Katsutoshi Oe
Department of Mechanical Systems Engineering, Daiichi Institute of Technologyabstract
We aimed to develop some welfare devices for patients with phonation disorder. These devices include the artificial larynx, the compact pump unit for speech assist and the electric control type speaking valve, all of these are controlled by our control unit using neck myoelectric signal. The conventional speaking valves have one-way valve architecture, they open when the patient breathes in, and they close when patient breathes out or produces a sound. Therefore, the patients feel closeness in case of exhalation without phonation. In this report, we described about the proposal of myoelectric control-type speaking valve, and evaluated the performance. From the result, it was clarified that this valve system was better than conventional valves.
background
We developed the compact control unit using of neck myoelectric signal for controllable artificial larynx (Ooe & Tercero, 2010). In our previous research, it was clarified that this unit could control on/off and pitch frequency of the artificial larynx (Ooe & Kishimoto, 2013). In this step, we aimed to develop other welfare devices controlled by this unit, proposed two devices. One of them was a speech assist compact pump (Ooe, 2013) and the other was an electric control type speaking valve. In this report, we described about the speaking valve.
The speech cannula and tracheal opening retainer (TOR) were used as spacers to prevent tracheostoma closure. Patients who use these devices can not vocalize because exhalation can not vibrate the vocal cords. This valve is a one-way valve that is connected to a commercial speech cannula or a TOR. The valve closes during expiration; as a result, the air passes through the glottis, vibrates the vocal cords, and produces a laryngeal tone. However, This valve closes during the non-vocalization phase, causes resistance during inspiration, and can make the user feel uncomfortable. Therefore, the new type speaking valve was desired by the patients.
purpose
Characteristics of the ideal speech valve include
- Low resistance to airflow in the opening.
- Noninvation of parts in the case of device breakage.
- High-speed operation (reaction time of 300msec)
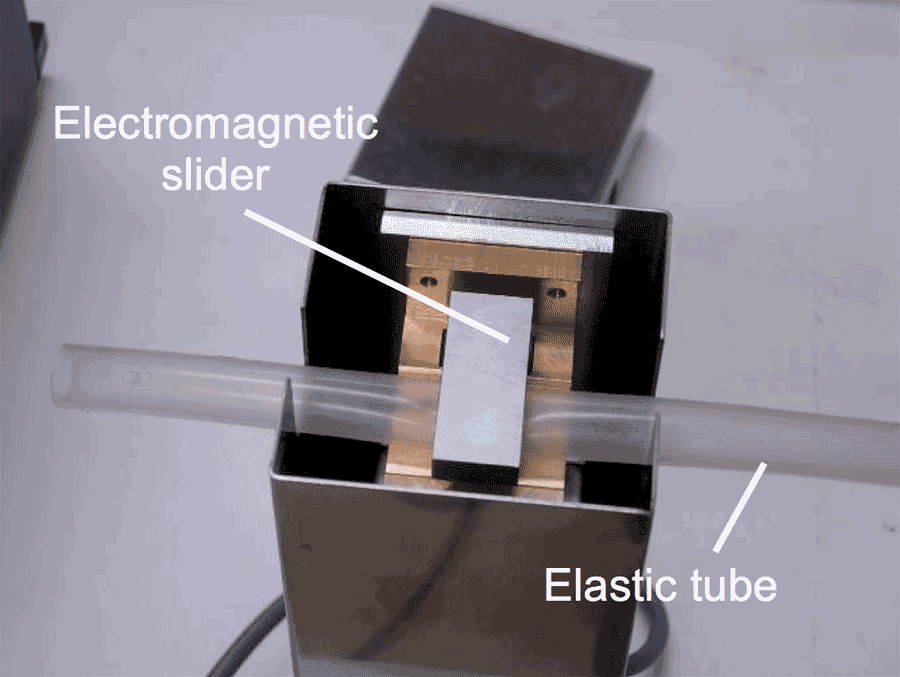 Figure 1: The electrical control-type speaking valve
Figure 1: The electrical control-type speaking valveAccordingly, we designed and prepared the prototype speaking valve shown in Figure 1. This valve has an electromagnetic slider and an elastic tube for its open/close mechanism, and the elastic tube is clamped by the electromagnetic slider when the valve is closed. The elastic tube is made of silicone rubber. Its inner diameter is 12 mm and its outer diameter is 13 mm.
This elastic tube is connected to the speech cannula that is attached to the tracheostoma. This mechanism does not have any structures inside the tube; thus, there is no danger of part invasion into the trachea upon device breakage, and resistance within the tube is low. The size of this valve system is 65 × 65 × 160 mm, making it easy to use at the bedside, but it is not suitable for wearing.
Method
We evaluated this speech valve prototype by assessing patients for smothering feelings during use. The evaluation test was carried out using the following workflow with continuous SpO2 and EtCO2 monitoring:
- To place the burden on the cardiopulmonary function, the test subject stepped up and down an 18-step staircase 5 times.
- To monitor the stability of breathing during phonation, after stepping the stairs, the subject sat down and read a 219-word English short story aloud.
- After that, the recovery time of EtCO2 to 40 mgHg was measured.
We chose the oxygen saturation of arterial blood (SpO2) and the end-tidal carbon dioxide concentration (EtCO2) asassessment criteria. These values are used as clinical markers of the smothering feeling and are suitable assessment criteria.
The measurement conditions of the control-type speech valve prototype are shown in Figure 2. The subject of this experiment was a 40-year-old man who had a closable tracheostoma by his mind. He had stenosis of the glottis and felt that breath constrictions would cause tracheostoma closure.
results &discussion
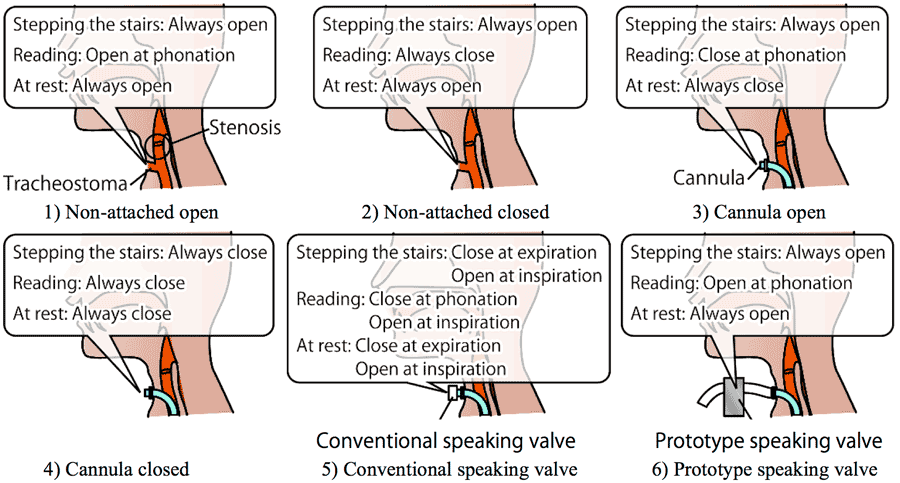 Figure 3: Measurement conditions of prototype speaking valve
Figure 3: Measurement conditions of prototype speaking valve Results of evaluation of the speech valve system prototype are shown in Table 1. Compared with condition 1 (the least resistant condition), the minimum SpO2 values were lower in other conditions and the maximum EtCO2 values were higher in conditions 2, 4, and 5. These findings confirmed the degradation of ventilation efficiency.
|
|
Min SpO2 (%) |
Max EtCO2 (mmHg) |
Recovery time (sec) |
1) |
96 |
53 |
92 |
2) |
86 |
60 |
168 |
3) |
94 |
53 |
118 |
4) |
86 |
58 |
172 |
5) |
89 |
58 |
162 |
6) |
94 |
53 |
128 |
This comparison revealed that the maximum EtCO2 was lower, the minimum SpO2 was higher, and the recovery time was shorter with the prototype valve than with the existing valve.
The prototype speech valve had the same maximum EtCO2 value as that of condition 6. The recovery time of the prototype valve was shorter than those of conditions 2, 4, and 5. The prototype valve had low flow resistance. Additionally, since the user can control the opening and closing of this valve, misvocalization by closure insufficiency was not a problem.
From the aforementioned results, it was confirmed that this prototype speech valve system with compact control unit had a better performance than the existing speaking valve.
conclusion
The prototype electrical control-type speaking valve was prepared as a new piece of equipment that operates at the time of vocalization. This speaking valve used a compact control unit, and it was confirmed that its performance was better than that of the existing speech valve. This prototype speech valve was too big for portable use but was suitable for bedside use. Upon miniaturization, the dream of a wearable high-performance speech valve system will be realized.
References
Ooe K., Tercero C. & Fukuda T. (2010). Development of the artificial larynx with neck EMG signal control. 2010 International Symposium on Micro-NanoMechatronics and Human Science, 127-132.
Ooe K., Kishimoto R. & Hashimoto Y. (2013). Myoelectric control method for controllable electrolarynx. Proceeding of IEEE SENSORS 2013, 1262-1265.
Ooe K., Nishihateruma T. and Yamamoto T. (2013). A speech assistance compact pump system with piezo micro pump units. Proceedings of ICFPAM,.
Acknowledgements
A part of this research was performed within JSPS KAKENHI grant number 23500648, Adaptable and JST Seamless Technology Transfer Program through Target-driven R&D grant number AS232Z02397.
Audio Version PDF Version