Laurie A. Malone1, Sangeetha Padalabalanarayanan2, Mohanraj Thirumalai2, Casey Herman1, Laudrey B. Cody3, Christopher Mills3, David Ryan4, & James H. Rimmer2
1Lakeshore Foundation, Birmingham, AL; 2School of Health Professions,
University of Alabama at Birmingham; 3Department of Physical Therapy,
University of Alabama at Birmingham; 4Department of Human Studies,
University of Alabama at Birmingham
ABSTRACT
Children with disabilities have lower levels of physical activity and fitness and higher levels of obesity compared to their nondisabled peers. Furthermore, youth with disabilities are often limited or excluded from physical activity where winning and competition is a central focus. The aim of this study is to examine active video gaming (AVG) as an option for promoting physical activity in youth with disabilities, by first identifying and addressing barriers that limit participation in those games. During the initial phase of this project, seventy-five youth with lower extremity mobility disability, 10-17 years of age, will participate in 3 lab sessions to play AVGs. Quality of game play and energy expenditure will be used to analyze the accessibility of these AVG systems, and help determine what barriers to successful gameplay exist. This research will adapt AVG technologies for youth with disabilities in an attempt to open a new engaging avenue for physical activity participation.
Introduction
Children with disabilities have lower levels of physical activity and fitness (Steele, Kalnins, Jutai, Stevens, Bortolussi, & Biggar, 1996; McDonald, 2002) and higher levels of obesity compared to their nondisabled peers (Rimmer, Yamaki, Davis, Wang, & Vogel, 2011; Rimmer, Rowland, & Yamaki, 2007). Among children with disabilities, engaging in physical activity can be extremely challenging (Murphy & Carbone, 2008). Sports fields, parks, playgrounds, and physical education classes are often used for competitive games and sports with winning as the primary outcome (Rimmer & Rowland, 2008). Unfortunately, children and youth with physical limitations in balance, strength, coordination, power, and aerobic fitness have a difficult time keeping up with their peers and the lack of success often diminishes their enthusiasm for physical activity. With fewer opportunities to participate in sports, recreation, and fitness, youth with disabilities are more likely to spend available leisure time in sedentary behaviors (Steele, Kalins, Rossen, Biggar, Bortolussi, & Jutai, 2004; Buffart, van den Berg-Emons, van Meeteren, Stam, & Roebroeck, 2009).
Active video games (AVGs) refers to a category of video games in which game play, progress, and scoring require substantially greater levels of physical activity than the typical pushbutton or joystick movements commonly associated with video game play. Active music video games using floor pad controllers (i.e., Dance Dance Revolution) have been popular for more than a decade, but the recent introduction of motion controlled AVGs (i.e., Nintendo Wii, Sony PlayStation Eye and Move, Xbox Kinect) that allow a much greater variety of physically active games has made AVGs popular with players of all ages. These games hold promise for promoting higher levels of energy expenditure, weight management and fitness among youth (Lanningham-Foster, Jensen, Foster, Redmond, Walker, Heinz, & Levine, 2006) and are recognized by The President’s Council on Fitness, Sports & Nutrition (PCFSN) as a tool to reduce childhood obesity (www.presidentschallenge.org)
Unfortunately, many current AVGs are inaccessible or offer limited play options for children who are unable to stand, have balance issues, poor motor control, or cannot use their lower body to perform game movements (Unnithan, Houser, & Fernhall, 2006). AVGs using floor pad game controllers (e.g., Dance Dance Revolution; Wii Outdoor Challenge) have obvious accessibility limitations. Motion controlled AVGs offer somewhat greater access, but accelerometer-based hand controllers such as those used by the PlayStation Move and Nintendo Wii platforms often require rapid and precise movements for successful play. AVGs using the camera-based controller of Microsoft Kinect typically require the player to be standing for proper game function. Making AVGs accessible to people with disabilities offers an innovative approach to overcoming a number of barriers to participation in beneficial physical activity. Making AVGs accessible is a necessary first step toward finding alternative ways by which youth with disabilities can increase their daily energy expenditure.
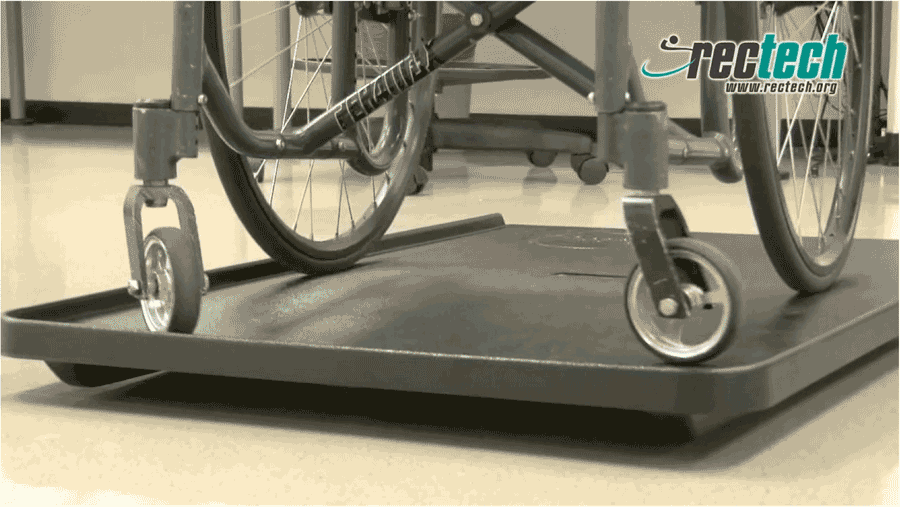 Figure 1. A large platform which sits on top of the Wii Balance Board as an example of an adaptation to allow wheelchair users to play games which require use of the balance board.
Figure 1. A large platform which sits on top of the Wii Balance Board as an example of an adaptation to allow wheelchair users to play games which require use of the balance board.Rehabilitation engineers and assistive technology specialists have developed a variety of creative and successful adaptations to game controllers and interfaces that allow people with disabilities to play video games (see Figure 1).
However, successful adaptation of game controllers to allow people with disabilities to play AVGs requires not only adaptation to allow satisfactory game play but also adaption to assure that the player with a disability experiences a similar level of energy expenditure. The results of a recent study with three non-ambulatory young adults with disabilities found clinically significant increases in energy expenditure could be achieved with AVGs (Rowland & Rimmer, 2012).
PURPOSE
The first step in this multi-phase project is to identify accessibility barriers encountered by youth with disabilities while using AVG controllers. The barriers found in this phase of the study will be used to develop adapted gaming controllers that enable children with disabilities to experience exercise benefits similar to those experienced by non-disabled youth.
METHOD
Participants
Seventy five participants will include boys and girls between the ages of 10-17 years. Potential participants must have been diagnosed with a lower extremity mobility disability (e.g, spina bifida, cerebral palsy, muscular dystrophy, spinal cord injury) with partial or full use of their upper extremities.
Procedures
The participants will come to the RecTech lab located at Lakeshore Foundation on 3 separate sessions to play AVGS on one of three systems (Nintendo Wii, Sony PlayStation, Microsoft Kinect). For each gaming session, the participant will be asked to play 4 different video games for a period of 8 minutes each, with a 5 min break between each game. The selected video games are rated E10+ (content suitable for ages 10 and older).
Over the course of the 3 sessions each participant will have played a total of twelve different video games. At the beginning of each session the participant will be outfitted with a Polar heart rate (HR) monitor to capture peak heart rate during game play.
After each game is played, the child's OMNI scale (Utter et al., 2002) will be used to collect the participant's rating of perceived exertion (RPE). Using the range of numbers 1–10 and child-like pictures, this scale quantifies how tired the participant was during the exercise testing. In addition, the participant will complete the Active Video Gaming Session Feedback sheet to document aspects pertaining to use of the system (e.g., did they experience pain, loss of balance) and sixteen Active Video Game Enjoyment questions. During each gaming session, the investigator will complete an Active Game Observation Sheet to document quality of game play and ability to use controllers. During game play the participants will be video recorded for performance and safety review.
Initial feedback
The first phase of this project will involve identifying the most common barriers for children with disabilities at functionally diverse levels in using controllers for active video game play at a satisfactory level. The RecTech research team has been finalizing the study protocols and running pilot tests with research staff and volunteers who have disabilities or work closely with children with disabilities.
The following are some of the comments we received from our test participants and assures us of the importance of this study for end users:
Volunteer A (manual wheelchair user) commented, “The concept of accessible video game platform is great. I need not just watch my friends playing games, instead participate if I can have adaptations that can be easily installed and transported”.
Volunteer B (manual wheelchair user) said, “If these non-inclusive games/consoles are frustrating me, I can imagine how this will demotivate a child with a disability. If these controllers can be adapted, we can reinforce that no matter what your disability is you can equally participate in playing active video games”.
Volunteer C (amputee uses crutches) told us, “The game pad in Wii console did not detect my movements because of my missing leg. It would be very important to make adaptations to broaden the audience”.
Volunteer D (multiple sclerosis, uses cane occasionally) said, “I have problems with balance so would like to see a more slip-resistant surface for mat games that would allow me to play more confidently”.
NEXT STEPS
Once barriers to successful play have been identified, the information will be fed to a team of engineers who will adapt current technology or develop new technologies to overcome these barriers. A primary strategy will be to develop technology which sits between the standard controller and the console, reading a specific remapped or adapted interface. While some adaptations may require only simple reengineering, others are likely to require complicated reverse engineering, which will be utilized as deemed feasible and/or necessary.
With adapted technologies in place, phase II will determine the dose-response relationship involved in playing AVGs in youth with a mobility disability with the resultant outcome of a listing of energy expenditure values in METs (metabolic equivalents) for each AVG. Currently, there are no guidelines for energy expenditure of various types of AVGs for youth with disabilities.
Games will be categorized into low, moderate, or vigorous intensity based on the participants’ heart rate during game play and measure of oxygen consumption reserve (VO2R = VO2 peak – VO2 resting) using a portable gas analyzer: light intensity = 20 to 39% VO2R; moderate intensity = 40 to 59% VO2R; and vigorous intensity = 60 to 84% VO2R (American College of Sports Medicine, 2010). The energy expenditure exercise protocol will include two sessions of 24 minutes of AVG play while connected to the portable analyzer for each gaming system.
Our long-term goal is to make AVGs accessible and develop an evidence base for the use of AVGs as an exercise modality for improving cardiorespiratory fitness and strength in youth with disability.
References
American College of Sports Medicine (2010). ACSM's Guidelines for Exercise Testing and Prescription (8th ed). Baltimore: Lippincott Williams & Wilkins.
Buffart, L., van den Berg-Emons, R.J.G., van Meeteren, J., Stam, H.J., Roebroeck, M.E. (2009). Lifestyle, participation, and health-related quality of life in adolescents and young adults with myelomeningocele. Developmental Medicine and Child Neurology. 51(11), 886-894.
Lanningham-Foster, L., Jensen, T.B., Foster, R.C., Redmond, A.B., Walker, B.A., Heinz, D., & Levine, J.A. (2006). Energy expenditure of sedentary screen time compared with active screen time for children. Pediatrics, 118(6), 1831-1835.
McDonald, C.M. (2002). Physical activity, health impairments, and disability in neuromuscular disease. American Journal of Physical Medicine and Rehabilitation, 81(11 Suppl), S108-120.
Murphy, N.A. & Carbone, P.S. (2008). Promoting the participation of children with disabilities in sports, recreation, and physical activities. Pediatrics, 121(5), 1057-1061.
Rimmer, J.H. & Rowland, J.L. (2008). Physical activity in youth with disabilities: A critical need in an underserved population. Developmental Neurorehabilitation, 11(2), 141-148.
Rimmer, J., Rowland, J.L., & Yamaki, Y. (2007). Obesity and obesity-related secondary conditions in adolescents with disabilities. Journal of Adolescent Health, 41, 224-229.
Rimmer, J., Yamaki, K., Davis, B., Wang, E., & Vogel, L.C. (2011). Obesity and overweight prevalence in adolescents with disabilities. Preventing Chronic Disease, 8, 1-6.
Rowland, J.L. & Rimmer, J.H. (2012). Feasibility of using active video gaming as a means for increasing energy expenditure in three nonambulatory young adults with disabilities. Physical Medicine and Rehabilitation, 4(8), 569-573.
Steele, C.A., Kalnins, I.V., Jutai, J.W., Stevens, S.E., Bortolussi, J.A., & Biggar, W.D. (1996). Lifestyle health behaviors of 11- to 16-year-old youth with physical disabilities. Health Education Research, 11(2), 173-186.
Steele, C.A., Kalins, I.V., Rossen, B.E., Biggar, D.W., Bortolussi, J.A., & Jutai, J.W. (2004). Age-related health risk behaviors of adolescents with physical disabilities. Sozial- und Präventivmedizin, 49, 132-141.
The President’s Challenge. Active Play PALA+ Challenge (2014). Retrieved January 12, 2014, from https://www.presidentschallenge.org/ActivePlayPALAChallenge/
Unnithan, V., Houser, W., & Fernhall, B. (2006). Evaluation of the energy cost of playing a dance simulation video game in overweight children and adolescents. International Journal of Sports Medicine, 27, 804-809.
Utter, A.C., Robertson, R.J., Nieman, D.C., & Kang, J. (2002). Children's OMNI Scale of Perceived Exertion: walking/running evaluation. Medicine and Science in Sports and Exercise, 34(1), 139-144.
Acknowledgements
This project is supported by RERC RecTech funded through grant H133E120005 from the National Institute on Disability and Rehabilitation Research.
Audio Version PDF Version