Garet Gamache, Joey Pitzo, Brian Talbot, Eric Zettergren, Jodi Abramowitz, Katelyn Bergeron, Sarah Martyn, and Kathleen Masters
ABSTRACT:
The purpose of this project was: 1) To design and build a power wheelchair controller to meet the needs identified by a consumer consultant; and 2) To identify important procedural elements to guide future projects utilizing interdisciplinary, consumer-engaged research and development (R&D). Multiple data sources were used to guide the inductive process of developing a successful AT outcome. Qualitative analysis of meeting notes and pre/post project student surveys revealed the procedural guidelines used to bring this work to successful completion.
Keywords:
Interdisciplinary, consumer-engaged, power wheelchair, controller
BACKGROUND/STATEMENT OF THE PROBLEM
The idea for this project grew out of a need expressed by a consumer to obtain a more functional controller for his power wheelchair and the desire of physical therapy (PT) and electrical/computer engineering (ECE) faculty to develop an interdisciplinary Capstone course for seniors in each program to help students understand the value and challenges of interdisciplinary research and design (R&D). Four PT and four ECE students elected to participated in the project. The consumer participant is a 39-year-old-man who is a husband, father of two children, self-employed hip-hop artist, motivational speaker, and disability advocate. He has a diagnosis of spastic/athetoid quadriplegic cerebral palsy (CP), which is characterized by dysfunction of the basal ganglia and typically associated with impairment of postural reflexes, the presence of arrhythmic involuntary movements and dysarthria. Sensation, ocular control and intelligence are generally within normal limits (1). All of these characteristics were true for this consumer.
The consumer reported numerous problems with his previous controller, which was a heavy duty joystick. In order to operate it, he had to remove his right shoe. This served two purposes. First, operation required fine motor control, which he provided with his toes. Second, the joystick was four inches high as mounted on the wheelchair footplate. This positioning required him to place the right shoe under his heel so that he could be level with the controller. Another problem was related to New England weather. Driving without wearing a shoe was particularly unfavorable in the winter months. Further, the joystick was not weatherproof and had a tendency to short out when he used the wheelchair in inclement weather.
Based upon problems identified, we had two goals for this project: 1) Design and build a flush-mounted, weatherproof, and reliable controller that the consumer could operate while wearing his shoe; and 2) Capture the processes and procedures used in this project for the benefit of future projects of this kind.
METHODS
We used an inductive, interdisciplinary, consumer-engaged research design to conduct this project. It required an early emphasis on “cross-cultural” (PT, ECE, consumer) education until a common language and collaborative plan emerged. Several data sources were used, including the results of a PT exam; a search of manufacturers’ websites and the patent registry; a meeting with the regional representative of the consumer’s wheelchair manufacturer; conference calls with the manufacturer’s technical group; peer-reviewed literature related to the project; meeting notes and pretest/posttest survey results to capture the procedural elements we identified as important to the success of projects like ours. We used multiple sources of data because potential weaknesses in any one source can be overcome by the others (2).
At the start of the project, the PT students performed a seating and mobility assessment. Major concerns identified included a severe increase in muscle tone throughout his body, left side greater than right; presence of symmetrical and asymmetrical tonic neck reflexes, and decreased motor control throughout. In spite of significant physical impairments, the consumer is independent in all activities of daily living and demonstrates safe, independent mobility in the community with his power wheelchair. The consumer uses his right lower extremity for all activities, including driving the wheelchair, typing, pushing elevator buttons, and accessing objects within his reach. He uses his upper extremities, which are quite limited in range of motion, as stabilizers. He demonstrates mild dysarthria but is able to communicate effectively. As stated above, the consumer was propping his right foot on top of his shoe in order to operate the joystick of his wheelchair, and this caused asymmetry in his sitting posture, increasing the risk of advancing existing musculoskeletal deformities.
The PTs shared pertinent findings with the team who synthesized this information and brainstormed ideas to identify controller designs that might work. No commercially available options were available. Early meetings were frequent, designed to share information and progress, gather feedback, and revise plans. Over time, role delineation and interdependency developed among the team members. The PT students assumed the role of ensuring that the consumer’s physical and functional abilities remained in the forefront, while the ECE students developed the design ideas and built the device. The consumer provided his input, concerns, preferences, and design recommendations.
The ECEs communicated with technicians from the manufacturer of the consumer’s wheelchair, professors, and experts in industry and made suggestions based on that feedback. The first step was to identify an appropriate sensor. Hall effect sensors, optical sensors, pressure sensors were ruled out because of the complexity involved in integrating them with the consumer’s wheelchair. Sip ‘n puff, a proven controller technology, was a viable option but the consumer refused this based upon aesthetic concerns. Strain gauges were chosen because they can be used to sense very minute measures of strain, a property that was desirable given the consumer’s physical impairments. They also possess the benefits of being inexpensive and small. The next step was to identify a processor capable of making decisions based on the input from the sensors. Requirements included the need for six analog and digital input/output ports and the lowest possible power demand (because the processor would draw power from the wheelchair batteries). The Cypress PSoC microprocessor was selected as it fit all of the requirements.
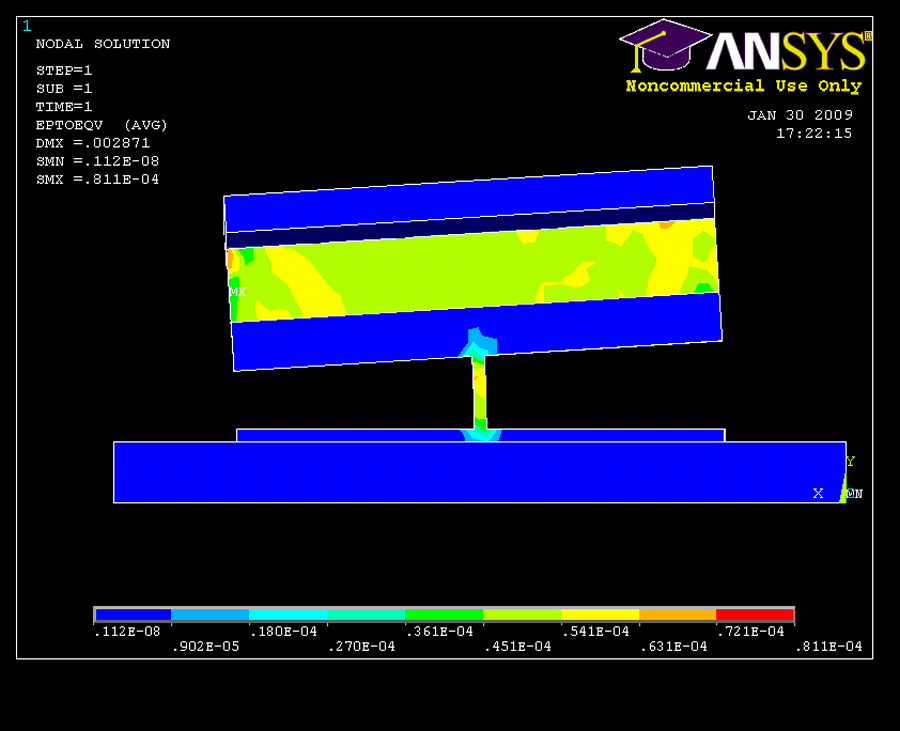
Next we considered materials for the sensor “block” because strain gauges must be matched to the mounting material. Anodized aluminum was chosen because it is weatherproof, flexible and has a high strength to weight ratio. Perpendicular I-beams were cut into a cube of aluminum in order to achieve flex in four directions. To determine the beam width and block size, we used a program called ANSYS, which measures the strain on an object given an input force (in this case the human foot). Figure 1 shows the ANSYS results with “front left” input to the block. The increase in strain is represented in both I-beams with a color mix of green and yellow, showing greater strain in this area compared to the blue areas.
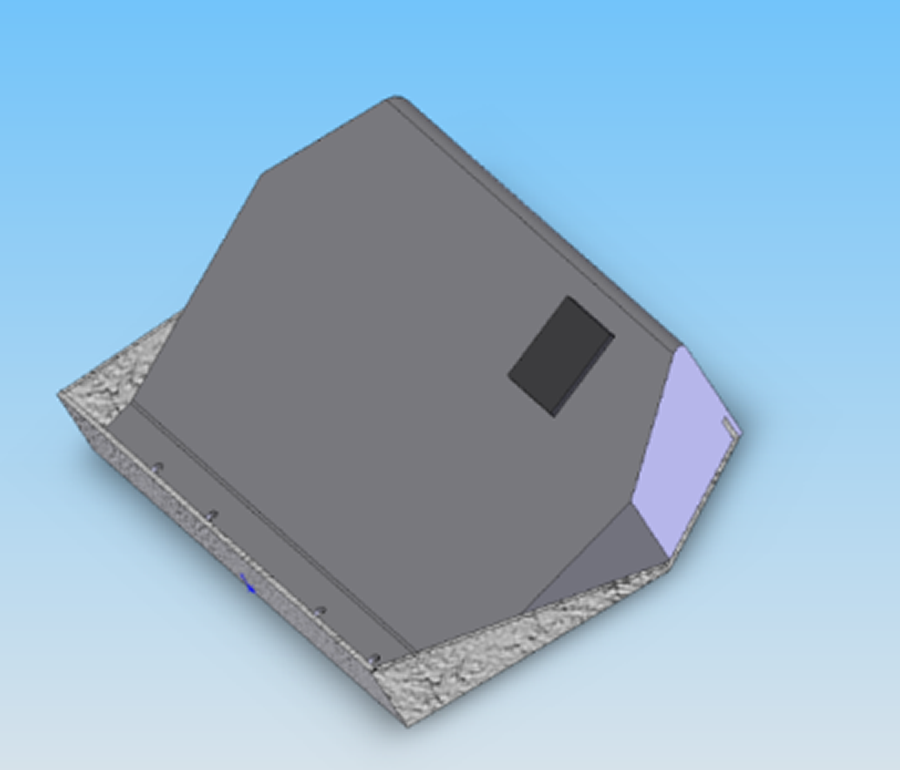
We created a new footplate for the consumer in order to meet the goals of weatherproofing and improved positioning. We chose stainless steel and designed it to enclose the circuit board and sensor block and caulked any open areas to make the whole design weatherproof. A solid works drawing of the footplate is shown in Figure 2. The dark gray area represents the sensor block, which is flush with the top. The footplate is angled to promote better posture and to provide a “catch” at the rear of the plate for storing personal items without risk of them falling off of the plate.
RESULTS
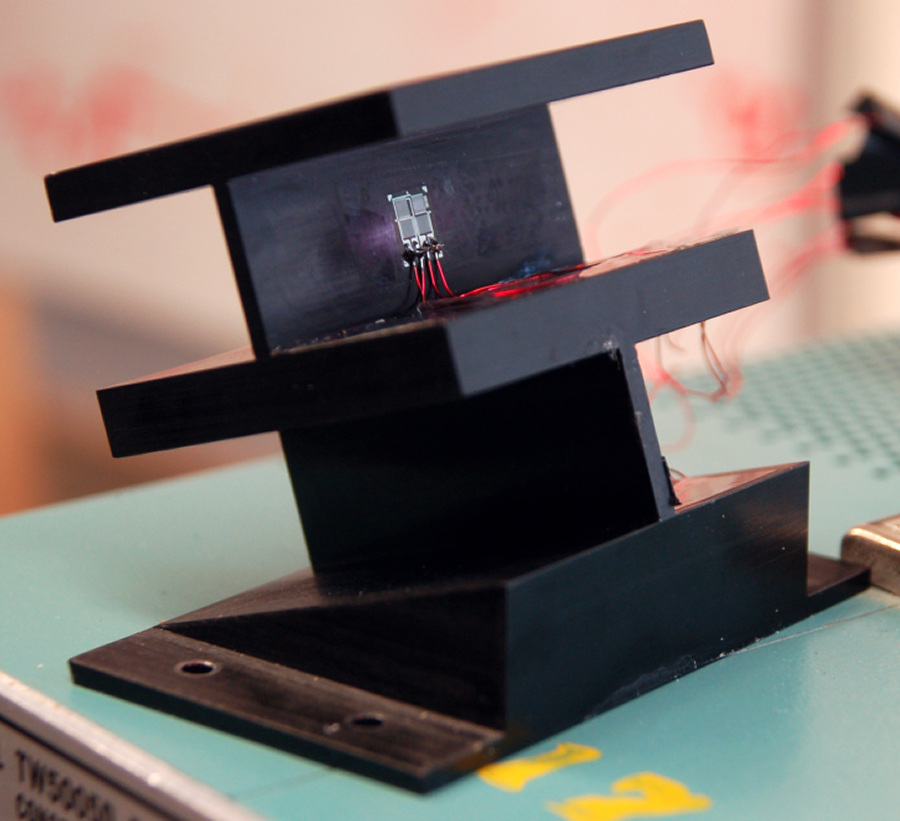
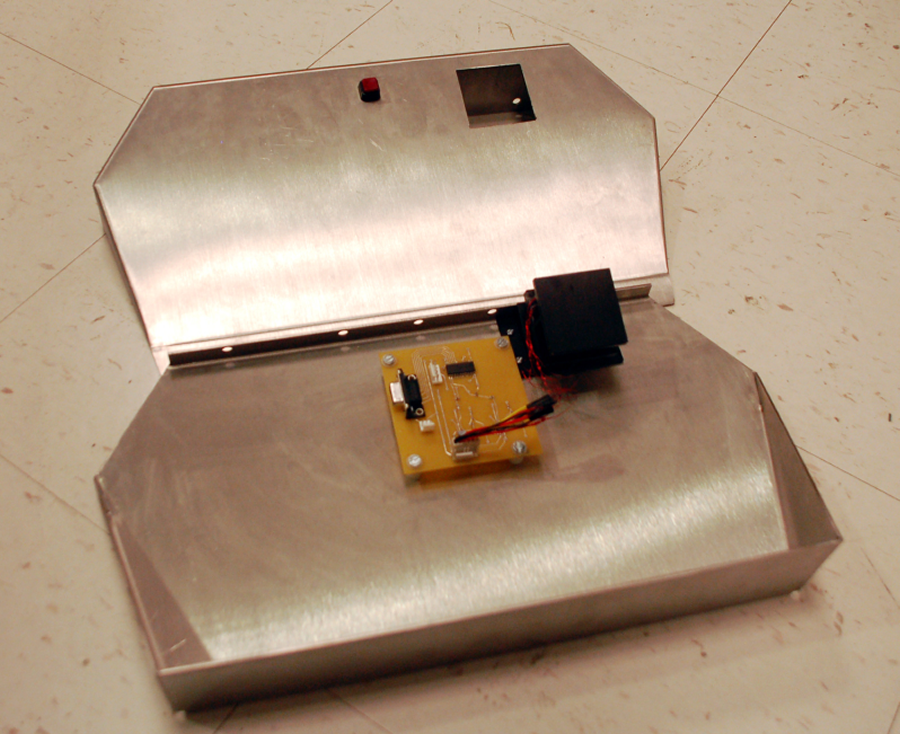
The final built design of the new controller is shown in Figure 3 and Figure 4 shoes the controller mounted in the customized footplate. It is weatherproofed and provides a symmetrical, solid platform for the consumer’s feet, which will help to minimize the risk of worsening existing musculoskeletal deformities. The consumer is able to drive with his shoe on because the controller is responsive to his available motor control as applied through a shoe, requiring only rotation of the ball of his right foot.
The following guidelines emerged from qualitative analysis of the meeting notes and our responses to the pre/post project surveys. The importance of communication was the most common theme. It included the need to communicate ideas in a way that everyone could understand, in the most timely manner possible, using all means available (primarily email and cell phones). We also determined that it would be helpful to teach each other early on about what each of our disciplines can contribute to the project. We found it helpful to establish a schedule of mutually available meeting times for each semester, but it was also important to remain flexible to meet more or less often, depending on the progress or unanticipated delays of collaborators. Finally, we discovered the importance of developing collaborative goals as quickly as possible and checking often to ensure that all collaborators were working toward them.
DISCUSSION
Interdisciplinary collaboration was a key component in this project. It helped us ensure that the consumer’s needs were met in an effective manner that considered many aspects of his physical function, history, and lifestyle. Research has shown that interdisciplinary work can be difficult to accomplish unless specific measures are taken to avoid potential barriers (3). A supportive infrastructure is needed to facilitate communication and understanding in order to identify shared project goals as early as possible in the process. We found that each member of the team needed to possess openness to the ideas of others, and that all members had the opportunity to make valuable contributions to the project. Our work included several meetings per semester that involved the consumer, students, and mentors. Numerous challenges arose, including time constraints, initial struggles with communication of ideas across disciplines, and maintaining a focus on the consumer’s physical and personal needs, rather than the project. The team worked through these effectively to achieve a successful result.
REFERENCES
- Amor, D. J., Craig, J. E., Delatycki, M. B., & Reddihough, D. (2001). Genetic factors in athetoid cerebral palsy. Journal of Child Neurology, 16(11), 793-797.
- Patton, M. Q. (2002). Qualitative research and evaluation methods. Thousand Oaks, California: Sage.
- Choi, B.C. (2007). Multidisciplinarity, interdisciplinarity, and transdisciplinarity in health research, services, education and policy: 2. Promotors, barriers, and strategies of enhancement. Clin Invest Med, 30(6), E224-232.
| Sensor Block | $285.00 |
| PCB and Components | $100.00 |
| Strain Gauges | $12.00 |
| Stainless Steel Footplate | Donated |
| Labor to Construct Sensor Block | Donated |
| Manufacturer Consultation | Donated |
| Total | $397.00 |
COST AND ACKNOWLEDGEMENTS
We were able to stay within the budget provided by the university. In addition, the costs for the new footplate and cutting the aluminum block into I-beams were offered as in-kind services as outlined in Table 1.
Contact:
Garet Gamache at ggamache@gmail.com or 401-378-4478