29th Annual RESNA Conference Proceedings
The Effect of Restricted Ankle Motion on Stair Ambulation
Allen H. Hoffman, PhD, Rosanna C. Glynn, MS, and Holly K. Ault, PhD
Mechanical Engineering Department, Worcester Polytechnic Institute, Worcester, MA 01609
ABSTRACT
The kinematics of stair ascent and descent was investigated in 5 young adult females under normal conditions and where an ankle-foot orthosis (AFO) was used to restrict left ankle flexion. Joint goniometers, sampled at 50 Hz, were used to record the angles of the hips, knees and ankles. With the exception of the right hip, restricting left ankle flexion caused a significant change in at least one kinematic variable associated with each of the other joints. These results likely parallel the effects of wearing a transtibial prosthesis that restricts ankle motion.
KEYWORDS
Stair ascent/descent, prostheses, orthoses, gait
BACKGROUND
Stair ascent and descent is a challenging activity for persons with lower limb prostheses. These prostheses generally restrict ankle flexion. A better understanding of the effects of ankle restriction could lead to improved designs for lower limb prostheses. Prior studies have investigated stair ambulation in normal subjects (1), in amputees using transtibial prostheses (2), and have compared normal subjects with amputees using transtibial prostheses (3). However, the majority of below the knee amputations occur from non-trauma related causes, such as diabetes. Thus, comparisons of stair ambulation between normal and amputee groups may be influenced by underlying medical conditions and age. The effect of restricting ankle motion in normal children has been investigated (4). An advantage of this type of study is that each subject serves as his/her own control.
RESEARCH QUESTION
Previous studies of the effect of restricted ankle motion on stair ambulation in adults have compared normal populations to populations using transtibial prostheses. These comparisons are potentially confounded by the existence of underlying medical conditions in the group of prosthesis users. To isolate the effect of restricted ankle motion in adults, there is a need to conduct studies in a normal population where each subject can serve as his/her own control.
METHODS
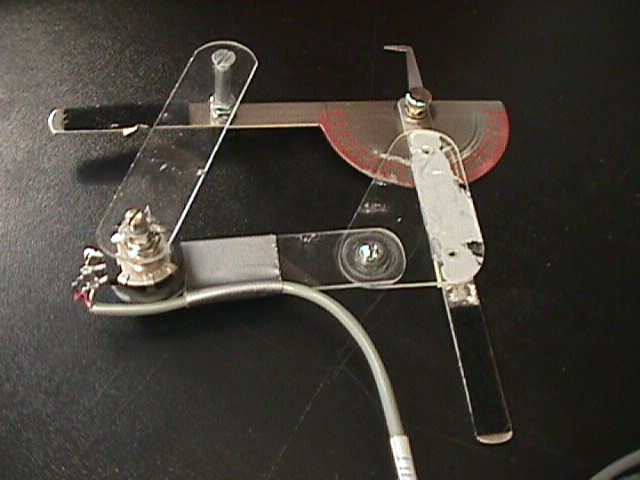 Figure 1: Knee Goniometer. Two arms of the parallelogram linkage are comprised of a commercial mechanical goniometer. The potentiometer is in the lower left corner of the linkage. (Click image for larger view)
Figure 1: Knee Goniometer. Two arms of the parallelogram linkage are comprised of a commercial mechanical goniometer. The potentiometer is in the lower left corner of the linkage. (Click image for larger view)
An ankle-foot orthosis (AFO) was used to restrict left ankle motion in five female subjects (age 22-26) who had no prior history of lower limb orthopedic injuries. Each subject completed 3 trials under each of the following four conditions; normal stair ascent, normal stair descent, stair ascent with the AFO and stair descent with the AFO. Goniometers containing potentiometers were used to record the joint angles of the hips, knees and ankles. Each pair of goniometers was based upon a parallelogram linkage. One joint in the linkage contained a potentiometer. Details of the knee goniometer are shown in Figure 1. The hip and ankle goniometers were generally similar in design.
 Figure 2. Knee Goniometer Mounted on Right Knee. The two metal arms of the parallelogram linkage opposite the potentiometer are aligned with the femur and tibia. (Click image for larger view)
Figure 2. Knee Goniometer Mounted on Right Knee. The two metal arms of the parallelogram linkage opposite the potentiometer are aligned with the femur and tibia. (Click image for larger view) Each goniometer was individually calibrated. The goniometers were affixed to each subject so that the joint of the parallelogram linkage opposite to the potentiometer coincided with the anatomical joint center (Figure 2).
Footswitches on the soles of the footwear were used to identify heel strike and toe off for each foot. Wiring from the goniometers and footswitches was brought to a common point and then tethered to a computer through a data acquisition board. The AFO was set to hold the left ankle in the neutral position. After donning the AFO, each subject spent 15 minutes acclimating herself to the orthosis before commencing the trials. Data were gathered using the first 5 stairs of a longer staircase. For both ascent and descent, the subject initiated stair ambulation with her right foot. The gait cycle was defined as the period between successive left heel strikes. These heel strikes occurred on the 2nd and 4th stairs during ascent and on the 3rd and 1st stairs during descent. Data were sampled at 50 Hz. Joint angle data were double smoothed using central differencing prior to analysis. Angular velocity was computed from the joint angle data. The footswitch data allowed determination of the stance and swing phase times as well as the total gait cycle time. The stance and swing phase times were normalized to the subject's gait cycle time. For each joint, angle versus time graphs were created and analyzed. For each variable, the mean values for each subject with and without the AFO were treated as paired variates (n=5).
RESULTS
Restricting ankle motion with an AFO on the left leg produced substantial variations in the kinematics of both legs (Table 1). When using the AFO, one of the subjects very substantially slowed her progression on the stairs when compared to the other subjects. As a result, a nonparametric Wilcoxon test was used to determine differences in gait cycle time and stance and swing phase times. Data from the other variables appeared to be reasonably normally distributed and a one-tailed t-test was used for analysis. Restricting ankle flexion caused a significant increase gait cycle time (p < 0.05). For stair ascent, the percentage of gait cycle devoted to left leg swing phase increased. There were statistically significant (p < 0.05) increases in the maximum flexion of the left hip as well as in the ranges of motion of the left hip, knee and right ankle. The maximum angular velocity of the left knee in stance increased as did the extension of the right knee. In stair descent, the percentage of the gait cycle devoted to right leg stance increased. Significant increases occurred in left hip flexion, range of motion and maximum swing angular velocity. The right knee extension and right ankle dorsiflexion also increased. The maximum stance angular velocity of the left knee decreased. In addition, Table 1 shows a number of other kinematic variables where the changes caused by restricted ankle motion are labeled as trends (0.05<p=0.10).
| All Subjects (n=5) | Ascent | Descent |
|---|---|---|
Gait Cycle |
||
| % Stance time - left leg | -* |
o |
| % Swing time - left leg | +* |
o * |
| % Stance time - right leg | o |
+* |
| % Swing time - right leg | o |
-* |
| Total gait cycle time | +* |
+* |
Maximum Joint Flexion |
||
| Left Hip | +* |
+* |
| Right Hip | o |
o |
| Left Knee | + |
o |
| Right Knee | - |
- |
Max. joint Extension |
||
| Left Hip | o |
o |
| Right Hip | o |
o |
| Left Knee | o |
o |
| Right Knee | +* |
+* |
Maximum Dorsiflexion
|
||
| Right Ankle | + |
+* |
Max. Plantar Flexion |
||
| Right Ankle | o |
o |
Mean Range of Motion |
||
| Left Hip | +* |
+* |
| Right Hip | o |
o |
| Left Knee | +* |
o |
| Right Knee | o |
o |
| Right Ankle | +* |
o |
Max. Stance Ang. Vel. |
||
| Left Hip | o |
+ |
| Right Hip | o |
o |
| Left Knee | +* |
-* |
| Right Knee | + |
o |
| Right Ankle | n |
o |
Max. Swing Ang. Vel. |
||
| Left Hip | + |
+* |
| Right Hip | o |
o |
| Left Knee | - |
- |
| Right Knee | o |
o |
| Right Ankle | o |
o |
DISCUSSION
Restricting ankle flexion on one leg creates an asymmetry in gait during stair ambulation. As noted in Table 1, wearing an AFO caused significant variations (p<0.05) in a number of gait parameters and joint kinematic variables. The majority of the kinematic variables were associated with the left hip and knee (4 of 6 in ascent, 4 of 6 in descent). Gait asymmetry and slower gait progression on stairs by transtibial prostheses users has been previously reported (2). The kinematic variables reported in Table 1 are based upon maximum values and therefore are not fully representative of the changes that occurred over the entire gait cycle. Phase plane plots (joint angular velocity versus joint angle) were used to develop a more detailed qualitative understanding of stair ambulation with and without the AFO over the gait cycle. For each joint, the phase plane plot for normal stair ambulation was compared to the corresponding phase plane plot for ambulation with restricted ankle motion. In all cases, regardless of the direction of ambulation, comparison of these two plots revealed distinctly different characteristics. Thus when viewed in the phase plane, it can be stated qualitatively that compensation for restricted ankle motion on one leg causes noticeable changes in the joint kinematics of all the joints on both legs.
A limitation of this study is the small number of subjects (n=5). Thus some of the effects reported as trends (0.05<p=0.10) in Table 1 might be significant in a larger sample size. It is also possible that some effects are exaggerated due to the relatively short time (15 minutes) allowed for the subjects to adapt to wearing the AFO. Despite these potential limitations, it is likely that the results of this study reflect several of the effects of wearing a transtibial prosthesis that restricts ankle motion.
REFERENCES
- Andriacchi, T. P., Andersson, G. B. J., Fermier, R. W., Stern, D. & Galante, J. O. (1997). A study of lower-limb mechanics during stair-climbing. Journal of Bone and Joint Surgery, 62-A: 749-757.
- Powers, C. M., Boyd, L.A., Torburn, L. & Perry J. (1997). Stair ambulation in persons with transtibial amputation: an analysis of the Seattle LightFoot ä . Journal of Rehabilitation Research and Development, 34: 9-18.
- Torburn L., Perry J., Ayyappa E. & Shanfield, S. L. (1990). Below-knee amputee gait with dynamic elastic response prosthetic feet: a pilot study. Journal of Rehabilitation Research, 27: 369-384.
- Nahorniak, M. T., Gorton, G. E. III, Gannotti, M. E. & Masso, P. D. (1999). Kinematic compensations as children reciprocally ascend and descend stairs with unilateral and bilateral solid AFOs. Gait and Posture, 9: 199-206.
Author Contact Information:
Allen H. Hoffman, PhD
Mechanical Engineering Department
Worcester Polytechnic Institute
100 Institute Road
Worcester, MA 01609-2280
Office Phone (508) 831-5217
EMAIL: ahoffman@wpi.edu
This should be in the right column.