Sharon Eve Sonenblum, Stephen H. Sprigle
Rehabilitation Engineering and Applied Research Laboratory, Georgia Institute of TechnologyIntroduction
Studies investigating risk factors for PrU development in SCI cohorts have not found pressure relief behavior or frequency to be associated with PrU occurrence (Garber, Rintala, Hart, & Fuhrer, 2000; Krause & Broderick, 2004; Raghavan, Raza, Ahmed, & Chamberlain, 2003). There are two possible explanations for this finding. First, each of the studies relied on self-report measures of pressure relief practices. Yet self-reported behavior is known to be highly unreliable. Second, protective weight shifting behaviors may include activities other than dedicated pressure reliefs. Indeed, many functional movements performed while seated in a wheelchair will also redistribute pressure off PrU risk sites (S. E. Sonenblum & Sprigle, 2011; S. E. Sonenblum, Vonk, Janssen, & Sprigle, 2014).
The purpose of this study was to describe how individuals with acute and chronic SCI move in their wheelchairs during everyday life, and to test if in-seat behavior differs between people with and without a history of recurrent PrUs.
Methods
| Chronic | Acute | |||
|---|---|---|---|---|
| # Subjects (% Subjects) | # Subjects (% Subjects) | |||
| Male | 23 (79%) | 22 (71%) | ||
| Female | 6 (21%) | 9 (29%) | ||
| Level of Injury (n=28): | ||||
| Cervical | 3 (11%) | 8 (26%) | ||
| Upper Thoracic (T1-T6) | 7 (25%) | 10 (32%) | ||
| Lower Thoracic - Lumbar (T7-L3) | 18 (64%) | 13 (42%) | ||
| Complete Injury (n=28) | 17 (61%) | 11 (35%) | ||
| Mean (SD) | Range | Mean (SD) | Range | |
| Age | 41 (12) | 21 – 66 | 32 (13) | 19-63 |
| Height (inches) | 70 (4) | 60 - 77 | 70 (4) | 62 – 78 |
| Weight (lbs.) | 175 (42) | 93 - 280 | 161 (32) | 112 - 240 |
| Time Since Injury | 15 (10) years | 2 – 33 years | 97 (42) days | 25 – 215 days |
For this study, all participants were adults with SCI who used a wheelchair as their primary mobility device and had the ability to independently perform weight shift maneuvers. 29 participants with chronic SCI, defined as more than 2 years post injury, were recruited, as well as another 31 participants with acute SCI who were recruited as soon as possible within their first 5 months following discharge from acute rehabilitation.
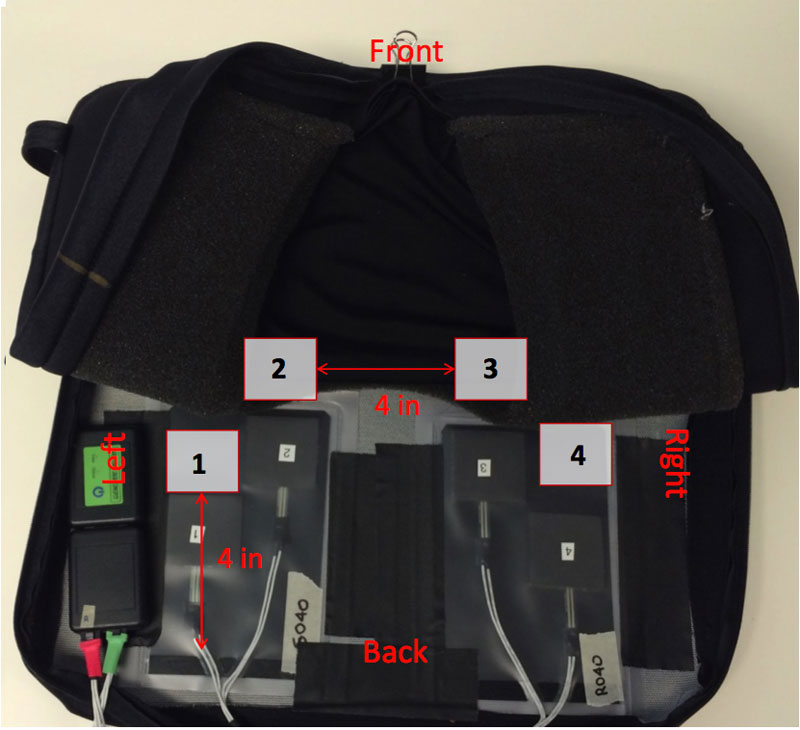
Participants were instrumented with a custom weight shift monitor (WSM) beneath their wheelchair cushion and a data logger to store the recorded forces (Figure 1). Forces beneath the wheelchair cushion were sampled at 1 Hz for a period of 1-2 weeks, at which point data was retrieved for post-processing with Matlab R2014a. A tri-axial accelerometer was attached to the wheel and used to calculate daily mobility characteristics (S. E. Sonenblum, Sprigle, Caspall, & Lopez, 2012).
The setup and analysis protocol for this study has been described elsewhere (Martin, Sonenblum, & Sprigle, 2014; S.E. Sonenblum, Sprigle, & Martin, In Press), but will be described here briefly. The instrumentation session commenced with a training protocol designed to relate the loads measured by the WSM to the actual loading condition at the buttocks/cushion interface as simultaneously measured by an FSA interface pressure mat. The protocol included a series of leans with upright sitting and depression lifts interspersed. Once complete, the interface pressure mat was removed and participants were sent home with the WSM, data logger, and accelerometer and instructed to go about their daily life as if the equipment was not present.
WSM data analysis to describe in-seat movement required defining three variables as follows:
- Weight Shift – either ischium is partially unloaded (> 30% pressure reduction) for > 15 seconds
- Pressure Relief – left and right ischium fully unloaded for > 15 seconds and < 2 minutes
- Out of Chair – fully unloaded for > 2 minutes
The daily time in spent in the wheelchair and the in-seat behavior characteristics, along with the number of bouts, distance wheeled and percent of time in chair spent moving (% mobile) were presented for each group and a one-way ANOVA was run to identify differences across groups. Within the group of participants with chronic SCI, confidence intervals are presented to compare behavior across PrU status.
RESULTS
We recorded 359 complete days across 31 participants with recent injuries and 225 complete days across 29 participants with chronic injuries. Participants in the two groups were predominantly male and of similar height and weight (Table 1). However, participants in the chronic group were significantly older than those in the acute group, which is consistent with the increased time since injury. The chronic group was more heavily biased towards complete low level injuries, while the acute group was spread more evenly between cervical, and upper and lower thoracic level injuries. More of the acute injuries were classified as incomplete.
Of the chronic participants, 12 participants had a history of recurrent pressure ulcers and 17 had not experienced any ulcers, or only had one immediately following their injury.
Participants spent an average (standard deviation) of 8.2 (3.8) hours in their wheelchairs per day (Table 2). During those 8 hours, participants transferred out of their wheelchairs 8.2 times per day. When including transfers back to their wheelchair, this implies a total of more than 16 transfers per day.
Those with recent injuries spent less time seated in their wheelchairs and wheeled a smaller number of bouts and a shorter distance each day. They also performed a slightly more transfers daily compared to individuals with chronic injuries, despite spending 3 fewer hours in their chairs.
| Acute | Chronic | P value | |
| Distance Wheeled (km) | 1.2 (1.1) | 1.5 (1.2) | 0.010 |
| # Bouts | 55 (32) | 84 (41) | <0.01 |
| % Mobile | 9.7 (8.5) | 8.1 (5.7) | 0.041 |
| Weight Shift Frequency (per hr in chair) | 3.8 (4.2) | 2.3 (2.3) | <0.01 |
| Pressure Relief Frequency (per hr in chair) | 1.2 (1.7) | 0.5 (0.8) | <0.01 |
| # Transfers Out of Chair | 8.6 (5.4) | 7.6 (4.5) | 0.024 |
| Time in Chair (hrs) | 7.0 (3.4) | 10.1 (3.8) | <0.01 |
On the whole, participants performed less than one full pressure relief per hour they were seated in the wheelchair (0.9 (1.5) pressure reliefs per hour). Weight shifts, on the other hand, were performed much more frequently, with the average day including 3.2 (3.6) weight shifts per hour. Participants with acute injuries were considerably more active in their seats than those with chronic injuries (Table 2).
Within the population of individuals with chronic injuries, in-seat movement was evaluated for differences between PrU groups. All participants with chronic SCI performed full pressure reliefs less frequently than once every 2 hours, regardless of PrU status. Weight shifts, on the other hand, were performed more frequently by those with no history of pressure ulcers (95% confidence interval [2.53, 3.39] versus [1.03, 1.69], (Figure 2)).
Discussion
![Figure 2. Figure two is an interval plot presenting the mean and 95% confidence intervals of weight shift frequency for individuals with and without a pressure ulcer history. There is a gap between the two intervals, as the mean and confidence interval of weight shift frequency for participants without a history of pressure ulcers is 2.96 [2.53, 3.39], while participants with a history of recurrent pressure ulcers performed weight shifts on average 1.36 time per hour [1.03, 1.69].](sonenblum/fig2.jpg)
In-seat behavior and wheelchair mobility differed considerably between people with acute and chronic SCI. The reduced mobility shortly after discharge could be attributable to the need to develop wheelchair skills and build strength and sitting tolerance. Environmental factors may also contribute to the reduced mobility, as participants’ homes may still need further accommodations, and accessible transportation options might not be available. Regardless of the reason, these results provide evidence that wheelchair use and behavior change following discharge, suggesting that the equipment and intervention needs of an individual following discharge are also likely to change with time.
Although they wheeled less, individuals with acute SCI performed more frequent weight shifts and pressure reliefs than those with chronic SCI. The pressure ulcer prevention education and training received during rehabilitation appears to be initially effective, but its impact decreases with time. Future work should investigate the timeline of changes to mobility and weight shift behaviors to optimize the timing for reevaluating interventions and repeating pressure ulcer prevention education.
The comparison of individuals with acute and chronic SCI used a cohort design, in which different populations were studied. The populations differed in terms of age and injury characteristics, and this could influence our results.
Despite subjective studies indicating that pressure relief behavior is unrelated to pressure ulcer outcomes, our results suggest that there is a difference in weight shifting between individuals with and without a history of PrU (Garber et al., 2000; Krause & Broderick, 2004; Raghavan et al., 2003). Our study is unique in that it captured weight shifts that resulted from functional activities in addition to pressure reliefs intended solely to relieve pressure. These results, combined with evidence describing the physiological benefits of weight shifts (Smit et al., 2013; S. E. Sonenblum & Sprigle, 2011; S. E. Sonenblum et al., 2014), support the importance of in-seat movement in PrU prevention.
References
Garber, S. L., Rintala, D. H., Hart, K. A., & Fuhrer, M. J. (2000). Pressure ulcer risk in spinal cord injury: predictors of ulcer status over 3 years. Arch Phys Med Rehabil, 81(4), 465-471. Retrieved from http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=10768537
Kosiak, M. (1959). Etiology and pathology of ischemic ulcers. Arch Phys Med Rehabil, 40(2), 62-69. Retrieved from http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=13618101
Krause, J. S., & Broderick, L. (2004). Patterns of recurrent pressure ulcers after spinal cord injury: identification of risk and protective factors 5 or more years after onset. Arch Phys Med Rehabil, 85(8), 1257-1264. Retrieved from http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=15295750
Martin, J. S., Sonenblum, S. E., & Sprigle, S. (2014). Signal processing for a wheelchair pressure relief monitoring system. Paper presented at the RESNA Annual Meeting, Indianapolis, IN.
Middleton JW, L. K., Taylor L, Soden R, Rutkowski S. . (2004). Patterns of morbidity and rehospitalisation following spinal cord injury. . Spinal Cord, 42, 359-367.
Raghavan, P., Raza, W. A., Ahmed, Y. S., & Chamberlain, M. A. (2003). Prevalence of pressure sores in a community sample of spinal injury patients. Clin Rehabil, 17(8), 879-884.
Reswick, J. B., & Rogers, J. (1976). Experience at Rancho Los Amigos Hospital with devices and techniques to prevent pressure sores. In R. M. Kenedi, J. M. Cowden, & J. T. Scales (Eds.), Bedsore Biomechanics (pp. 301-310). Baltimore: University Park Press.
Smit, C. A., Zwinkels, M., van Dijk, T., de Groot, S., Stolwijk-Swuste, J. M., & Janssen, T. W. (2013). Gluteal blood flow and oxygenation during electrical stimulation-induced muscle activation versus pressure relief movements in wheelchair users with a spinal cord injury. Spinal Cord, 51(9), 694-699. doi:10.1038/sc.2013.66
Sonenblum, S. E., Sprigle, S., Caspall, J., & Lopez, R. (2012). Validation of an accelerometer-based method to measure the use of manual wheelchairs. Med Eng Phys, 34(6), 781-786. doi:S1350-4533(12)00129-4 [pii]
10.1016/j.medengphy.2012.05.009
Sonenblum, S. E., Sprigle, S., & Martin, J. S. (In Press). Everyday sitting behavior of full time wheelchair users. J Rehabil Res Dev.
Sonenblum, S. E., & Sprigle, S. H. (2011). The impact of tilting on blood flow and localized tissue loading. J Tissue Viability, 20(1), 3-13. doi:S0965-206X(10)00067-7 [pii]
10.1016/j.jtv.2010.10.001
Sonenblum, S. E., Vonk, T. E., Janssen, T. W., & Sprigle, S. H. (2014). Effects of wheelchair cushions and pressure relief maneuvers on ischial interface pressure and blood flow in people with spinal cord injury. Arch Phys Med Rehabil, 95(7), 1350-1357. doi:10.1016/j.apmr.2014.01.007
Sprigle S; Sonenblum SE. (2011). Assessing evidence supporting redistribution of pressure for pressure ulcer prevention: A review. J Rehabil Res Dev, 48(3), 203-214.
Acknowledgements
The authors would like to acknowledge collaborators at Duke University and the Durham VA (Kevin Caves and Helen Hoenig), Shepherd Center (Chris Maurer, David Kreutz, and Jennith Bernstein, and Marina Moldavskiy), and Kessler Foundation (Trevor Dyson-Hudson and William Weber) for their efforts with participant recruitment and data collection.
This work was completed as part of the Mobility RERC, which is funded by the National Institute on Disability, Independent Living, and Rehabilitation Research, grant number H133E080003. Support for this study was also provided through the US Department of Defense, grant number W81XWH-13-1-0387.