An Improved Lateral Key-Pinch Grip Orthosis For Tetraplegics With Wrist Extension
Marcus J. King, BE1, Julian K. Verkaaik, BDes2, Fiona Collins, BHSc (OT), PGCert. MSc (clinical rehabilitation), NZROT3, Angela Nicholls, DipOT, Dip Erg, NZROT3.
1 Industrial Research Ltd., NZ
2 Burwood Academy of Independent Living, NZ
3 Burwood Spinal Unit, NZ
ABSTRACT
An orthosis has been developed to provide a lateral key-pinch grip for tetraplegics who have a functional wrist extension. This new design is less obtrusive than previous tenodesis splints and may be donned and doffed by the user independently of their caregiver. A clinical trial of the orthosis has been initiated and this report details the results of the first two participants. The trial measured the key grip force and also used an assessment tool that was developed to test functionality of 6 activities of daily living, including 13 subtasks. When using the orthosis, the participants could develop a key grip that was more than twice as great as without and could achieve approximately twice as many of the ADLs.
KEYWORDS:
quadriplegia; tetraplegia; orthosis; lateral pinch grip; key grip
STATEMENT OF THE PROBLEM
A spinal cord injury at the cervical region (C1-C7) of the spine results in paralysis affecting all limbs. Loss of function in the hands is very debilitating and previous authors (1, 2) report that most tetraplegics would prefer restoration of hand and arm function to that of any other function lost.
According to the American National Spinal Cord Injury Statistical Center (3), 14.8 % of spinal cord injuries occur at C5, 11% at C6 and 5.4% at C7. These 31% of all spinal cord injured persons have partial or complete loss of digital and/or wrist function and so require special orthoses and/or grasping techniques in order to carry out basic activities of daily living (ADL).
Many techniques and orthoses concentrate on restoring a lateral key-pinch grip (key grip) as the fundamental grip for people with tetraplegia. Lateral key grip is used in 20% of ADLs (4). However, this doesn’t demonstrate the full importance of key grip for a person who has no other alternative grip. Relatively small key grip forces are required to achieve independence. For example a key grip of 16 N can achieve 9 out of 12 ADL tasks (5) and a pinch force of 10 N is adequate for accomplishing the majority of simple grasping activities involving the digits (6).
CURRENT TECHNOLOGY
Solutions are available for restoring hand function to people with tetraplegia, such as tendon transfer surgery and functional electrical stimulation. However, these solutions are expensive, may not work for everyone, or therapists may determine that an individual is not yet suitable for such interventions for non-physical reasons such as motivation etc.
A tenodesis splint is a device used by C6-C7 tetraplegics to grasp objects and occasionally by some incomplete C5 tetraplegics, who lack finger movement but retain the ability to extend their wrist. Examples of devices include manually operated wrist extension devices manufactured by JAECO Orthopedic Inc. Arkansas, USA., or Orthotic Technical Services, Victoria Australia and powered devices are made by Broadened Horizons, Minnesota, USA. However, these devices tend to function by rigid links connecting stiff customised orthoses. As a result they are obtrusive and tend to be difficult for the user to don and doff independently and require an experienced occupational therapist to prescribe.
DESIGN AND DEVELOPMENT
In this paper we describe a wrist extension tenodesis key grip orthosis, that can be independently donned and doffed by the user. A system for assessment and training in the use of the orthosis is also described.
Gripping Mechanism:
The action of extending the wrist is harnessed to stretch a Bowden cable that runs along the dorsal region of the forearm to the palmar region of the hand. A Bowden cable, which is often used for bicycle brakes, has a tension cable that runs inside an outer sheath that holds the cable in position. The inner cable attaches to a ring around the thumb proximal phalanx. Tension on the cable pulls the thumb into palmar adduction so that a grip forms against the lateral region of the proximal or middle phalanx of the index finger. The cable outer is held in position by being attached to a hard rubber palmar pad that can also act as a wheelchair push pad. The proximal end of the cable inner is attached to a length adjustment system so that the cable length can be tuned to suit the requirements of the user. This length adjustment system is strapped to the palmar region of the forearm. Figure 1 shows a palmar view of the orthosis
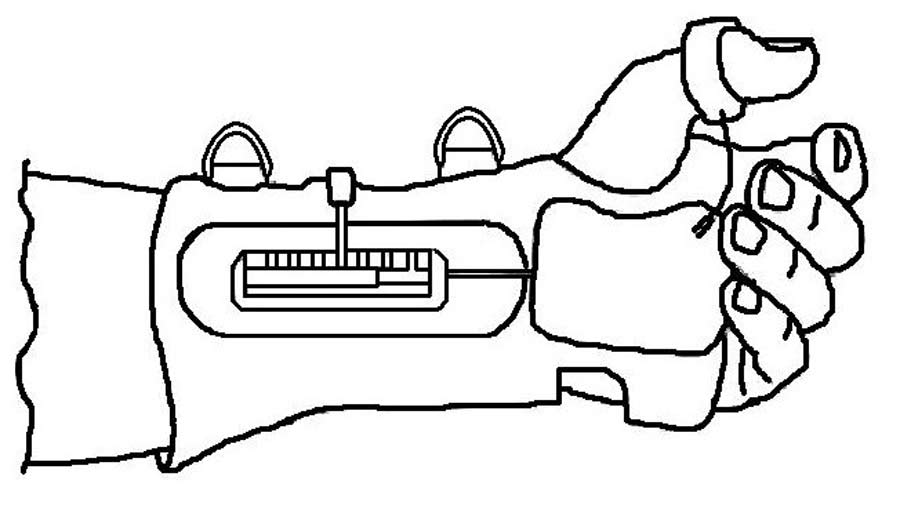 Figure 1 Line drawing (palmar view) of key grip orthosis fitted to a hand (Click image for larger view)
Figure 1 Line drawing (palmar view) of key grip orthosis fitted to a hand (Click image for larger view) Fitting And Adjustment For Use By Tetraplegics
All design developments were carried out in response to user feedback. A selected group of tetraplegics were involved in the developmental testing of the device prototypes to ensure that it met the end user’s requirements.
An orthosis that is to be worn as part of daily living should have low obtrusiveness and have good aesthetics to the target user group. It should also be possible for the user to independently don and doff the device so that they are not reliant on caregivers. The design and ease of use of the orthosis was tested with a selected group of potential users. Materials used were similar to sports equipment such as cycle gloves so that it would not look so different from other clothes commonly worn.
Reduced digital function was considered in the design of strapping systems and the cable adjustment mechanism. The straps may be tightened by hooking a finger through a rubber or plastic loop or even using teeth. The cable length adjustment may be carried out using gross arm movements against a hard surface to unlock and slide the latch mechanism and then relock it in place. The thumb can be manoeuvred into the ring by positioning the ring against a hard surface or possibly using teeth to grip it. The ring is covered in a soft material to facilitate this. The orthosis has since been patent protected (7). Figure 2 shows the orthosis being used to assist pen holding. It can be seen that the design is not obtrusive.
 Figure 2 Photograph of key grip orthosis being used to hold a pen (Click image for larger view)
Figure 2 Photograph of key grip orthosis being used to hold a pen (Click image for larger view)
EVALUATION
After proving the concept with selected volunteers a clinical trial of the device was developed to quantify the functional benefit that users can obtain from the device. A total of 25 participants at Burwood and Auckland, NZ Spinal Units will be used for the trial. These participants will undergo training in the use of the device and ½ hour hand class sessions five days per week for 6 weeks. Alternatively, outpatients will be required to utilise the device for a minimum of ½ hour per day for functional tasks in the home environment. Assessment of functional ability, both with and without the orthosis, will be carried out at the end of each week, using a specially design ADL assessment tool and also a pinch grip meter (Clinical Analysis System 1991,
Medical Research Ltd, UK). When measuring the force of the key grip, 3 readings will be taken and the average recorded. Participant safety will be assessed by the therapists who check for any skin marking by the orthosis. The assessment tool was developed to measure functionality using actual ADL tasks that represent a range of pinch force magnitudes and require the ability to assume a variety of proximal joint positions, hand postures and grasp openings (5). The ADL tasks used in this study are:
- opening and closing two types of zippers (one oriented horizontally and the other orientated vertically);
- inserting and removing an electrical appliance plug (using a NZ style plug);
- inserting and removing a key;
- inserting and removing an automated teller machine card;
- stabbing food with a fork;
- using a remote control button.
This resulted in 13 subtasks that were measured as being either achieved or not achieved: Remote Control; Fork + Putty; Card Out; Card In; Vertical Zip Open; Vertical Zip Close; Horizontal Zip Open; Horizontal Zip Close; Key Out; Key In; Key Turn; Electric Plug Out; Electric Plug In.
Figure 3 shows the tool developed to carry out the ADL assessments. It is packaged into a briefcase with integrated clamps for fixing onto a table to give stability.
 Figure 3 Photograph of assessment tool for measuring functional ability of the key grip. (Click image for larger view)
Figure 3 Photograph of assessment tool for measuring functional ability of the key grip. (Click image for larger view)
OUTCOME
Two participants have been fully assessed for a six week period, the first started the trial 6 weeks post injury and the second was approximately 20 years post injury. Both users could don and doff the gloves independently of their caregivers although some carer assistance was required if wearing thick winter clothes. Accuracy of self positioned orthosis alignment improved with practise over the 6 week period. The increased functionality that they achieved was significant (P < 0.0001). Pinch forces varied greatly over the 6 week period, so any increase in force achieved over time was not significant. However, there was a significant increase in pinch force when the orthosis was used compared with not used (P = 0.0002).
The number of functional tasks achieved for each participant was always more with the orthosis and there was no task that the orthosis hindered. A learning effect occurred over the six week period as the participants achieved more tasks both with and without the orthosis over time (P = 0.0029). Table 1 summarises the improvements in pinch force and number of tasks achieved when using the orthosis.
|
First participant |
Second participant |
||
|---|---|---|---|---|
|
Without orthosis |
With orthosis |
Without orthosis |
With orthosis |
| Pinch force (range) |
1 to 7 N |
3 to 14 N |
0 to 5 N |
4 to 7 N |
| Ratio of pinch forces |
1 : 2.4 (S.D. 1.2) |
1 : 2.6 (S.D. 1.1) |
||
| Number of tasks achieved in first week |
0 |
2 |
4 |
9 |
| Number of tasks achieved in 6th week |
4 |
11 |
6 |
10 |
IMPLICATIONS
The two participants varied considerably in terms of time since injury, but they both achieved a functional benefit from the device. Even though the first participant could produce twice the pinch force of the second (14 N compared to 7 N), they both achieved a similar number of ADL tasks (11 as compared to 10). The high number of tasks that the second participant achieved relative to their pinch forces is probably attributable to the more than 20 years of experience of tetraplegia.
The degree of MCP flexion of the index finger is critical to the development of a useful lateral key grip. The current orthosis does not have any component that maintains flexion of the index finger. Instead it relies on inherent flexion of the index finger when the thumb presses against it. If the index finger is extended, contact between the thumb and forefinger is lost. Methods may need to be developed to assist positioning of the index finger.
The assessment tool has been found to be a good hand class training tool as both users became more proficient at ADLs over time. Users reported that they would prefer to carry out hand therapy classes with such a tool that provides a realistic and positive learning experience.
NEXT STEPS
After clinical trial is completed in NZ then commercial manufacture and prescription of the orthosis will be developed.
ACKNOWLEDGEMENTS
We thank the tetraplegics who contributed to the design of the orthosis, especially Paul Stafford, the participants who have consented to the trial and the future participants who will take part in the ongoing trial, and The Foundation for Research Science and Technology (contract CO8X0404) and also Burwood Academy of Independent Living for funding the research.
REFERENCES
- Hanson, R. W., & Franklin, M. R. (1976). Sexual Loss in relation to other functional losses for spinal cord injured males. Archives of Physical Medicine and Rehabilitation; 57, 291-293.
- Moberg, E. (1978). The upper limb in tetraplegia: a new approach to surgical rehabilitation. Stuttgart: George Thieme.
- The 2004 Annual Statistical Report For The Model Spinal Cord Injury Care Systems; National Spinal Cord Injury Statistical Center, Birmingham, Alabama.
- Sollerman, C. & Ejeskar, A. (1995). Sollerman 1995 hand function test. A standardised method and its use in tetraplegic patients. Scandinavian Journal of Plastic and Reconstructive Surgery and Hand Surgery 29(2), 167-76.
- Smaby, N., Johanson, M. E., Baker, B., Kenney, D. E., Murray, W. M. & Hentz, V. R. (2004). Identification of key pinch forces required to complete functional tasks. Journal of Rehabilitation Research and Development. 41(2), 215-224.
- Swanson, A. B., De Groot Swanson, G. & Göran-Hagert, G. (1990). Evaluation of impairment of hand function. In J. M. Hunter, L. H. Schneider, E. J. Mackin, & A. D. Callahan (Eds.), Rehabilitation of the hand: Surgery and therapy (3rd ed., pp. 109–138). St Louis: CV Mosby.
- King, M. J., Le-Ngoc, L., & Verkaaik. J. (2006). An Orthosis - PCT International patent application PCT/NZ2006/000160 and NZ patent application 540912
Author contact information:
Marcus J. King, BE
Industrial Research Ltd.
P O Box 20028
Christchurch, 8053, New Zealand
Phone +64 3 3586810
Email: m.king@irl.cri.nz;
Highlights
- Source Ordered
- No Tables
- Very Compatible
Gargoyles
Disney produced a television show in the mid 1990s called Gargoyles. It's a great show and I'm a big fan. A few years ago Disney started to release the show on DVD. The last release was of season 2, volume 1. That was two years ago. Volume 2 has not been released. Why? Poor sales. So if you should find yourself wanting to support my work, instead I ask you pick up a copy of season 2, volume 1. It's a great show and you might find yourself enjoying it.