Steve Sutter, CEO1, Michael D. Justiss, PhD, OTR2
1CreatAbility Concepts Inc., 2Indiana University Department of Occupational Therapy, Indianapolis, IN.
INTRODUCTION
According to the U.S. Census, the rural elderly population was 8.4 million as of the year 2010. This number is expected to increase to 10.6 million by 2020, and 13.8 million by 2030 (U.S. Census Bureau, 1998). Rural seniors (people 65 years and over) represent a large portion of the nation’s home care recipients. Rural seniors are more likely than their urban counterparts to have complex medical issues requiring health care interventions, including a higher incidence of diabetes and heart disease (American College of Physicians, 1995). Research demonstrates rural seniors in the U.S. have worse health outcomes than their urban counterparts (Jones, C.A., Parker, T.S., & Ahern, A., 2009). Rural America presents a unique set of obstacles and conditions that make the delivery of healthcare and related support services, such as aging in place difficult. Strategies are required to bridge the ever-widening gap between their care needs and their capabilities. From an economic and societal perspective, a cost effective solution may be to support the preference of older adults in rural communities to age in place (Rural Healthy People 2010).
PURPOSE
The purpose of this pilot study was to determine the feasibility and usability of the Rural-Health-Mate (RHM) system for helping rural seniors to more independently perform healthcare and safety-related tasks compared to their current methods.
METHODS
The feasibility study of the RHM system was conducted exploring the abilities of 26 rural seniors (75 to 93 years old). The abilities reviewed were: independently taking medications, measuring vital signs, detection of unsafe conditions in the home and alerting someone if they fell. This study compared the RHM system with their current methods of using digital or written lists, notes on pre-printed calendars, and lanyard-style personal emergency response systems (PERS).
The basic hypothesis was that rural seniors would be able to perform these health and safety-related tasks with less assistance and with fewer errors when using the RHM system prototype as compared to their current method. The Rural-Health-Mate (RHM) system was designed and developed for use in the pilot study evaluation. This first release of the software and hardware components concentrated on supporting the essential features and capabilities that determined the technical feasibility, as well as the usability with study participants.
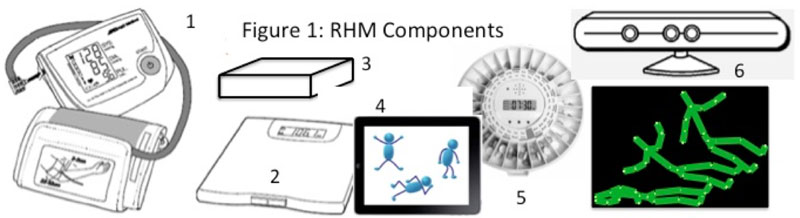
The physical components of the prototypes are RHM (Figure 1 (left to right)): 1) Bluetooth blood pressure cuff used to measure the senior’s blood pressure, 2) Bluetooth scale to measure weight, 3) Control Center that communicates with the Bluetooth devices and the medication tray via Z-wave, 4) Tablet Console, 5) COTS disc-style medication tray with a rotating slot includes an integrated wireless sensor to detect when medication was dispensed, and 6) Kinect sensor (with the three eyes) used to predict and detect falls and with behaviors projected/recorded as stick figures.
Inclusion criteria: Seniors enrolled in one of three different community centers in rural Colorado; > 45 minutes to nearest healthcare provider, 75+ years old, lives independently, currently under the care of a healthcare professional or have been released from the hospital in the past 12 months. All participants lived in a rural setting for most of their lives (>30 years). Subjects were each paid a stipend for participation in the study.
19 women, 7 men |
Age range: 75 to 93 |
3 used portable oxygen |
||
7 had mobility impairments |
19 had hearing impairments |
18 had type II diabetes |
||
4 profound vision loss (diabetic retinopathy) |
8 reported recent falls |
|||
Average distance to care provider was 55 miles |
8 owned and operated a car (5 W, 3 M) |
|||
7 had been discharged from a hospital in the past 12 months (14 medication non-adherence-related, 3 orthopedic surgery, 4 heart-related). |
5 reported reduced strength (reporting that a half-gallon of milk was heavy) |
|||
13 (all women) saw a Dr. every quarter |
||||
The field evaluation took place over a four-week period. There were two dependent measures: 1) accuracy as measured by the number of errors made during the experimental session; and 2) independence as measured by the number of prompts required to complete the session. The vital sign devices and the medication trays were the same. Each participant took their blood pressure, weighed themselves, took (pretend) medications (swallowing not required), abruptly stood from a sitting position, answered survey questions, and tried to detect safety-related issues (such as a space heater being left on unattended when they were leaving).
Data collection forms were used to record errors and prompts during each experimental session. The performance of each subject was closely monitored, with verbal prompts from the instructor and assistance provided when requested or as soon as mistakes were made. In this way, individuals always achieved success at the task, even if they needed assistance to achieve it. In addition to the quantitative data collected, there was room provided on the data collection forms to record additional observations as well as statements made by subjects during the test sessions. These observations identified areas for more rigorous assessment during Phase II.
Data Analysis
The data was analyzed using SPSS [24], software package for behavioral statistics. A multivariate analysis of variance procedure was used to compare mean differences between the two experimental conditions (RHM vs. their current method) for each dependent measure Average Errors and Average Prompts (Table 2).
RESULTS
|
Mean |
SD |
Range |
|
Average Errors |
RHM |
1.07 |
1.19 |
0-3 |
|
Typical Method |
4.92 |
3.17 |
0-14 |
Average Prompts |
RHM |
1.67 |
1.56 |
0-4 |
(from instructor) |
Typical Method |
6.51 |
4.02 |
1-16 |
The first dependent measure was accuracy, as measured by recording Average Errors (p<.001), which was a measure of subjects’ ability to correctly operate the equipment using both methods. When using RHM (X = 1.07, SD= 1.19) subjects made significantly fewer errors when compared to their normal method (p<.001). The second dependent variable, independence, as measured by Average Prompts (p<.001) provided to subjects while performing the healthcare and safety-related tasks during the experimental sessions. Subjects required significantly fewer prompts when using RHM (X = 1.67, SD= 1.56) to complete the tasks as compared to when using their typical method (p>.001).
After the testing was completed, each participant was again asked to rate their experience with RHM (Table 3).
1 = strongly disagree 5 = strongly agree |
Typical method |
Using RHM |
Mean |
Mean |
|
Sense of Independence |
2.4 |
4.7 |
Ease of use |
2.2 |
4.2 |
Physical / mental effort |
1.8 |
3.9 |
Satisfaction with approach |
1.7 |
4.4 |
Sense of safety |
1.6 |
4.6 |
The RHM system was also tested with 27 professional and volunteer caregivers and providers. Inclusion criteria: previously or currently a volunteer or professional caregiver for a senior that required them to travel more than 30 minutes to the rural senior’s home. Caregiver population: 27 (19 women, 8 men), association with senior: 8 volunteer, 7 family members, 12 professional. These 27 caregivers first completed a survey focused on key areas identified in the focus groups. This exercise was repeated after having used RHM’s caregiver interface called Care Plan. Caregivers performed the following tasks: viewed the dashboard and navigated the HIPPA-compliant Care Plan screens, verified the senior’s vital signs, adjusted the senior’s schedule, viewed their fall risk assessment, and explore the electronic whiteboard to verify stakeholder coordination and the status of the care-giving activities.
1 = strongly disagree 5 = strongly agree |
Without RHM |
With RHM |
|
Mean |
Mean |
Immediate awareness of a problem |
2.1 |
4.7 |
Information available in one location |
1.7 |
4.4 |
Remote verification vitals / meds |
1.4 |
4.7 |
Can adjust and verify schedule |
2.1 |
3.9 |
Monitor fall risk assessment |
1.7 |
4.4 |
Intuitive stakeholder coordination |
2.2 |
4.2 |
DISCUSSION
The results of this Phase I pilot project demonstrated the technical merit and feasibility of the RHM system for helping rural seniors to more independently perform healthcare and safety-related tasks compared to their current methods. Results also demonstrated that the RHM offers rural seniors a cost-effective and non-intrusive option to preserve the independence that they value while maintaining their health and quality of life. The pilot study provided substantive empirical support for the idea that the RHM system can be used by rural seniors to take their medications, and measure their vital signs independently, as well as to be aware of safety-related situations in the home. The prototype of the RHM system was significantly more accessible than their current method used by all of the participants in the study. All but one subject thought that RHM’s capabilities were personally relevant to them. Next steps will involve a wider subject base for a longer period of time, to hopefully collect improvements in outcomes.
REFERENCES
Barley, G. E., Reeves, C. B., & O-Brien-Gonzales, A. (2001). Characteristics of and issues faced by rural female family physicians. Journal of Rural Health, 17(3), 251–258.
Davis, R., & Magilvy, J. K. (2000). Quiet pride: The experience of chronic illness by rural older adults. Journal of Nursing Scholarship, 32(4), 385-390.
Jones, C.A., Parker, T.S., & Ahern, A (2009). Taking the Pulse of Rural Health Care. Amber Waves: The Economics of Food, Framing, Natural Resources and Rural America. U.S. Department of Agriculture.
National Rural Health Association Facts and Figures Retrieved 8/10/12 From: http://www.ruralhealthweb.org/go/left/about-rural-health/
Rural Healthy People 2010—"Healthy People 2010: A Companion Document for Rural Areas," via a project funded with grant support from the federal Office of Rural Health Policy. Retrieved 8/12/12 from: http://www.srph.tamushsc.edu/rhp2010/
Rural primary care. (1995) American College of Physicians. Ann Intern Med. 122(5):380-90.
Smith, Matthew; Ahn, Sang Nam; Sharkey, Joseph; et al, (2012) Successful Falls Prevention Programming for Older Adults in Texas: Rural–Urban Variations. Journal of Applied Gerontology 31(1) 3–27.
U.S. Census Bureau. (1998). Aging in the United States: Past, Present, and Future. [online]. Retrieved March 2010 from: http://www.census.gov/ipc/prod/97agewc.pdf
ACKNOWLEDGEMENTS
We would like to thank the USDA for funding this project with the aim of improving life in rural America. We would also like to thank Greg McGrew and his team at Assistive Technology Partners, Denver, Colorado, for coordinating and assisting with many of the pilot study evaluations