A New Hand-Held Strength And Range-Of-Motion Measurement Tool
Andrew B. Lintott, PhD1 ; Marcus J. King, BE1 ; Jason Nichols, BPhty2 ; Julian K.Verkaaik, BDes3
1 Industrial Research Ltd., NZ
2 Burwood Spinal Unit, NZ
3 Burwood Academy of Independent Living, NZ
ABSTRACT
A new measurement tool has been developed that is capable of measuring muscle strength and joint angle simultaneously, creating a profile of muscle strength throughout the range of motion. This type of measurement has not been available on a hand-held device previously. A clinical pre-trial has been carried out which concluded that the measurement was useful in assessing muscle strength in a clinical situation.
KEYWORDS:
dynamometer, physiotherapy, strength, range of motion
BACKGROUND
Strength and range-of-movement (ROM) are two key indicators of progress during rehabilitation. Changes in strength over time may indicate damage or healing of muscular or connective tissue, or the progress of a neurological or muscular disorder. Likewise, changes in ROM give the therapist insight into the level of recovery from injury, or progress of a disease.
Measurement throughout the ROM can give therapists insight into the nature, location and magnitude of an injury or impairment. Hand-held dynamometer devices are available that can measure strength isometrically (1) while larger devices exist that can measure strength isokinetically (2) however the cost of isokinetic dynamometers is prohibitive for many clinics.
CURRENT TECHNOLOGY
Physical therapists typically assess strength by manual muscle testing, which involves judging the resistance a patient can exert throughout their ROM. Scales such as the British Medical Research Council scale (MRC), or the Modified Oxford scale, which rate strength of an individual muscle on a point scale from zero to five, are used in assessments (Table 1). These scales lack the ability to track subtle changes in muscle strength which may have significant functional benefit for the patient. This is particularly evident within grades 4 and 5 on the Modified Oxford Scale. Inter-tester and intra-tester variability is a recognised problem with this type of testing and Van Tuijl et al. (3) discuss the difficulties of this approach in relation to spinal cord injury rehabilitation.
| Grading | Explanation |
|---|---|
| 0 | No Movement |
| 1 | Flicker |
| 2- | Incomplete RoM >50% gravity eliminated |
| 2 | Full RoM Gravity eliminated |
| 2+ | Incomplete RoM <50% against gravity |
| 3- | Incomplete RoM >50% against gravity |
| 3 | Complete RoM against gravity |
| 3+ | Complete RoM against slight resistance |
| 4- | Incomplete RoM >50% against moderate resistance |
| 4 | Complete RoM against moderate resistance |
| 5 | Normal |
Handheld dynamometers vary from metal, pneumatic, or hydraulic spring systems such as the B&L® Pinch Gauges or Martin Pneumatic Squeeze Dynamometer, to electronic systems such as the Chatillon® Electronic Push/Pull Dynamometer. These devices are often customised to suit particular joints such as the Jamar® Hydraulic Hand Dynamometer. The Hoggan Health MicroFET 2 dynamometer is capable of isometric strength measurements and features an electronic inclinometer for measuring ROM, although it does not measure both strength and ROM simultaneously.
The EVAL System is for analyzing hand and upper extremity movement and strength. Although it calculates impairment automatically and various tools (e.g., a pinchmeter, hand goniometer, upper extremity goniometer and a customized dynamometer) are used to provide electronic measurement of patient range of motion, pinch strength, and grip strengths, the system also does not compare strength across the range of motion of a joint.
ROM may be manually estimated as normal / deficient etc., or goniometers of various shapes and sizes can be employed to measure the angular range of motion. As well as the simple protractor type goniometers, there are various pendulum or bubble types such as the Baseline® Inclinometer and electronic versions such as the MicroFET 6 Range of Motion Inclinometer .
All of the devices mentioned so far require a hands-on measurement by the therapist and subsequent manual transfer of measurement data into patient records. The devices record only the peak force or the range of motion that the patient manages to achieve. If the capability of the patient over their range of motion is to be measured then a large dynamometer is required, such as the CSMi CYBEX or HUMAC NORM Testing & Rehabilitation System. Such devices are expensive, require a large amount of space to set up, require specialist therapist training to use and are time consuming to use in clinical practise.
There is no commercially available device that fits the intermediate need to measure patient strength over their range of motion and which can store patient records electronically in a database. An Australian research group developed a prototype hand-held dynamometer with integrated orientation sensors and trialled it on healthy subjects (4). The results were compared with those from an isokinetic dynamometer (KinCom) and it was found to provide information comparable to that obtained by isokinetic dynamometers at a fraction of the cost and size. Unfortunately that device consisted of three components that therapists had to manipulate along with the patient and it has not been commercialised.
May et al. (5) studied the intra-rater reliability of hand-held dynamometry and concluded that reliability is high and compares favourably with results from isokinetic dynamometry. The intra-rater correlation coefficient ranged from 0.89 to 0.96 while comparative tests with a Cybex dynamometer yielded a correlation coefficient of 0.52 to 0.88 which was statistically significant (p < 0.1). Dunn and Iverson (6) investigated inter-rater reliability of knee extensor and flexor muscle force measurements and found correlation coefficients of 0.87 to 0.93.
DESIGN AND DEVELOPMENT
 Figure 1: Photograph of dynamometer (Click image for larger view)
Figure 1: Photograph of dynamometer (Click image for larger view) We developed a new handheld measurement tool capable of recording strength over the full ROM of a joint to provide a richer and more consistent assessment of a patient’s condition. A patient’s strength throughout the range of motion is presented either graphically or numerically and may be uploaded to a computer for further analysis (Figure 1). An objective record of a patient’s functionality can be produced and compared over time. The dynamometer contains an electronic inclinometer as well as a load cell force pad so that it can record the muscle strength measurement simultaneously with respect to the joint angle. The dynamometer features a soft pad that is placed at a reference location on the limb such as a bony protuberance (Figure 2 part 1).
The patient is instructed to push against the pad with their full strength and the therapist controls the movement of the limb so that it travels as smoothly as possibly through the patient’s range of motion. The force exerted by the patient is recorded throughout the movement along with the angle of the device relative to the vertical axis. The dynamometer then displays a plot of force against joint angle as well as critical information such as peak force, joint angle at peak force, range of motion, deficit, angle at maximum extension, average joint velocity etc. The data can be stored on the device for comparison with previous or future recordings or with normative data. The working principle of the device is described in a world patent (7). The dynamometer can be applied to a wide variety of measurements including complex joint motions such as shoulder and spinal column movements.
EVALUATION
A clinical pre-trial of the device involved a series of measurements of a SCI patient by a final year physiotherapy student. Among the conclusions reached were that there was value in presenting the results graphically to the patient as a motivator and to aid understanding, and that the ability to store patient referenced data electronically and transfer it to a computer was useful.
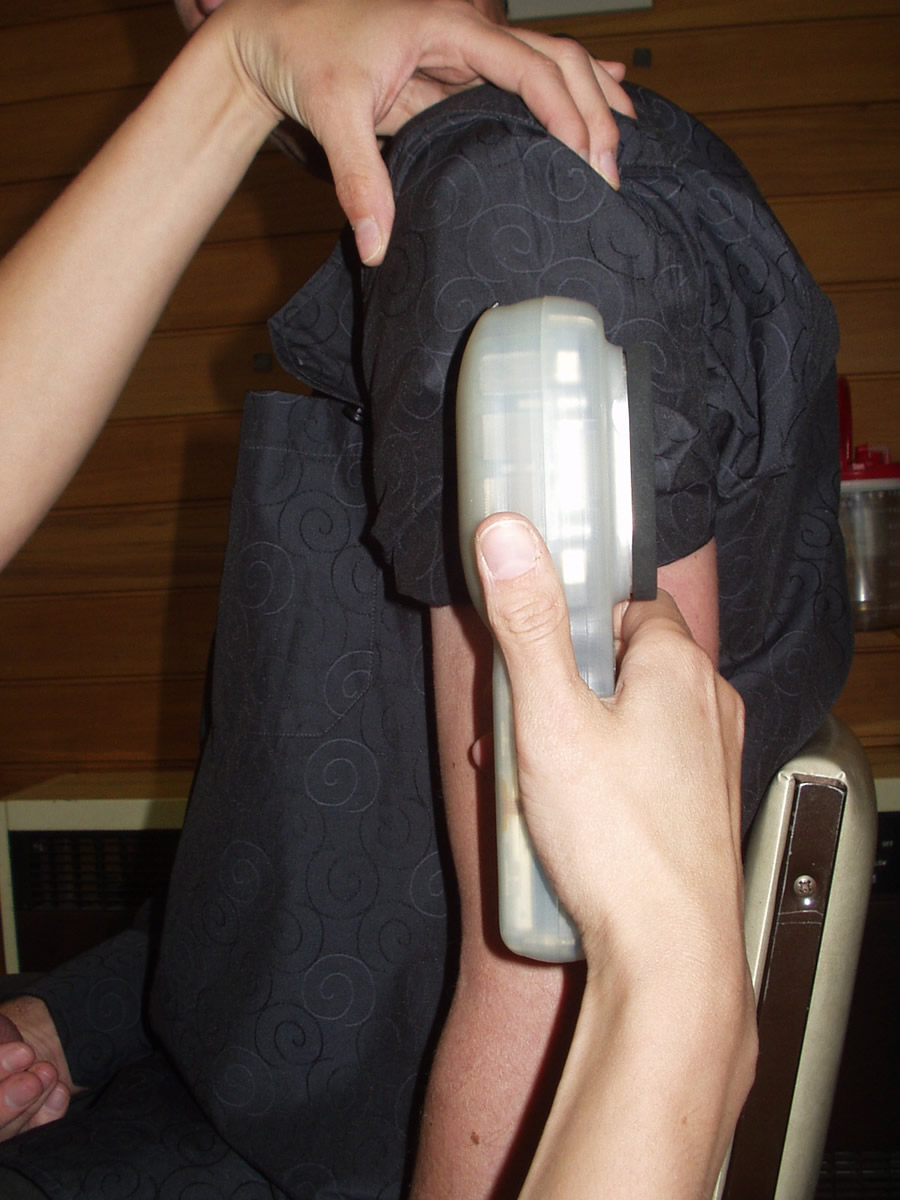 Figure 2a: Alignment with humerus. (Click image for larger view)
Figure 2a: Alignment with humerus. (Click image for larger view) In another trial the device was used to measure the post surgical recovery of function of an individual who had sustained a fracture dislocation of the radial head of the left arm. Heterotopic Ossification had occurred post injury resulting in the fusion of the radius and ulnar proximal heads which severely restricted elbow extension and prevented wrist supination and pronation. The device was used to measure changes in flexion contracture, extension contracture, pronation and supination following a second surgery to separate the radial and ulnar heads.
 Figure 2b: Placement at reference position at start of measurement. (Click image for larger view)
Figure 2b: Placement at reference position at start of measurement. (Click image for larger view) For the flexion contracture a reference plane was set for each recording by aligning the measurement axis of the dynamometer with the centre line of the humerus (Figure 2 part 1). The elbow was then extended to the maximum and the centre of the force pad placed against the bony protuberance of the distal radial head (Figure 2 part 2). The patient was then instructed to use maximum bicep exertion to move the elbow into maximum flexion (Figure 2 part 3). The therapist resisted the force by holding the device against the patient’s wrist and took care to allow the arm to move through its full range in a controlled manner, so that the speed of motion was reasonably constant and the patient could still exert maximum force during the movement. When the elbow was at maximum flexion, the measurement was stopped. Figure 3 shows a graph of the patient’s strength across the ROM for that movement measured at various times post the second surgery. Table 2 summarises the results of the various measurements carried out and provides a comparison with a conventional physiotherapist’s assessment of ROM.
 Figure 2c: Resisted flexion. (Click image for larger view)
Figure 2c: Resisted flexion. (Click image for larger view) Twenty days post operatively there was a marked improvement in active forearm pronation and supination with 70 degrees and 55 degrees respectively. Active elbow flexion range of motion improved to achieve 110 degrees of motion with a peak force value of 5.1Kg.
 Figure 3: Results of patient trial (Click image for larger view)
Figure 3: Results of patient trial (Click image for larger view) Thirty-six days post operatively there was a loss of active forearm pronation and supination of 12 degrees and 9 degrees respectively. Active elbow flexion range of motion continued to improve to achieve 126 degrees of motion with a peak force value of 7.1Kg.
Conventional measurements with goniometry at 20 and 36 days post operatively compared accurately to the angle measurements obtained from the device. Simultaneous recording of strength using the device showed significant improvements in force while the Modified Oxford scaling remained unchanged in this time period.
| Concentric Flexion | |||||
|---|---|---|---|---|---|
| Days post | Joint angle | Physiotherapists assessment | Force Max | ||
| surgery | Min | Max | Rng | ||
| 17 | 8 | 125 | 117 | 110 | 3 |
| 20 | 8 | 122 | 114 | 110 | 5.1 |
| 36 | 3 | 126 | 123 | 125 | 7 |
| Eccentric Flexion | |||||
| Days post | Joint angle | Force | |||
| surgery | Min | Max | Rng | Max | |
| 20 | 15 | 122 | 110 | 7.2 | |
| 36 | -2 | 122 | 124 | 8.2 | |
| Pronation | |||||
| Days post | Joint angle | ||||
| surgery | Min | Max | Rng | ||
| 17 | -3 | 57 | 60 | ||
| 20 | 0 | 59 | 59 | ||
| 36 | 0 | 58 | 58 | ||
| Supination | |||||
| Days post | Joint angle | ||||
| surgery | Min | Max | Rng | ||
| 17 | 3 | 48 | 45 | ||
| 20 | 0 | 55 | 55 | ||
| 36 | -2 | 51 | 53 | ||
IMPLICATIONS
A new measurement device has been developed that provides the simultaneous measurement of two key physical measurements: Strength and ROM, with the benefit of measuring the strength throughout the ROM. The diagnostic benefit of the data obtained has not been fully explored to date, however clinical trials will establish standardised procedures and build a background of clinical experience with the device. Hand held dynamometers have been shown to produce results comparable to an isometric dynamometer (5).
The device has the following key advantages:
- It provides a richer visual assessment of the strength profile of a muscle group or joint.
- Patient records can be easily stored, retrieved and compared over the rehabilitation period.
- It is easier to align and apply to the patient than traditional goniometers.
- It removes the need to visually read and note start and stop angles allowing the therapist to pay more attention to the patient, monitoring pain, effort, strain, and compensatory movements.
- Assessment is faster as both ROM and strength are measured in the same movement.
- Finer granularity of force is obtained (tenths of kilograms) compared to the Modified Oxford scale (0 to 5).
It should be noted that dynamometers, including the new device described in this paper, are not useful in measuring muscle strength for MRC scores below 3.5 because the patient must be capable of exerting force against resistance.
NEXT STEPS
To further develop this system of measurement, it is necessary to establish a set of standardised procedures for taking measurements. Pre-clinical trials have demonstrated the potential of the device and a clinical trial is planned to assess the practicality and clinical relevance of the measurements obtained. An upcoming study will evaluate the inter- and intra-rater variability and accuracy of the device by evaluating the performance of a group of physiotherapists as they measure an artificial arm with a known force-angle relationship. Commercialisation of the device is underway.
REFERENCES
- Anon. (2003). The Lafayette Manual Muscle Test System User’s Manual, Model 01163, Lafayette Instrument, IN, USA. http://www.lafayetteinstrument.com/Downloads/01163manual.pdf
- Bemben, M. G., Grump, K. J. & Massey, B. H. (1989). Assessment of Technical Accuracy of the Cybex II isokinetic dynamometer and analogue recording system. J Orthop Sports Phys Ther, 10, 12-17.
- Van Tuijl, J. H., Janssen-Potton, y. J. M. & Seelen, H. A. M. (2002). Evaluation of Upper Extremity Motor Function Tests in Tetraplegics, Spinal Cord, 40, 51-64.
- Li, R.C., Jasiewicz, J. M., Middleton, J., Condie, P., Barriskill, A., Hebnes, H. & Purcell, B. (2006). The Development, Validity, and Reliability of a Manual Muscle Testing Device With Integrated Limb Position Sensors. Arch Phys Med Rehabil. 87, 411-7.
- May, L. A., Burnham, R. S. & Steadward, R. D. (1997). Assessment of Isokinetic and Hand-Held Dynamometer Measures of Shoulder rotator Strength Among Individuals With Spinal Cord Injury. Arch Phys Med. Rehabil; 78, 251-5.
- Dunn, J. C. & Iverson, M. D. (2003). Inter-rater Reliability of Knee Muscle Forces Obtained by Hand-Held Dynamometer from Elderly Subjects with Degenerative Back Pain, J Geriatr Phys Ther, 26, 23-9.
- Le-Lengoc, L., Lintott, A. B., King, M. J., & Verkaaik, J. K. (2006). Angle and force measurement instrument. WO 2006/038822 A1
Author Contact Information:
Andrew B. Lintott, Ph.D.
Industrial Research Ltd.
P O Box 20028
Christchurch, 8053
New Zealand
Phone +64 3 3586844
Email: a.lintott@irl.cri.nz
Highlights
- Source Ordered
- No Tables
- Very Compatible
Gargoyles
Disney produced a television show in the mid 1990s called Gargoyles. It's a great show and I'm a big fan. A few years ago Disney started to release the show on DVD. The last release was of season 2, volume 1. That was two years ago. Volume 2 has not been released. Why? Poor sales. So if you should find yourself wanting to support my work, instead I ask you pick up a copy of season 2, volume 1. It's a great show and you might find yourself enjoying it.