RehabCounter: A Smartphone-based Assessment Tool for Rehabilitation Practitioners
Ishmat Zerin1, Casey O’ Brien1, Sheikh Iqbal Ahamed1, and Roger O. Smith2
1Marquette University, Milwaukee, WI 53233, 2University of Milwaukee- Wisconsin, Milwaukee, WI 53201-0413
ABSTRACT
As the rehabilitation industry continues to grow in size and maturity, technological innovation can facilitate evidenced-based practice. In this paper, we introduce the RehabCounter, a smartphone-based iOS application that allows rehabilitation practitioners to define, execute, and validate interventions using a single-subject design tailoring data collection to the specific needs of each patient. The RehabCounter allows users to gather data quickly and efficiently since it has an intuitive and robust data collection interface. Our proposed application highlights patient progress over time by comparing sessions tagged by intervention phases. To our knowledge, the RehabCounter is the first iPhone based standalone application that can reduce data collection burdens for the practitioner and allow them to obtain a more accurate, empirically driven picture of how well their rehabilitation programs work.
Keywords:
mHealth, Smartphone, Evidenced-based practice, Rehabilitation.
INTRODUCTION
Advances in smartphone technology place the ability to collect, analyze, and interpret data squarely at the fingertips of users. The influence of smartphones in today’s society is undeniable. In fact, smartphones are now the most popular mobile technology according to sales [9, 12]. With time, these devices have become more computationally powerful, broadening the domain of their potential applications. Providing faster and better accessible health service at lower prices is a major global challenge in the health care sector [2]. Another challenge involves the medical community’s continuing goal to meet patients’ expectations and satisfaction levels [1]. To address these challenges, mHealth works to make the treatment process easy, portable and flexible [10]. Remote patient interaction, advising, monitoring patient performance, recording doctors observations as well as patients' self-observations regarding their own health-related behavior now have the possibility of being facilitated by smartphones [15]. According to a PricewaterhouseCoopers report from the Economist Intelligence Unit (EIU), 68% of doctors in emerging markets have recommended mHealth [14].
Therapists and other practitioners work together with people receiving rehabilitation services to help generate the best intervention plans [6]. Rehabilitation relies upon precise clinical perception and decision-making [5]. There are a number of existing smartphone and web applications for rehabilitation. However, we could not find any current application that emphasizes precise data collection with immediate analysis of an individual patient’s performance over time.
This paper presents a novel, smartphone-based approach to help rehabilitation practitioners improve their evidence-based documentation. Initially we selected the iPhone as a popular platform that both achieves a high market penetration among practitioners and has a basic library for programming an accessible interface for people with disabilities. Throughout the paper, we explain the design, impact and reasons for making this application. The major contributions of RehabCounter are as follows:
- RehabCounter is an iPhone-based application for single subject design. This application can record quantitative data about a patient’s behavior and instantly create evidence-based graphs of progress.
- A new approach that works to simplify the job of rehabilitation practitioners in terms of analysis, time, and cost.
- The data collection model with timestamps and tagging of rehabilitation sessions with a particular phase allows practitioners to generate insightful graphs automatically that highlight patient performance over time and specifically defined intervention phases.
- RehabCounter is a generic and flexible system. There are no predefined task sets, and practitioners can collect any kind of count or frequency-based data.
Rehabilitation practitioners can define phases associated with a single or multiple sessions for each task set. It will help them to achieve individual patients’ goals, and consequently will guide practitioners to make quick, informed decisions based on collected data. That will eventually influence ability of a patient to take back control of their life and independence. To the best of our knowledge, this is the first smartphone-based rehabilitation application that can efficiently and precisely collect or store data as well as incorporate different types of progress graphs over time.
MOTIVATION
In the medical research field, disability and impairment have drawn attention in recent years. According to a survey of the World Health Organization (WHO) from 2007 – 2008, 7-10% of the world population has some degree of impairment or disability [16]. These numbers could increase as the world population increases. To achieve the maximum quality of life and highest level of independence, rehabilitation practitioners are helping these people through various rehabilitation programs. They are actively working with patients to rehabilitate them from chronic conditions or injuries, restore the optimal function of injured area, and prevent re-injury.
It is important to support rehabilitation practitioners with the highest possible technology throughout their treatment process. RehabCounter has the capability to meet the function of a general counter of any type of task with timestamps. Users can customize tasks to gather quantitative data about any kind of counting, exercise or personal training in the application.
RELATED WORK
Technology support for data collection and analysis of patient performance can enhance evidence-based documentation. Several applications are available for both smartphone and web interfaces that try to address this need.
iOrtho is an iOS-based rehabilitation application that contains features such as 85 orthopedic special tests, mobilization techniques with helpful descriptions and high quality large photos [7][8]. However, the downside of this application is its lack of data collection, storage and result assessments.
Fitness Builder PT is a tool for physical and occupational therapist practitioners that is executable on all kinds of iOS devices [4]. This software contains a number of exercise images and videos for rehabilitation programs and the freedom to add new exercises. This software is more likely used as a guideline or assistant to practitioners or patients on how to perform their exercises, but there is no option to examine their performance or evaluate their progress over time. On top of all this, Fitness Builder PT is costly and struggles with slow execution.
Droid-Glove is an Android-based gaming application for wrist rehabilitation [3]. It has features such as data collection from sensors and makes comparisons in real-time but the scope of this application is very limited since it targets only wrist rehabilitation. It does not appear that Droid-Glove has been implemented and brought to market.
PlanetRehab [13] and Mavenlive [11] are powerful applications in the rehabilitation area but address more the workflow requirements of running a private rehabilitation business. PlanetRehab includes automated scheduling for patients, bill generation, storing medical records and reports with some additional user-friendly features. Mavenlive is also good in automated assessments, exercise prescription, documentation and more. One of the main drawbacks of these applications is that they are web-based. Though these applications are executable on smartphone devices, the strength of the RehabCounter is that it is a standalone application and does not require an internet connection. It is an effective and useful application even in remote places or developing counties that have slow e-communication speed.
Through RehabCounter, our goal is to provide user-friendly customized data collection with automatic assessment facilities for single subject design experiments by using the capabilities of smartphone technology.
DESIGN AND IMPLEMENTATION
While designing the RehabCounter, our first concern was to develop a self-contained evidence-based application that will be highly customizable. This characteristic allows practitioners the maximum flexibility during their treatment program while at the same time guides them through instantly generated evidence-based graphs.
In order to perform the rehabilitation procedure efficiently and accurately, the RehabCounter allows practitioners to define any task for which they would like to count frequency with timestamps. Several phases and sessions can be conducted with a suitable timeframe during the treatment process. The number of phases and sessions depend on a patient’s condition and progress. RehabCounter provides customizable phase and session declarations before data collection with a timestamp.
Our application does not require an Internet connection to access content. No extra hardware is required. A sample task set is provided with tasks already populated so that practitioners can experiment with the application’s data collection and graph generation features immediately. Presently we use the CoreData framework for iPhone devices for storage and retrieval of the collected data. Practitioners can facilitate personal goal setting and assess the progress of each patient in this application though more accurate, empirically driven graphs.
Important features of the RehabCounter are:
- Data collection: The RehabCounter will collect data precisely and efficiently. It is an intuitive method that will record counts of events along with timestamps.
- Customizable: Every section of the RehabCounter is completely customizable. For example task sets, tasks, phases, sessions, reports, patient information, etc.
- Evidence-based: Phases, sessions, graphs, and events all assist in using actual data to make therapy decisions.
- Single Subject design: Creates formal single subject design data collection and comparisons of phases in the development of evidence-based practice.
The RehabCounter application starts with collecting the practitioner’s name and takes users to the main menu, which consists of three options. They are (1) Configuration/Setup, (2) Data Collection, and (3) Reports.
Configuration/ Setup
Practitioners enter information in the setup/configuration section to insert patients’ information and define Task Sets.
 Figure: 1(a) List of Task Set 1(b) User Interface for defining a Task Set
Figure: 1(a) List of Task Set 1(b) User Interface for defining a Task SetThis section contains another two options: Patient Lists and Task Sets. In Patient List, users will able to view existing patients, add a new patient, or edit existing information for patients. Practitioners can personalize, define, and customize Task Sets. For example “CN-NNM” could be the title of Task Sets. Associated with the “CN-NNM” Task Set, users can add any number of associated Tasks. For example, the tasks could be “Balance touches”, “Toe drags,” etc.
Data Collection
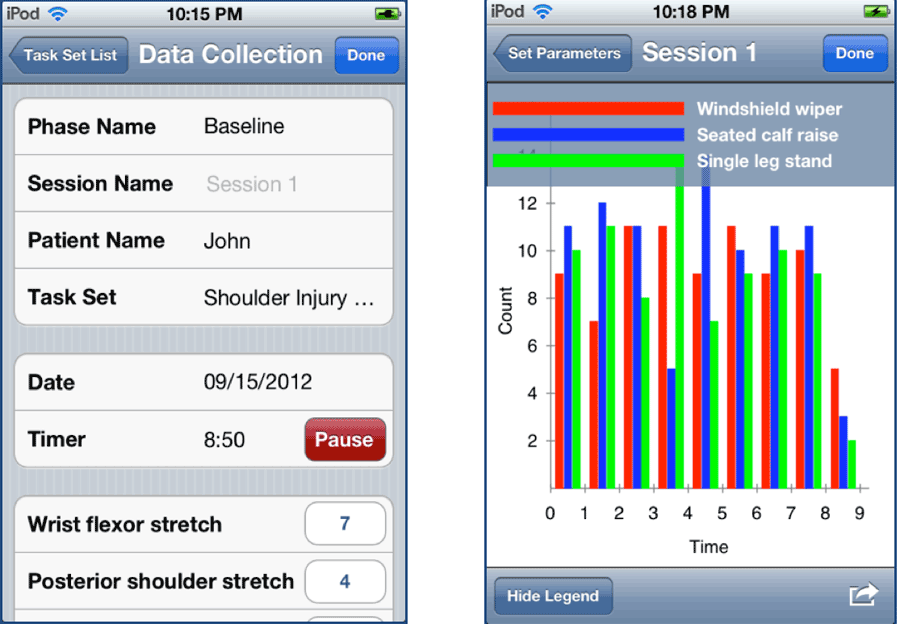 Figure: 2(a) User Interface for Data Collection; 2(b) Graph within a Session
Figure: 2(a) User Interface for Data Collection; 2(b) Graph within a Session Before collecting data, practitioners can define the phase and session for patients and task sets. This allows practitioners to collect data precisely for their assessment. Along with a selected patient and a predefined task set, they can count the number of times the patient successfully performs the selected tasks. A date and timer field keeps track of the date and the time duration needed to finish the tasks associated with that session. If needed, practitioners can customize or personalize sessions and phases [Figure 2(a)] according to each patient’s need. The results of the session can be saved and used later to generate graphs. This feature can reduce a practitioner’s data collection burden. Plotting these data in performance evaluating graphs immediately is entirely new idea. Practitioners can quickly monitor individual progress over time by viewing instant graph generation.
Reports
Report is one of the important features of the RehabCounter. Through this feature, practitioners can instantly view the performance of a patient over time, sessions, and phases based on collected data from the “Data Collection” period. Here practitioners can evaluate patients’ progress over time, session to session, and phases to phases. They can compare and select the best treatment plan for each individual patient. The goal of generating graphs automatically that would be useful to analize the single subject design experiments was crucial for implementation. In order to see the report of a particular patient with a task set, practitioners select the type of graph they desire. There are three available options for choosing the graph. They are (a) Graph within a session; (b) Graph across sessions; and (c) Graph across phases.
Graph within a session
This graph [figure 2(b)] allows practitioners to observe and analyze the performance of a patient on a selected Task Set within a single session. This graph will be generated based on the data timestamps to observe patient performance over time. The x-axis divides the total session time into one-minute intervals. A bar for each task within a Task Set represents the total counts for a given task over the interval. Practitioners can easily see if certain tasks are performed in clusters more towards the beginning, middle, or end of the session, for example. A legend, showing which colored bars represent which tasks, can be toggled on or off with a button at the bottom of the screen.
Graph Across Sessions
 Figure: 3(a) Graph across Sessions; 3(b) Graph across Phases
Figure: 3(a) Graph across Sessions; 3(b) Graph across PhasesPractitioners will analyze this graph [figure 3(a)] to compare the performance of a patient across multiple sessions. On the x-axis are the sessions that the patient has completed. On the y-axis are the overall counts for tasks that were performed during a session. Practitioners can track changes in task counts over sessions. This can be a helpful graph to identify how the patient is doing with the therapy. It also can allow the practitioner to visually inspect when a baseline has been achieved, thus indicating when to move to a new phase. By automatically generating this graph, the practitioner can create targeted treatment programs that are empirically driven and efficient. Again, a legend can be toggled at the bottom of the screen.
Graph Across Phases
This graph [figure 3(b)] contains phases, sessions, and event counts. To the best of our knowledge, RehabCounter is the first application that can show a patient’s performance precisely from phase to phase. With the quantitative data, practitioners can evaluate and compare which therapy or treatment plan works best for which patient. Practitioners can observe a patient’s performance across phases and can evaluate the improvement from phase to phase. On the x-axis are the sessions and on the y-axis are the associated counts for the selected tasks. The headings at the top of the graph indicate the titles of the phases. This graph represents the culmination of a rehabilitation therapy program. Through visual inspection, one can easily identify the extent to which therapy has been effective or not. If necessary, practitioners can add an arbitrary number of phases in the data collection section and view the completed and in-progress phases with this graph.
Practitioners can email these graphs for further analysis or share them with patients or other professions involved in patient care. Additionally, these graphs can be directly printed from iPhone devices. Consultation between practitioner and patient can help facilitate and personalize feedback and goal setting.
We believe these techniques will offer an effective health care management tool for both patients and practitioners.
CONCLUSION
Rehabilitation is a restoring process that helps injured or disabled people to get back their maximum level of independence. This paper gives an explanation of how our application, RehabCounter for iPhones, can make a positive impact in treatment procedure and help practitioners to gather data quickly and efficiently. Using RehabCounter, practitioners can accelerate the decision period by utilizing instantly generated performance graphs over time. While most existing rehabilitation software focuses on guiding patients in performing therapy exercises, our application emphasizes the collection and assessment of accurate therapy session data.
In the future, we are planning to use a remote server to make all services centralized and provide the maximum level of security that is expected in the medical field. We will send the collected data from the iPhone to a server for remote exercise performance analysis and consultation by the patient's personal practitioner. We are planning to integrate mobile phones and web services.
Our work offers a positive impact in the rehabilitation process as well as combines advance cellular technology with medical services. The main strengths of the model include effective data collection, analysis power, and reliance on existing smartphone technology, which allows potentially cost efficient implementation in various settings. We believe RehabCounter will make a remarkable influence on the utility of the developed care model in the rehabilitation area.
REFERENCES
- Benner, P., Ronda, G. H., Sutphen, M., Clinical Reasoning, Decision making, and Action: Thinking Critically and Clinically. Patient safety and quality, 2008 - 162.99.46.13
- Detmer, D. E. and Steen B. E., Information and Communications Technology and the Future Health Workforce: Transformative Opportunities and Critical Challenges, Copyright 2008, Published 2008.
- Deponti, D., Maggiorini, D., Palazzi, E. C., DroidGlove: An Android-Based Application for Wrist Rehabilitation. Ultra Modern Telecommunications & Workshops, 2009. ICUMT '09. International Conference on; 12-14 Oct. 2009.
- FitnessBuilder PT. 2012. https://www.fitnessbuilder.com/pt [Last accessed 26th September, 2012]
- Grimes, Facce, S.L., Gentech, The future of clinical engineering: the challenge of change Sarasota Springs, NY, USA. Engineering in Medicine and Biology Magazine, IEEE; March-April 2003.
- Hache, G., Lemaire, E.D., Baddour, N., Mobility change-of-state detection using a smartphone-based approach. Medical Measurements and Applications Proceedings (MeMeA), 2010 IEEE International Workshop on April 30 2010-May 1 2010; 43 – 46
- iOrtho+ Review. 2010. http://www.mhealth360.com/2010/08/07/iortho-review [Last accessed 26th September, 2012]
- iOrtho+ Mobile App for iPhone http://www.therapeuticarticulations.com/iPhone___iPad_App.html. [Last accessed 26th September, 2012]
- Kim R., By 2013, it will be a smartphone majority world. http://gigaom.com/mobile/by-2013-it-will-be-a-smartphone-majority-world [ Last accessed 26th September, 2012]
- Kyriacou, E.C., Pattichis, C.S., Pattichis, M.S., An overview of recent health care support systems for eEmergency and mHealth applications; Engineering in Medicine and Biology Society, 2009. EMBC 2009. Annual International Conference of the IEEE; 1246-1249
- Mavenlive. 2012. http://www.mavenlive.com. [Last accessed 27th September, 2012]
- Nishiguchi S., Yamada, M., Nagai, K., Mori, S., Kajiwara, Y., Sonoda, T., Yoshimura, K., Yoshitomi, H., Ito, H., Okamoto, K., Ito, T., Muto, S., Ishihara, T., and Aoyama, T. Reliability and Validity of Gait Analysis by Android-Based Smartphone. Telemedicine and e-Health. May 2012, Vol. 18, No. 4: 292-296
- PlanetRehab. 2012. www.planetrehab.com. [Last accessed 27th September, 2012]
- PriceWaterhouseCoopers. 2012. Current and future state of mHealth. http://www.pwc.com/gx/en/healthcare/mhealth/index.jhtml [Last accessed 27th September, 2012]
- Shimira, K., Mukasa, O., Schellenberg,A. J., Manzi, F., John, D., Mushi, A., Mrisho, M., Tanner, M., Mshinda, H., Schellenberg, D. The use of personal digital assistants for data entry at the point of collection in a large household survey in southern Tanzania. Emerging Themes in Epidemiology (2007), 4:5
- World Health Organization (WHO). mHealth: New Horizons for Health Through Mobile Technologies. Jan 2011. [Last accessed 27th September, 2012.