Jing Wang, Dan Ding, Harshal P. Mahajan, Ashlee B. Filippone, Pamela E. Toto, Michael P. McCue
Department of Rehabilitation Science and Technology, University of Pittsburgh, PAABSTRACT
Assistive technology for cognition (ATC) has provided new ways to serve people with cognitive disabilities in completing ADLs independently. The objective of this pilot study is to evaluate the effectiveness and preference of different types of prompts used in ATC to assist people with traumatic brain injury (TBI). Four types of prompts: verbal, light, image and smart glass were tested to guide people through common kitchen tasks. Five adults with TBI participated in this pilot study. Participants were asked to complete retrieving items using four types of prompts. The completion time, preferences and the neuropsychological status of each participant were accessed. Results showed that image and smart glass were most preferred by participants while verbal prompts were least preferred. Image prompts seemed the most efficient while verbal prompts seemed to be the least efficient type to assisting participants to complete multistep tasks in this study.
Introduction
Each year, approximately 1.7 million people in the United States sustain a traumatic brain injury (TBI) (Faul, Xu, Wald, & Coronado, 2010). Survivors of TBI usually suffer from various cognitive deficits such as problems with memory, attention, planning and executive functions (Sohlberg & Mateer, 2001). These cognitive deficits can limit an individual from completing activities of daily living (ADLs) independently, including cooking, dressing, and cleaning, etc. Among ADLs, cooking tasks have been identified as essential skills for living independently (Graves, Collins, Schuster, & Kleinert, 2005; Horsfall & Maggs, 1986; Mechling, 2008; Schuster, 1988), which can play an important part in an individuals’ overall health implications, accomplishment in social roles, self-esteem and sense of control (Schuster).
For the past two decades, clinical interventions with incorporated computer science and other advanced technology, often referred to as assistive technology for cognition (ATC), have provided new ways to serve people with cognitive disabilities in completing ADLs independently (Bergman, 1998; LoPresti, Mihailidis, & Kirsch, 2004). Though verbal prompts have been predominantly used in ATC for a long time (Mihailidis & Fernie, 2002; Van Tassel, Bouchard, Bouchard, & Bouzouane, 2011), several different types of prompts currently have started to be used for prompting multistep tasks like cooking, such as image prompts and video prompts (Lancioni et al., 2011; Mechling & Gustafson, 2009). However, due to the prevalence of ATC studies being mainly directed towards scheduling devices and sensor technology, the information about effectiveness of different types of prompts in guiding multistep tasks is relatively scarce (Gottfried, 2009; LoPresti et al., 2004; Van Tassel et al., 2011; Wherton & Monk, 2008). Providing prompts that are not optimized with the cognitive levels of users and the characteristics of the tasks can significantly affect the efficiency of ATC (Van Tassel et al., 2011), decrease user satisfaction and lead to a high abandon rate of the ATC devices (Phillips & Zhao, 1993; Verza, Carvalho, Battaglia, & Uccelli, 2006).
The objective of this pilot study is to help fulfill the aforementioned gap in research by evaluating the effectiveness and preference of four types of prompts in assisting individuals with TBI in the completion of kitchen tasks. The types of prompts are verbal, light, image, and smart glass.
Methods
Participants
This study was approved by the University of Pittsburgh Institutional Review Board. Participants were recruited from the local TBI support groups. Inclusion criteria consisted of 1) over the age of 18; 2) having a self-reported diagnosis of TBI; 3) having difficulties in kitchen tasks based on the self-report; and 4) capable of understanding the objectives, risks, voluntary nature and procedures of this study. Individuals who had severe mobility, visual, or hearing impairments that would prevent them from receiving the prompts were excluded from this study.
Five adults with Traumatic Brain Injury participated in this study. Their subject IDs were CI01, CI02, CI03, CI04, and CI06. The participants range in age from 31-63 (Mean=47.2, SD=14.4), and four were male. Their duration post brain injury was 15.6±14 years. Participants CI02 and CI03 lived in group homes and other three participants lived in community. Two of the participants (CI01 and CI04) had their highest education in vocation/technical school and the other three had a GED or high school diploma. All participants could walk without using any mobility assistive technology.
Settings
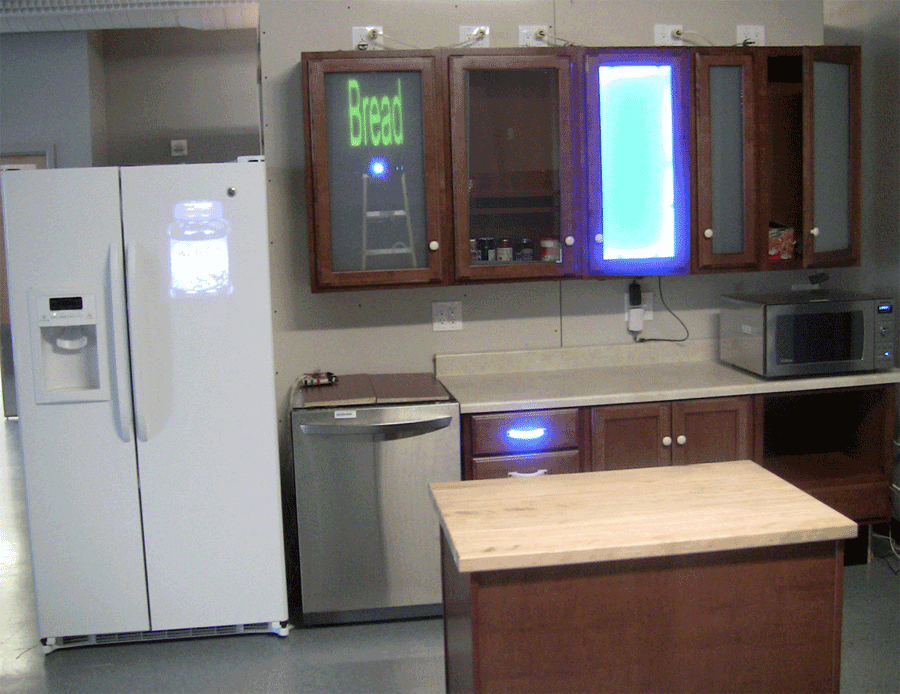 Figure 1 The experimental settings used in this study. This is the kitchen test-bed implemented with sensors and prompts. The image on the refrigerator showing that the jelly is in the refrigerator is an example of the image prompts. The glass of the second left cabinet becoming transparent is a smart glass prompt. The lighted door of the middle cabinet and the glowing handle of the top drawer show examples of the light prompts.
Figure 1 The experimental settings used in this study. This is the kitchen test-bed implemented with sensors and prompts. The image on the refrigerator showing that the jelly is in the refrigerator is an example of the image prompts. The glass of the second left cabinet becoming transparent is a smart glass prompt. The lighted door of the middle cabinet and the glowing handle of the top drawer show examples of the light prompts.
A kitchen test-bed has been implemented with four types of automated prompts to assist people with cognitive impairments through common kitchen tasks (Fig. 1). In this test-bed, verbal prompts can be played through computer speakers; light prompts are in the form of illuminated cabinets and handles; image prompts are projected on the cabinets or refrigerator; and smart glass implemented in the glass doors of cabinets can switch between transparent and opaque, to show the location of the target item. For verbal prompts, both the name of an target item (e.g. a can of tomato soup) and the location of that item (e.g. the middle cabinet) are provided verbally. For light, image and smart glass prompts, only the names of target items are provided verbally. All of these prompts can be controlled by the software system. Multiple contact switch sensors are deployed in the kitchen to log user activities information.
Protocol
Participants completed a questionnaire to elicit demographic and kitchen experience information. They were then oriented through the test kitchen and the four types of prompts. The study protocol was composed of two sessions.
In session #1, participants were required to retrieve items for recipes. They were asked to complete four trials with the four types of prompts: verbal, light, image, and smart glass. Each trial had one assigned type of prompts and one recipe which included four different items located in four different places. The sequence of the trials was counterbalanced. The completion time for retrieving each item was recorded by the software system.
Immediately following these four trials, participants were asked to complete a questionnaire on their preferences regarding the prompts and participate in a brief interview where they gave feedback on the prompting system.
In session#2, participants went through a series of neuropsychology assessment (BDEA Complex Ideation subtest, Greek Cross Drawing, Go No-Go Test, Logical Memory Subtest from Wechsler Memory Scale IV, COWAT – Controlled Fluency Digit Span, Cancellation subtests of the Wechsler Adult Intelligence Scale – IV, Trail Making Test A & B, Stroop Color-Word test, and Grooved Pegboard Test) to evaluate their cognitive level respect to memory, executive function, attention, etc.
Results
Kitchen experience
The participants’ answers for kitchen experience on the questionnaire showed that the microwave oven is the most frequently used appliance in the kitchen, while remembering item locations and keeping track of recipe steps are the two most difficult activities for participants in doing kitchen tasks.
Domains |
Tests |
CI01 |
CI02 |
CI03 |
CI04 |
CI06 |
Memory |
Log Mem I |
-2.0 |
-1.0 |
-2.9 |
-0.7 |
-0.7 |
Log Mem II |
-2.0 |
-1.0 |
-2.9 |
-1.1 |
-1.0 |
|
Executive function |
Trails A |
-1.3 |
-2.4 |
-2.1 |
0.1 |
-0.5 |
Trails B |
-1.1 |
-2.4 |
-2.3 |
-1.3 |
-0.3 |
|
Stroop W |
-1.3 |
-3.0 |
-2.1 |
-1.7 |
-0.6 |
|
Stroop C |
-2.3 |
-3.0 |
-2.1 |
-0.9 |
0.3 |
|
Stroop CW |
-1.2 |
-2.3 |
-1.1 |
-0.3 |
-0.3 |
|
Language |
COWAT |
-1.6 |
-2.2 |
-1.4 |
0.8 |
0.7 |
BDAE |
1.0 |
1.0 |
-2.5 |
-0.4 |
-1.5 |
|
Sensory Motor |
GPeg DH |
-2.4 |
-3.4 |
-2.6 |
-1.2 |
-0.6 |
GPeg NDH |
-2.5 |
-4.5 |
- |
-1.3 |
-1.6 |
|
Spatial |
Crosses 1 |
-1.0 |
-0.6 |
0.7 |
0.8 |
0.4 |
Crosses 2 |
0 |
-0.6 |
0.7 |
0.8 |
0.4 |
|
Attention |
DigSpan |
-0.7 |
-1.3 |
-1.6 |
0.0 |
0.3 |
Cancellation |
-2.7 |
-2.0 |
-2.0 |
-0.6 |
-0.6 |
Neuropsychological tests
Each participant’s neuropsychological status was accessed through a series of standard neuropsychological tests. Table 1 shows the different neuropsychological statuses of the participants. Most of the participants performed within an impaired range on tests of memory, executive functions, and attention. Based on these results, the participants can be generally divided into two groups: group 1, including CI01, CI04, and CI06 who had mild to moderate impairments in executive functions; and group 2, including CI02 and CI03 who performed within a significantly impaired range of executive functions.
Preferences regarding the prompts
The participants’ preferences regarding to the four types of prompts can be seen in Table 2. For the overall preference ranking, participants were most satisfied with smart glass and image while verbal prompts were preferred least.
During the brief interview, all participants reported that multiple sensors and prompts implemented in their residential or group home would be easy to accept, as long as it would not compromise the general appearance of their home. In addition, all participants wanted to obtain portable prompting devices with touch screens. Some participants would like to have beeps before prompts to help with concentration.
Subject ID |
|
Verbal |
Light |
Image |
Smart Glass |
CI01 |
Preference |
1 |
4 |
2 |
3 |
C-Time |
16.83 |
18.21 |
13.25 |
17.08 |
|
CI02 |
Preference |
2 |
3 |
1 |
4 |
C-Time |
15.92 |
10.42 |
11.95 |
11.30 |
|
CI03 |
Preference |
4 |
3 |
2 |
1 |
C-Time |
17.90 |
18.99 |
16.56 |
- |
|
CI04 |
Preference |
4 |
2 |
3 |
1 |
C-Time |
16.88 |
12.40 |
10.31 |
10.35 |
|
CI06 |
Preference |
4 |
3 |
1 |
2 |
C-Time |
16.30 |
12.20 |
11.12 |
10.43 |
Effectiveness of the prompts
The average completion time to retrieve items using the different types of prompts for each participant is shown in Table 2. As it is shown, three participants took the least amount of time to retrieve items with image prompts and the other two participants used least amount of time with smart glass prompts. In contrast, all five participants took the most amount of time to retrieve items with verbal prompts or light prompts.
Discussion
The aim of this study is to evaluate different types of prompts in guiding multistep kitchen tasks for people with TBI, and to examine the end users’ preferences and acceptance of features of the current prompting system.
In the neuropsychological assessments, participants showed deficits in memory, executive functions and attention. Participant CI01 showed mild impairment to normal performance in memory and executive function and low level attention; CI02 had mildly impaired memory functions but significantly impaired executive functions and attention; CI03 had significant impairments across all of these three domains while CI04 and CI06 demonstrated generally normal to mild impairment of cognitive functions, compared with other participants.
Among the four types of prompts, image and smart glass were highly preferred by participants. In contrast, verbal prompts were least preferred by users. No clear correlations or patterns are found between participant preferences and the results of their neuropsychological assessments. It’s possible that the preferences are more related to participants’ personal habits and aesthetic factors. For example, although the participants were highly satisfied with the image prompts, they did not like the projectors as they were worried about how it would impact the appearance of the kitchen. Moreover, two participants rated smart glass prompts as their favorite because they were impressed by the neat design.
Participants took differing amounts of completion time in tasks with different types of prompts. Image prompts seemed the most efficient type to guide participants to complete the multistep tasks while verbal prompts seemed to be the least efficient. Another notable trend which can be observed from Table 2 is that participants in group 1 who had mild to moderate impairments in executive functions (CI01, CI04 and CI06), needed to use less amount of time to complete tasks with the prompts they preferred more. However, the trend in group 2, who had profound impairments is not clear, which may be related to the participants’ impaired self-aware abilities.
This study indicates some directions of the future ATC. For example, further research may need to pay more attention to how to help end users with their difficulties in locating and organizing kitchen items, and keeping track of recipe steps; also, aesthetic factors can have a key effect on the acceptance of the sensors and the effectiveness of the prompts. Therefore, further ATC development will need to keep the aesthetic design of sensors and prompts in mind, and offer users options to choose their favorite types of prompts. Concern over preserving the current aesthetics of their homes contributed to the fact that participants did not like projectors for image prompt. Portable devices with touch screens may be an alternative for the images. The ability to cooperate with caregivers will also be important, meaning different functions and interfaces for caregivers and end users will be necessary for the future prompting systems.
It’s our hope that this current study could produce some preliminary evidence on the effectiveness of different forms of prompts for task instructions, attracting more attention in the development of assistive technology for people with cognitive impairments.