Shoulder Joint Forces during Lateral and Overhead Wheelchair Transfers
Padmaja Kankipati, MS, Alicia M. Koontz, PhD, Megan Yarnall, BS
Human Engineering Research Laboratories, Highland Drive VA Medical Center, Pittsburgh, PA
Department of Rehabilitation Science and Technology, University of Pittsburgh, Pittsburgh, PA 15261
Department of Bioengineering, University of Pittsburgh, Pittsburgh, PA 15260
ABSTRACT
Wheelchair transfers have been associated with the high incidence of upper limb pain among persons with spinal cord injury. The focus of this study was to examine the shoulder joint forces during a lateral transfer and an identical transfer with the use of an overhead beam. Four persons with paraplegia performed each transfer while motion analysis equipment recorded their movements and force sensors recorded the forces applied by the hands. No significant differences were found between the forces at the shoulder of both the leading arm and trailing arm for both types of transfers. Overhead transfers, thought to be more detrimental to the shoulders, did not result in greater loading at the shoulders compared to lateral transfers. Further analysis should be carried out involving more subjects to confirm these findings.
KEYWORDS
Biomechanics, transfer, overhead, wheelchair, SCI.
BACKGROUND
People with lower limb dysfunction, like spinal cord injury, commonly have upper limb pain, due to their high reliance on their arms to perform activities of daily living such as wheelchair propulsion, pressure relief and transfers [1]. Any loss of upper limb function will severely affect their ability to function independently. There are different approaches that are used to perform transfer activities such as the lateral, front or back approach. The lateral transfer is the most common type of transfer and is most commonly favored since it is quick and requires less strength [2]. During a lateral wheelchair transfer, an individual lifts the buttocks by pushing off of the armrests, wheelchair seat, frame or wheel and then swings the buttocks and trunk over to an adjacent surface. Very little literature is available concerning a ‘pulling’ type shoulder task which is the case for an overhead transfer in which the applied force is directed toward the body. However performing forceful tasks with the arms positioned overhead is thought to predispose the shoulder to injury such as impingement [3]. A study by Das et al. [4] examined isometric pull and push strengths in persons with paraplegia for normal, maximum and extreme working reach envelopes. The findings of this study suggests that pulling with the arm vertically overhead may more efficiently recruit larger muscles of the proximal shoulder like the bicep, pectoralis major and deltoid muscles which may protect the joint from impingement since less depressive force is needed to stabilize the joint in this position.
The purpose of this study was to compare the forces at the shoulder between a lateral, level wheelchair to bench transfer (pushing technique), and the same transfer where one arm reaches overhead (employing a pulling technique) during the transfer. This analysis will help in identifying potential techniques that may prevent shoulder injury due to wheelchair transfers.
METHODS
Subjects:
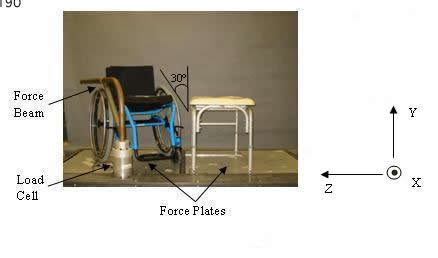 Figure 1. Experimental setup (Click image for larger view)
Figure 1. Experimental setup (Click image for larger view) After reading and providing informed consent, four male subjects with SCI (Table 1), who satisfied the inclusion criteria and signed informed consent, participated in this study. The inclusion criteria were: spinal cord injury between L2 and T1 ASIA A or B that occurred over one year prior to the start of the study, able to independently transfer to/from a manual wheelchair without human assistance or assistive devices, over 18 years of age, and free from upper extremity pain that influenced their ability to transfer. The mean (± standard deviation) age of the subjects was 35.50 (± 9.6) years and the mean time since SCI was 14.06 (± 9.02). The subject weight and height were 75.41 (± 18.33) kilograms and 1.82 ((± 0.13) meters.
Subject |
Age (yr) |
Weight (Kg) |
Height (m) |
Duration of Injury (yr) |
Injury Level (yr) |
|---|---|---|---|---|---|
1 |
38 |
78.93 |
1.73 |
13.25 |
T11-T12 |
2 |
33 |
63.96 |
1.73 |
11.5 |
missing |
3 |
24 |
99.79 |
2.01 |
5.0 |
T8 |
4 |
47 |
58.97 |
1.83 |
26.5 |
T4 |
Mean (SD) |
35.50 (9.6) |
75.41 (18.33) |
1.82 (0.13) |
14.06 (9.02) |
T4-T12 |
Experimental Protocol:
Participants used their personal wheelchairs to transfer to and from a bench. For both types of transfer the wheelchair was positioned and secured at and angle of 30 from an adjustable tub bench as shown in Figure 1. The tub bench was adjusted to be level with the subject’s wheelchair seat. The platform shown in Figure 1 contains two force plates (Bertec Corporation, Columbus, OH), one beneath the wheelchair and one beneath the tub bench. The wheelchair and bench were secured to the platform. A steel beam attached to a 6-component load cell (Model MC5 from AMTI, Watertown, MA) was used to simulate a wheelchair armrest or an overhead grab bar. Reflective markers were placed on the subjects C7 and T3 vertebrae, right and left acromion processes, 3rd metacarpalphalangeal joints, radial and ulnar styloid processes, and lateral epicondyles. The coordinates of the markers were recorded based on a global reference frame using a six camera three-dimensional motion capture system (Vicon Peak, Lake Forest, CA). Several anthropometric measurements were recorded such as: axillary arm, wrist, fist and elbow circumference, upper arm and forearm length.
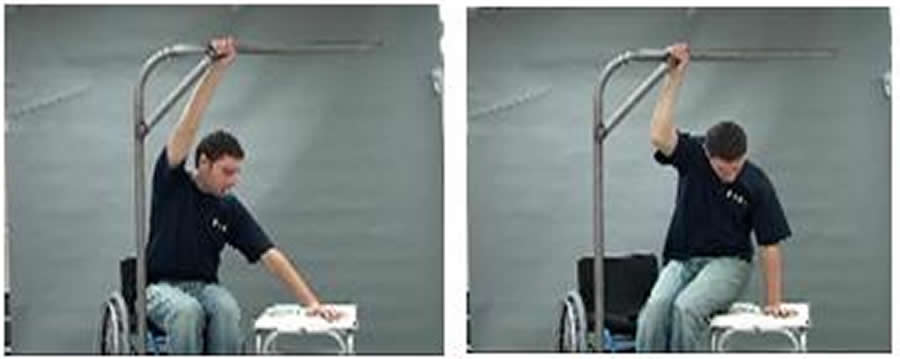 Figure 2. Still photos from the transfer instruction video for the overhead transfer. (Click image for larger view)
Figure 2. Still photos from the transfer instruction video for the overhead transfer. (Click image for larger view) Both the transfers began with the left arm leading and moving the body from the wheelchair to the tub bench. The first transfer performed by the subject was the self selected transfer. Subjects were instructed to transfer to the adjacent level tub bench, placing their left hand anywhere on the bench and right hand on the steel beam (height of wheelchair arm rest). The second transfer was an overhead transfer and the subjects were shown an instructional video describing step by step procedure to be followed. The overhead beam used in the transfer is shown in Figure 2; however it was oriented according to subject’s preference. Subjects were then allowed to practice before recording the transfer. Each transfer technique was performed three times and recorded at 60 Hz for the length of the transfer.
Data Analysis:
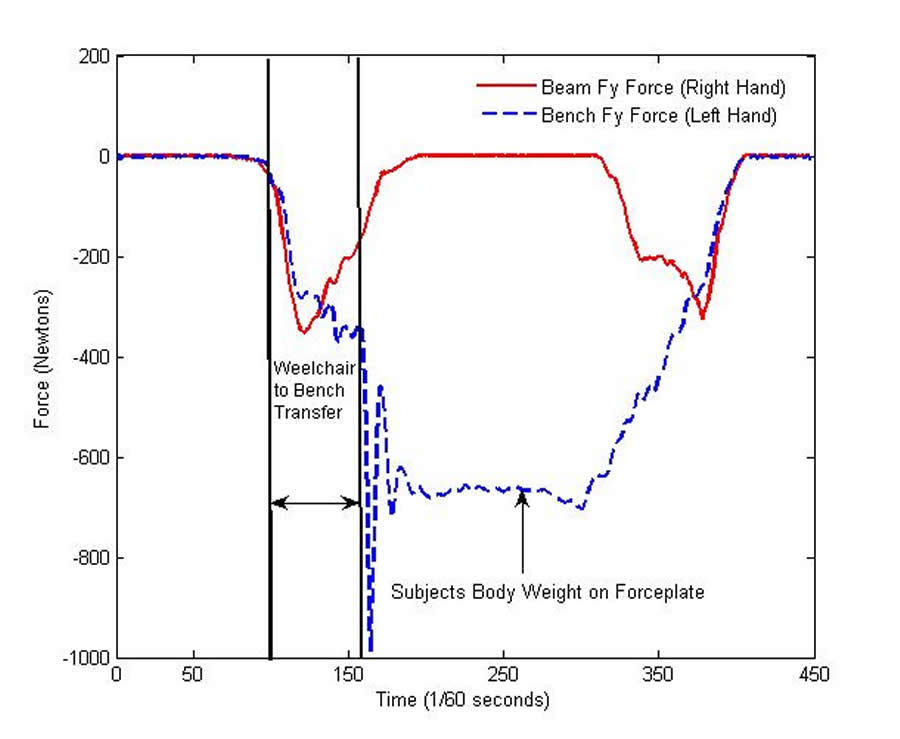 Figure 3. Representative self selective transfer recording of vertical forces of the force sensing beam and the force platform (bench force) to determine the wheelchair to bench transfer (Click image for larger view)
Figure 3. Representative self selective transfer recording of vertical forces of the force sensing beam and the force platform (bench force) to determine the wheelchair to bench transfer (Click image for larger view) Kinetic, kinematic, and anthropometric data were entered into an inverse dynamic model to calculate the net shoulder joint force and moment. The inverse dynamic model used was based on the general rigid-link segment model using a Newton-Euler method and a variable degree of freedom body co-ordinate system [5]. The beginning and the end of each transfer was determined from the vertical force data from the force plate under the tub bench and the force sensing beam. The increase of the forces followed by the decrease determines the duration of the transfer as shown in Figure 3.
Maximum forces for each shoulder component and resultant force for both the leading and trailing arm were calculated for each transfer to the tub bench. Variables were computed using Matlab (Mathworks, Inc., Natwick, MA). Group means and standard deviations were determined.
Statistical Analysis:
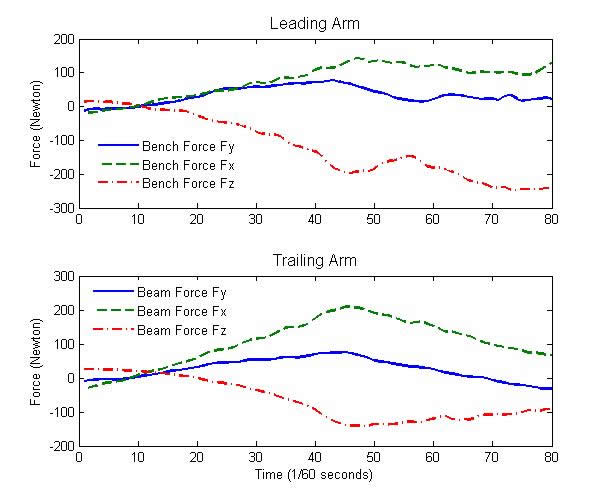 Figure 4. Forces at the shoulder for a self selected transfer (Click image for larger view)
Figure 4. Forces at the shoulder for a self selected transfer (Click image for larger view) Differences between the two types of transfers as well as between the leading and trailing arms were evaluated using a Wilcoxon Matched Pairs signed rank tests. The statistical tests were performed using SPSS statistical software (SPSS Inc., Chicago, IL). The level of significance was set at 0.05.
RESULTS
The forces from one representative subject for each of the three shoulder co-ordinate representations, for both the trailing and leading arm, are shown in Figure 2. The mean and the standard deviations of the maximum forces at the shoulder for the three co-ordinates (for both the trailing arm and leading arm), for each transfer type are presented in Table 2. There were no significant differences found between the two types of transfers or between the leading and trailing arms for each transfer. The anterior to posterior forces at the shoulders of both the leading and trailing arm for the overhead transfer were found to be lower as compared to the self selected transfer, as well as the compressive forces at the shoulder of the leading arm for the overhead transfer were found to be lower as compared to the self selected transfer, but they were not significant.
| Type of Transfer |
Arm |
Glenohumeral Joint to Acromion |
Acromion to Glenohumeral Joint |
Anterior to Posterior |
Posterior to Anterior |
Compressive (N) |
Distractive (N) |
Resultant Force |
|---|---|---|---|---|---|---|---|---|
Self Selected |
Trailing Arm |
65.15 |
37.86 |
219.41 |
33.16 |
148.07 |
29.21 |
267.93 |
Leading Arm |
80.47 |
29.43 |
200.67 |
23.11 |
14.96 |
266.40 |
336.95 |
|
Overhead |
Trailing Arm |
92.4 |
17.34 |
228.32 |
6.86 |
91.67 |
17.90 |
258.09 |
Leading Arm |
176.96 |
6.64 |
276.11 |
6.64 |
14.33 |
140.15 |
334.56 |
DISCUSSION
This study investigated shoulder joint loading for two types of transfers: self selected transfer and the overhead transfer. Although overhead shoulder activities are believed to elevate the risk for shoulder problems, we found that the overhead transfer technique employed in this study did not result in higher forces at the shoulder compared to the subjects preferred method of transferring. This study, however, cannot draw any definitive conclusions due to low statistical power (e.g. small sample size) and the high variability in the shoulder force data, particularly for the overhead transfer. Only three trials were analyzed after a short training/practice period which may not be representative of a longer experience using overhead techniques. There were also three individuals in this study who were far out from injury and may have optimized their self-selected technique for minimizing shoulder loads [6]. We found that for the subject who has had an injury for the shortest period in the group, approximately five years, there is a considerable decrease in the vertical reaction force at the shoulder of the trailing arm in the overhead transfer as compared to the self selected transfer. Transferring techniques may be dependant on a number of factors such as height, weight, level of injury, and duration of injury. Many biomechanical factors have been found to manipulate the ability to transfer such as the arm length, muscle strength and hand placement [7]. These factors should be considered in future analysis. Further study analyzing average forces, involving more subjects and other variables such as torque at the shoulder will help the analysis. Other factors that require further examination are the influence of individual characteristics such as body mass, level of SCI, duration of injury, balance control, and body anthropometry on shoulder joint loading during transfers.
REFERENCES
- Davidoff G, et al. (1991). Compressive mononeuropathies of the upper extremity in chronic paraplegia. Paraplegia, 29, 17 24.
- Somers MF, Spinal cord injury functional rehabilitation, 2nd Ed., Prentice-Hall,Inc., Upper Saddle River, NJ 2001.
- P. Herberts, R. Kadefors, C. Hogfors and G. Sigholm, Shoulder pain and heavy manual labor. Clinical Orthopaedics & Related Research 166-178 (1984).
- Das B., and Black N. L (2000). Isometric pull and push strengths of paraplegics in the workspace: 1. Strength measurement profiles. Int J Occup Saf Ergon 6, 47-65
- Cooper, R.A., Boninger, M.L., Shimada, S.D., Lawrence, B.M. (1999) Glenohumeral joint kinematics and kinetics for three co-ordinate system representations during wheelchair propulsion. American Journal of Physical Medicine and Rehabilitation, 78(5), 435-446
- Finley MA, McQuade KJ, & Rodgers MM. Scapular kinematics during transfers in manual wheelchair users with and without shoulder impingement. Clinical Biomechanics 2005:32-40
- Allison,GT, Singer KP, and Marshall RN Transfer movement strategies of individuals with spinal cord injuries. Disabil.Rehabil (1996); 18: 35-41.
ACKNOWLEDGEMENTS
Funding for this study was provided by the VA Rehabilitation Research R&D Services and the National Institute on Disability and Rehabilitation Research and the National Institute of Health (VA-RR&D E3589V and B3079R NIDRR H133A011107, NIH R49/CCR310285-06).
Padmaja Kankipati
Human Engineering Research Labs
VA Pittsburgh Healthcare System
Pittsburgh, PA 15206
Phone: (412) 365-4829
Fax: (412) 365-4858
Email:kankipatip@herlpitt.org.
Highlights
- Source Ordered
- No Tables
- Very Compatible
Gargoyles
Disney produced a television show in the mid 1990s called Gargoyles. It's a great show and I'm a big fan. A few years ago Disney started to release the show on DVD. The last release was of season 2, volume 1. That was two years ago. Volume 2 has not been released. Why? Poor sales. So if you should find yourself wanting to support my work, instead I ask you pick up a copy of season 2, volume 1. It's a great show and you might find yourself enjoying it.