Michael S. Orendurff, PhD, David A. Boone, CP, PhD, Teri Chou, PhD
& Toshiki Kobayashi, PhD
Biomechanics Laboratory, Orthocare Innovations, Mountlake Terrace, WA., USA
Introduction
 Figure 1. Assessing "Potential to Ambulate" from real-world steps per minute data.
Figure 1. Assessing "Potential to Ambulate" from real-world steps per minute data.Determining the functional level of an amputee is useful for making prosthetic component decisions, for understanding the cost-benefit of specific components or interventions on the locomotion behavior of individuals, and for rationalizing component choices to payers. The MFCL K-level is the most common scale used to rate the functional level of individuals with limb loss.
Typically, gait observation and informal questions about activity level, or instruments like the Amputee Mobility Predictor (AMP)(Gailey et al., 2002) have been utilized to predict the functional status of amputees. Those predicted to be K3 level or above are provided the most costly components, such as microprocessor-controlled knees and carbon fiber feet. Rather than predict K level based on movement capacity in the clinic, a wearable sensor might provide additional information on locomotor behavior in the community to assess actual ambulatory mobility. For example, a typical adult might rate a K4 on the AMP, but only have K2 level activity during locomotor behavior in their typical environment. If an automated functional level calculation based on actual locomotor activity data could be validated by expert opinion, it might provide additional objective information on actual prosthetic component use, and complement visual observation of gait or capacity measures in the clinic.
Methods
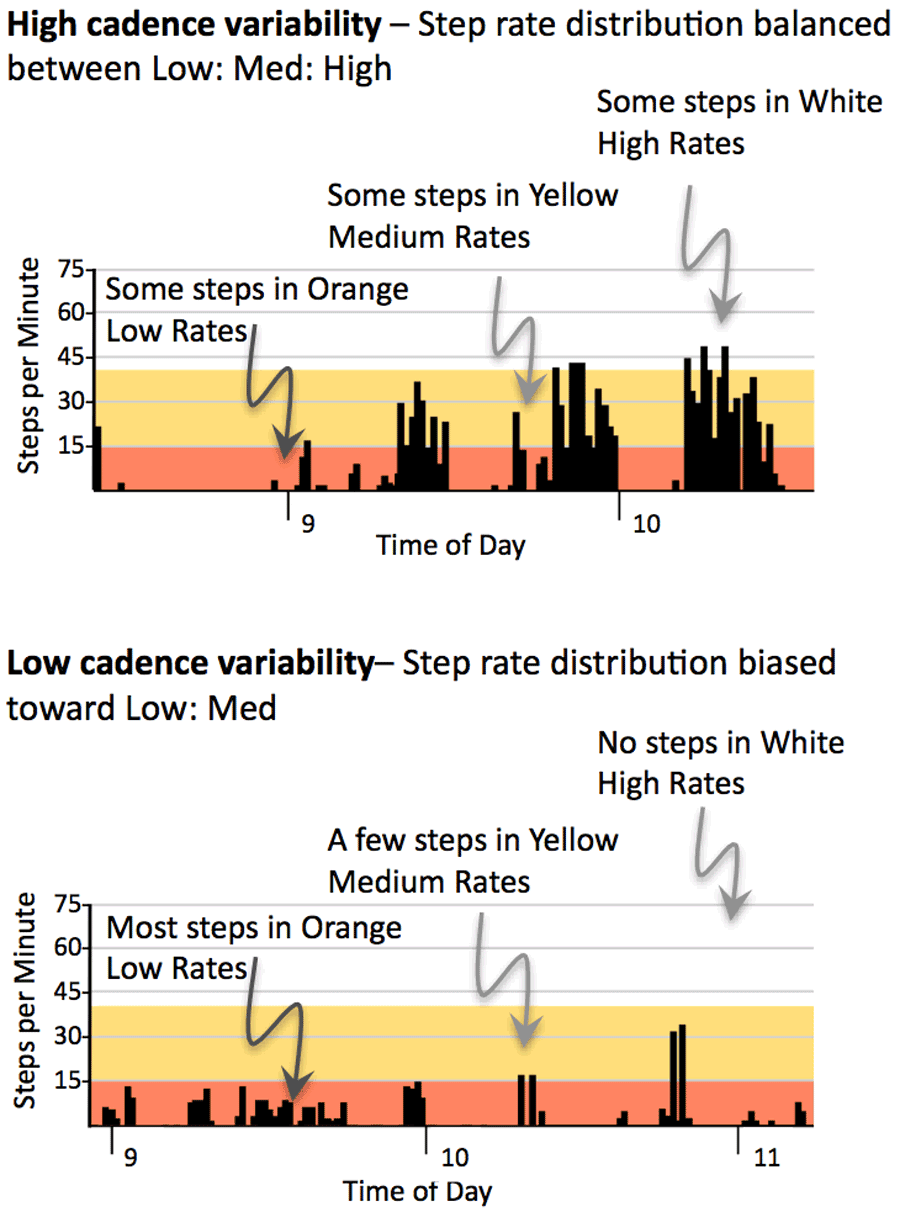 Figure 2. Evaluating Cadence Variability from real-world steps per minute data
Figure 2. Evaluating Cadence Variability from real-world steps per minute dataForty-eight experienced prosthetists were invited to participate in an anonymous online survey. Ethics committee review waived informed consent based on research methods that guaranteed anonymity for all participants. Prosthetists were chosen based on membership in the AAOP Gait Society, and on previous research or clinical expertise in prosthetic gait from published work. There were invited to participate twice, by email, one week apart. The participants who chose to take part in this study reviewed online images of the steps per minute data for 5-7 days of real-world activity (StepWatch Activity Monitor (Coleman et al., 1999)]) for eighty-one anonymous transtibial prosthesis users. Similar to the MCFL K level criteria, participants were asked to rate the amputee’s Potential to Ambulate, Cadence Variability, and Energy Level.
 Figure 3. Evaluating Energy Level from real-world steps per minute data.
Figure 3. Evaluating Energy Level from real-world steps per minute data.Potential to Ambulate was evaluated by estimating their most active one minute throughout the 5-7 days (see Figure 1); To assess Cadence Variability the ratio of Low:Med:High steps rates was estimated by the responding prosthetists (15<:16-40:>40 steps per minute; colored bands helped to define these ranges on the activity data images, see Figure 2).
To assess the Energy Level of the anonymous transtibial amputees the participating prosthetists estimated total daily step density (see Figure 3).
Based on these three activity characteristics the from 81 transtibial amputees, the study participants were asked to rate the functional level of each amputee on a 0-5 point scale and to include a decimal point estimate for increased resolution (for example 1.4 or 3.7). The participants never visually observed the amputees walking.
The amputees’ activity data was also used in a calculation to estimate their functional level based on Potential to Ambulate (best one minute of activity); Cadence Variability (Ratio of Low:Med:High step rates); and Energy Level (energy expenditure based on total daily steps(Foster et al., 2005)).
The calculated estimate was compared to the average of the participants’ functional level ratings using linear regression. It was hypothesized that the calculated estimate would account for greater than 60% of the variance of the participants’ rating. Significance was set to P < 0.05 a priori.
results
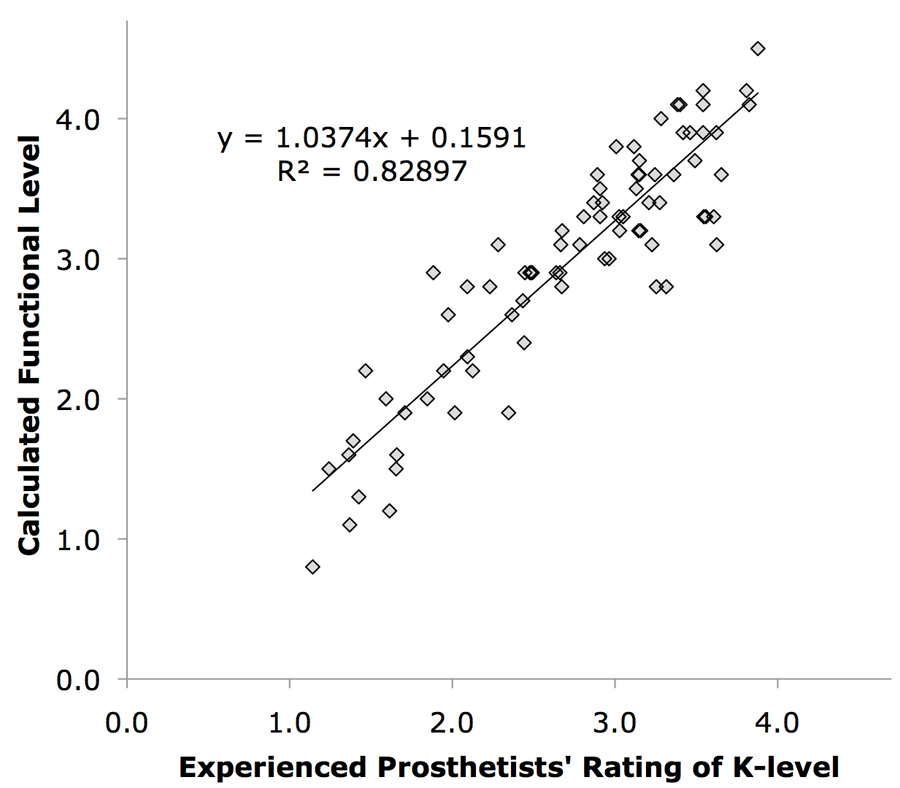 Figure 4. Experienced prosthetists rating of K level versus a calculated estimate based on real-world activity data. Although prosthetists were skeptical of their ability to rate K level solely from real-world activity data their mean K level values showed good agreement with the calculated estimate.
Figure 4. Experienced prosthetists rating of K level versus a calculated estimate based on real-world activity data. Although prosthetists were skeptical of their ability to rate K level solely from real-world activity data their mean K level values showed good agreement with the calculated estimate.
Fourteen prosthetists (29% response rate) completed the survey rating the functional level of the 81 anonymous amputees. Seven had >20 years of experience and 4 had >10 years of experience; Responding prosthetists treated 30 to >100 amputees each year. The calculated functional level showed good agreement with the average rating of the prosthetists (83% of the variance accounted for; P<0.001, Figure 4). The slope was close to one, showing good concordance within the two scales. The prosthetists did not receive any feedback on the accuracy of their ratings, and despite showing good agreement with the calculated estimate, the prosthetists expressed reservations at not being able to observe the individual amputees walk. Many felt gait observation added confidence and accuracy to their K level estimates.
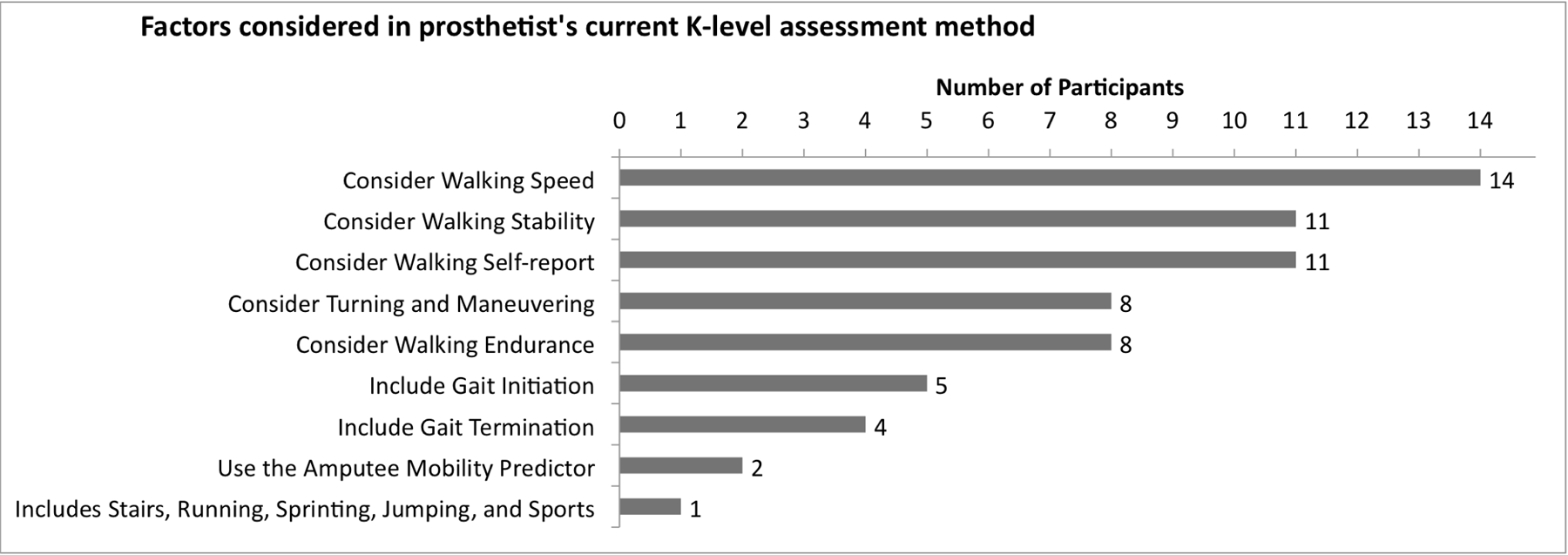 Figure 5. Prosthetists report that they evaluate a number of gait characteristics when determining K level.
Figure 5. Prosthetists report that they evaluate a number of gait characteristics when determining K level. The prosthetists also reported that they typically consider a variety of gait characteristics in order to estimate an individual’s K level. These were predominately focused on walking speed, maneuverability, stability, endurance, and amputee self-report.
discussion
The average K level rating of the fourteen experienced prosthetists who responded to this survey showed good agreement with the calculated functional level. The prosthetists may have been able to provide much greater accuracy if they were able view the amputee, and assess walking stability, speed, endurance, maneuverability and self-report. These factors may provide an additional and unique set of data that best evaluates an individual’s functional status.
The responses did cover a range of accuracy for each individual prosthetist, with some consistently lower or higher than the group average or the calculated estimate by nearly a full K level. For example, a specific prosthetists may have an accurate range of K levels based on the individual amputees they treat, but these levels may not match other prosthetists. This suggests that a combination of objective behavioral data (real-world activity level) and prosthetist assessment of walking characteristics might be the most accurate and most clinically feasible method to assess amputee functional level.
The real-world activity are distinctly different from clinic- or laboratory-based capacity measures, such as the AMP, that predict functional level based on an individual’s ability execute specific locomotor skills in a competent manner. Simply having the capacity to perform a specific set of ambulatory skills may not mean that the individual actually chooses to use those skills. An individual with no musculoskeletal pathologies may score K4 on the AMP, but may choose the activity pattern of K2 during community ambulation.
The Inspector General has leveled serious charges of questionable billing practices at the suppliers of prosthetic limbs(Levinson, 2011). Primarily this is base on data that show that prostheses provided for Medicare beneficiaries has decreased 2.5% from 76,000 in 2005 to 74,000 in 2009, while the cost for these prostheses has increased 27% from $517 million in 2005 to $655 million in 2009. This means more expensive components, primarily prosthetic feet, on low-level amputees who may be K1 or K2. It is not known if these more expensive components are facilitating increased activity levels in these Medicare beneficiaries, and no data is yet available on the consequences of this cost increase. It may be that these more expensive components are wasted on individuals who do not utilize them, or it may be that these more expensive components may increase activity, reduce inactivity-related co-morbidities, improve quality of life-years and ultimately reduce health care costs. It would be beneficial to acquire these data, and drive health care policy in an objective manner.
Some form of objective K level assessment for amputees may be required in the future, but since prosthetist are not compensated for this assessment, this task may move to physical therapists or perhaps rehabilitation physicians. Although these professionals may not have the conflict of interest that prosthetists may have, they are not likely to have any improved ability to predict actual prosthetic use based on clinic-based measures of ambulatory performance.
Additional work is needed on an objective K level determination method that uses both objective data on real-world activity patterns, and gait performance measures taken by health care professionals. This calculated functional estimate is a first step in creating a valid functional assessment process based on actual activity data during real-world ambulation.
References
Coleman KL, Smith DG, Boone DA, Joseph AW, del Aguila MA. (1999). Step activity monitor: long-term, continuous recording of ambulatory function. J Rehabil Res Dev, 36(1): 8-18.
Foster RC, Lanningham-Foster LM, Manohar C, McCrady SK, Nysse LJ, Kaufman KR, Padgett DJ, Levine JA. (2005). Precision and accuracy of an ankle-worn accelerometer-based pedometer in step counting and energy expenditure. Prev Med, 41(3-4): 778-783.
Gailey RS, Roach KE, Applegate EB, Cho B, Cunniffe B, Licht S, Maguire M, Nash MS. (2002). The amputee mobility predictor: an instrument to assess determinants of the lower-limb amputee's ability to ambulate. Arch Phys Med Rehabil, 83(5): 613-627.
Levinson D. (2011). Questionable billing by suppliers of lower limb prostheses. Washington, DC, O. o. t. I. G. Health and Human Services, OEI-02-10-00170