger hand-held device. During weeks 2 and 3, daily messages were delivered to the subject. Response keys for Done, Skip, and Replay were available for tracking performance or providing additional cueing.
Subjects carried the hand held devices, responded to the messages and followed the requested task. At the end of each day, the device was docked in a cradle. Automatic uploading of current messages and downloading of new messages occurred during the night. The therapist was able to track subject performance daily by monitoring the uploaded message response. Subjects were called if they failed to correctly dock the device and to adjust messages based on subject or caregiver input. For the fourth week of the study, half of the tasks to be completed were recorded on the "caregiver journal" and half were delivered through the hand held PC.
RESULTS
The primary statistical evaluation of results compared rates for task performance (total # of tasks done/total # of tasks scheduled) in the unprompted condition (weeks 1+4: 0.61 +/- 0.21) to the Jogger prompted condition (weeks 2+3+4: 0.76 +/- 0.11). There was a statistically significant improvement with Jogger use (t=2.785, df =11, p=0.177). In addition, exploratory statistical analyses found that there was a significant inverse correlation (r= -.83, p =0.0007) between the unprompted rate for task performance and a "change score" (calculated as [rate prompted-rate unprompted] / rate unprompted). This suggests that the more impaired subjects had the most improvement with the Jogger system use. There were no significant correlations between cognitive measures and rates of task performance or change. In a post-test survey, 75% or more of the subjects responded favorably to the reliability, recharging, dependability, therapist assistance and functionality of the Jogger.
DISCUSSION
The viability and user acceptance of remote delivery of alarms and messages through a PC-based PDA (The Jogger) was demonstrated for brain-injured patients. Subjects reported support and interest in use of a hand-held electronic reminding system as a means of fostering independent completion of tasks, appointments, and other user-defined activities. Daily monitoring of performance through a web-based report form permitted the therapist to adjust alarms and messages based on patient's selection of task completion key, cancel key, or ignoring of alarm and message. Further research with wireless technology and providing reminding systems for differing populations that suffer memory deficits is planned.
REFERENCES
- Able Link Technologies, "Measuring the Impact of Using Assistive Technology Software on a Palmtop PC for Increasing Independence and Productivity for Persons with Mental Retardation in Inclusive Settings" http://www.ablelinktech.com/ResearchPage.asp?SelectedProduct=PocketCoach 2003.
- Levinson, R, "PEAT - The Planning and Execution Assistant and Trainer" Journal of Head Trauma Rehabilitation, Aspen Press, April, 1997.
- Lynch, B, "Historical review of computer-assisted cognitive retraining" Journal of Head Trauma Rehabilitation, October, 2002.
ACKNOWLEDGMENTS
This study was funded by the National Institute of Health SBIR grant # R43 NS43834-01.
Author Contact Information:
Andrew Jinks, MA,
UPMC Rehabilitation Hospital,
1405 Shady Ave.,
Pittsburgh,
PA 15217,
Phone (412) 420-2422
EMAIL: jinksa@upmc.edu