The RightFit Prosthetics Initiative: Affordable Prosthetic Devices for the Developing World (Johns Hopkins University)
Nicholas Flower, Rochelle Dumm, Ian Graham, Jason Lansdown, Ada Sierraalta
ABSTRACT

Globally, there are over 30 million people with an amputation (1), and 47% of this population has a lower limb difference (2). In many developing countries, trauma is the primary cause (3). Unfortunately, 80% of people who need of a prosthetic device cannot obtain one (4). Patients often cannot afford transportation to a prosthetic clinic, the prosthesis, or its long-term maintenance. To meet these needs, we have developed the RightFit prosthesis: an adjustable, modular, thermoforming device that can be reshaped to fit an individual’s changing limb, improving function and comfort. Our design addresses three obstacles to prosthetic care in the developing world: cost, time, and location. Compared to current solutions, RightFit is less expensive and faster to fabricate, and it does not need specialized equipment. Our device is adaptable and efficient, with a wide potential sphere of influence in the developing world and beyond.
http://www.youtube.com/watch?v=8LiER8uUFNcINTRODUCTION
In the developed world, the majority of amputations are caused by vascular disease and diabetes. In the world’s developing countries, trauma is primary cause of amputation. In regions such as Cambodia, Guatemala, and India, hundreds of thousands of people lose their limbs because of trauma and lack of access to proper, timely medical care.
Due to the unaffordable nature of prostheses and the difficulty associated with obtaining them, most individuals use crutches or wheelchairs to get around. Crutches are uncomfortable and ineffective as full time transportation, and wheelchairs are expensive. The benefits of a prosthesis over crutches or a wheelchair include greater mobility, better ergonomics and comfort. The added mobility provides the opportunity for individuals to become productive members of society.
A prosthetic leg contains three basic components: the socket (the interface between the limb and the rest of the prosthesis), the pylon, and an artificial foot. The most important part is the socket, which needs to be fit individually to each patient. If the socket is not fitted properly, it is uncomfortable and causes sores and inflammation at the points of contact. Over time, residual limbs change in shape and volume due to swelling and atrophy, which is usually a natural processes like healing or a child’s growth. It is expected that one person could need 15 to 20 devices in his or her lifetime (5).
To fit a patient with a prosthesis, a trained prosthetist must create a mold of the patient’s residual limb and make the socket from the cast. The patient often waits weeks between the first visit and the final fitting. The entire fitting process as it stands today is expensive, lengthy, and requires a significant amount of skill.
While this prosthetic technology is appropriate for people with amputations in developed countries, the cost of prosthetic care is insurmountable for patients where the need is greatest: the developing world.
NEED STATEMENT
There is a need for an affordable prosthetic device that is quick and easy to fit, does not require specialized equipment or a prosthetic clinic, and can be efficiently readjusted as the patient’s limb changes in shape and volume over time.
MISSION
The RightFit Prosthetics Initiative strives to design appropriate prosthetic devices that fit patients’ lives, improving access by reducing the time and cost required to make a device, so that these individuals can go where they want and participate in the activities that they want to participate in. Our device will bring us one step closer to making this a reality.
DESIGN AND DEVELOPMENT
 The RightFit Prosthesis
The RightFit ProsthesisWe have developed the RightFit prosthesis, a low-cost, modular, and easily adjustable prosthetic device. The prosthesis consists of three components – the foot, the pylon, and a thermoplastic socket – which can be molded directly over the patient’s limb. Its unique design and assembly utilizes locally available materials, making it ideal for use in regional hospitals in low resource settings. The RightFit prosthesis does not require specialized tools; it can be fit by an ISPO Category II ortopedic technician at a local clinic, which substantially decreases the distance a patient must travel to obtain prosthetic care.
Furthermore, our device allows patients to get back on their feet in one day rather than one to two weeks after the first molding, the time usually required to fit a patient with a prosthetic device. Because of the quick fitting time, adjustability, and modularity, our device significantly reduces fabrication and maintenance costs, thus increasing the affordability of prosthetic care and the efficiency of an individual practitioner.
The thermoplastic material we have selected can be molded in warm water, so that the socket can be formed directly over the patient’s limb (over a sock), as opposed to fitting over a plaster mold, the commonly used technique. The thermoplastic is sufficiently strong to withstand the large compressive loads exerted during gait. The material is biocompatible and has been used in other commercially available medical products.
Interfaces between Components
The socket-pylon adapter, an off-the-shelf reducer bushing for PVC piping, distributes the compressive loads that are applied to the device. This generic component can be easily produced in developing countries at local plastics manufacturing companies or purchased at hardware depots. The pylon-foot (ankle) adapter is comprised of a reducer bushing and a PVC cap with a bolt to secure the prosthetic foot to the assembly. These two adapters provide rotational and translational adjustability so that the technician can properly align the prosthesis.
The Fitting Process
The fitting process makes the RightFit prosthesis truly unique and revolutionary.
Step 1 |
The technician prepares the limb with a socks and reliefs. |
Step 2 |
The thermoplastic is rolled into a sheet of uniform thickness and drape-molded over the patient’s limb. |
Step 3 |
Global compression is applied over the thermoplastic to create an intimately fitting socket. |
Step 4 |
Once the socket begins to harden (approximately five minutes), the compression is removed. |
Step 5 |
When the thermoplastic turns completely opaque, the socket can be removed from the patient’s limb. |
 This figure depicts our fabrication method. A – Drape-molding thermoplastic, B – Trimming excess material (can be re-used), C – Applying global compression, D – Applying localized compression, E – Adjusting alignment of proximal socket-pylon adapter, F – Adjusting overall alignment.
This figure depicts our fabrication method. A – Drape-molding thermoplastic, B – Trimming excess material (can be re-used), C – Applying global compression, D – Applying localized compression, E – Adjusting alignment of proximal socket-pylon adapter, F – Adjusting overall alignment. To train the technician, RightFit has created a manual for education and reference for proper fitting technique. RightFit will also provide a video tutorial for guidance, if the appropriate technology is available.
Alignment
Using bench alignment, the technician will attach the socket-pylon adapter and make angular, rotational, and translational adjustments according to standard prosthetic manuals. After assembly of the prosthesis, the alignment can be further adjusted by locally heating the thermoplastic at the upper adapter with a heat gun, hair dryer, or hot water.
EVALUATION
Our final prototype has been evaluated by usability and humidity test, and consumer needs assessments. We have been working with Dankmeyer Incorporated, a local prosthetic clinic in Maryland, and have adjusted our design to fit the needs of patients and practitioners. Protocols for mechanical testing (according to ISO standards) are complete. 4 point bend testing and structural testing are under way. Preliminary material analysis demonstrated that the material retains its mechanical properties after adjustment and finite element modeling simulations help confirm the durability of our device. Additionally, a patient pilot study, to be performed at the Kennedy Krieger Institute (a subsidiary of the Johns Hopkins Medical Institutions), has been approved by the Institutional Review Board at the Johns Hopkins School of Medicine. This test series will examine fit and comfort and compare our prosthesis to currently available devices.
In January, RightFit traveled to Guatemala with a prosthetist from Dankmeyer to meet with practitioners, patients, and other stakeholders to ask for feedback and explore the need for prosthetic devices. Our findings confirmed our need statement, and therapists at rehabilitation clinics would like our device so that they can send patients home with a prosthetic limb rather crutches. Our material can also be used to repair existing sockets. A patient came into a prosthetic clinic with a broken device, and thanks to RightFit, he left the clinic an hour later with a repaired prosthesis.
DISCUSSION AND CONCLUSION
Overall, our device meets all of our project goals. It serves the needs we have identified and has shown potential in other areas as well. To concisely reiterate, our prosthesis:
- - can be easily and quickly molded directly over the patient’s limb
- - can be readjusted
- - has modular components
- - does not require extensive training
- - does not require a full set of tools
- - uses mostly off-the-shelf parts
 Design Iterations
Design IterationsDuring the design process, the interfacial adapters to both ends of the pylon were the most difficult to develop. We wanted to optimize the strength of the device under compression and shear, but also minimize cost and maintain rotational or translational adjustability, which are both crucial when aligning the device prior to sending the patient home.
 Final Prototype
Final PrototypeCreating an ankle adapter and maintaining rotational adjustment were challenging. Initially, we considered a simple through bolt but decided against it because it was too primitive and did not allow for any adjustment. We also contemplated using a concave/convex mating system, but without a bolt to compress them together it would not work. Ultimately, we modified the second solution using existing PVC fittings and some machining and were able to meet our goals.
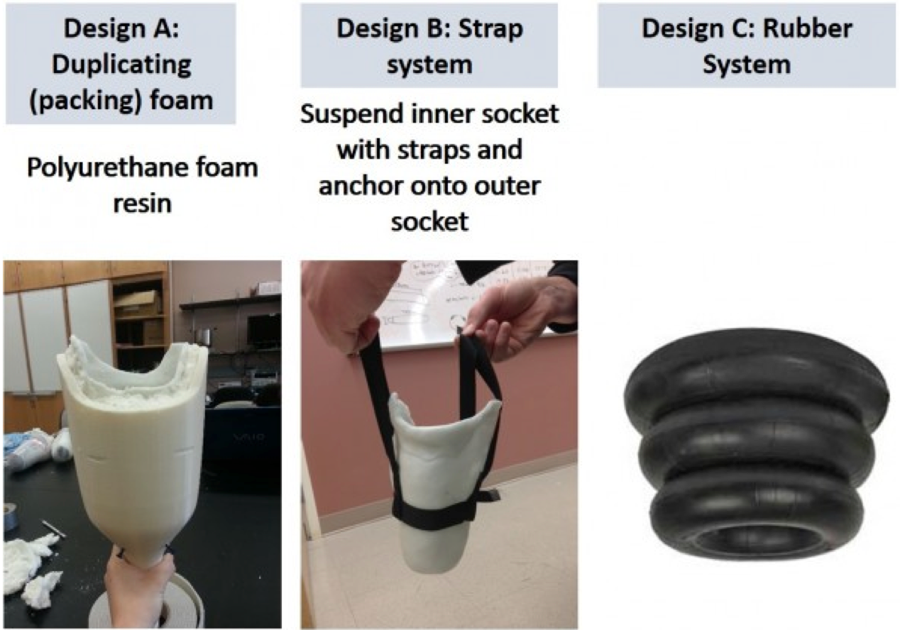
 Preliminary Prototype
Preliminary PrototypeWe also began by using a large outer shell for the socket that would be made of polypropylene for strength and durability purposes. The inner socket, as we called it, would then be hung by a series of four straps secured on the outside of the outer shell or suspended within using o-rings made of rubberized material. This made the interfacial adapters even more of an issue, raised the cost substantially, and was eventually deemed unnecessary after our first round of materials testing, when we found that our material is strong enough for our purposes, even under humid conditions.
Recently, we contemplated switching from PVC to aluminum, aware of the concomitant increase in cost. Standard prosthetic pylons and adapters (aluminum) collectively cost $75 USD, whereas our current adapters only cost a few dollars at most, especially at wholesale prices. We have chosen to stick with PVC for our device because even the 1.5” diameter tubing can sufficiently withstand up to 10X body weight.
We spoke with the International Committee of the Red Cross (ICRC), and the feedback we received was extremely helpful. Rather discourage collaboration, they embraced our ideas and suggested integrating our components into their own products.
After nearly two years of front-end design research and development, we have been able to design a device that meets the needs of our patients and their caregivers. We have created an adjustable prosthetic device that will increase patient access to prosthetic care in the developing world for those who could not otherwise obtain a prosthesis.
REFERENCES
[1] Aleccia J. 2010. Limb loss a grim, growing global crisis. Retrieved May 7, 2010, from http://haitiamputees.msnbc.msn.com/_news/2010/03/19/4040341-limb-loss-a-grim-growing-global-crisis
[2] ”A Manual for the Rehabilitation of People with Limb Amputation,” World Health Organization, 2004, <http://www.posna.org/news/amputations.pdf>.
[3] Strait, Erin. “Prosthetics in Developing Countries.” Journal of Orthotics and Prosthetics (2006).
[4] Necmioglu, S., M. Subasi, C. Kayikci, and D.B. Young. Lower Limb Landmine Injuries. 2004. Prosthetics and Orthotics International. Vol. 28. p37-43. <http://informahealthcare.com/doi/abs/10.3109/03093640409167923> 10 October, 2012.
[5] Andrysek, Jan. “Lower-limb prosthetic technologies in the developing world: A review of literature from 1994–2010,” Prosthetics and Orthotics International. 34(4): 378-398. December 2010.
ACKNOWLEDGEMENTS
We would like to thank our clinical advisors: Mark S. Hopkins, PT, CPO, of Dankmeyer Inc., and Dr. Marlis Gonzalez-Fernandez, Department of Physical Medicine and Rehabilitation at the Johns Hopkins School of Medicine. We would also like to thank our engineering and management advisors from the Johns Hopkins University and Center for Bioengineering Innovation and Design: Dr. Stephen Belkoff, Dr. Youseph Yazdi, Dr. Pamela Sheff, Prof. Lawrence Aronhime, Kevin Keenahan, and Nick Flower. A special thank you to the President Ronald Daniels of the Johns Hopkins University for making our field analysis in Guatemala possible, and to our partners at the Transitions Foundation of Guatemala: John Bell, Alex Galvez, and Joel Chiti. Lastly, we would like to thank Infinite Biomedical Technologies for providing counsel and support: Dr. Rahul R. Kaliki, CEO, Dr. Ananth Natarajan, Dr. Nitish Thakor, and Michelle Zwernemann.
Contact: Rochelle Dumm, 3900 N. Charles St., #212, Baltimore, MD 21218, rdumm1@jhu.edu
Audio Version PDF Version