Design And Testing Of An Agonist-Antagonist Switching Position-Impedance Controlled Myoelectric Prosthetic
Christopher Aymonin, Dr. Dianne Pawluk, Dr. Peter Pidcoe
Department of Biomedical Engineering, Virginia Commonwealth UniversityAbstract
Approaches to prosthetic hand control often focus on improving single handed grasping and manipulation. However, for those with unilateral upper-limb loss, clinical focus is on training the use of a prosthesis for helping with tasks that are difficult or impossible to do with a single hand. In many of these bimanual tasks, one hand is responsible for dexterous manipulation, while the other acts to primarily stabilize the object of interest. This paper describes the development of a low cost hand prosthetic designed to utilize co-contraction of the fingers and thumb to stabilize and assist in the manipulation of compliant objects that are common in many bimanual activities of daily living (ADLs). The prosthetic utilizes a Switching Position-Impedance controller that allows the user to control the aperture of the prosthetic using EMG signals, while the device modulates the impedance based on sensed compliance characteristics of the object of interest.
BackGround
Modern day myoelectric upper limb prosthetics provide a great opportunity to restore function to those who are missing limbs. They offer users advanced functionality compared to body powered prosthetics by utilizing the body’s neural signals for control. A number of impressively dexterous robotic hands have been developed, however the ability to fully control these sophisticated designs is limited by the number of neural inputs available, lack of sufficient sensory feedback, and usage of stiff actuators. These limitations make usage less intuitive, increasing cognitive load and often contributing to user rejection of the prosthetic (Spires 2014).
In addition, much of the research involving prosthetic hand control has focused on single hand grasping and manipulation with the prosthetic hand. However, typically, individuals who have hand prostheses have one healthy hand and one hand replaced by a prosthetic (Tennent et al., 2014). One handed tasks can more easily be performed by the healthy hand. Two handed tasks, though, require the use of the prosthetic hand. In many bimanual tasks, one hand (the healthy hand) requires dexterity while the other is used to maintain stability or perform less dexterous tasks. For example, cutting foods of varying compliance (e.g., tomatoes, bread, meat, etc.) on a cutting board requires one hand to cut and the other to stabilize the food without squishing it. A second example is squeezing a paste or gel from a tube (toothpaste, creams or other personal hygiene products) onto another item being held (e.g., a toothbrush) or a healthy finger for use.
For prosthetic control, components of the hand are typically controlled using distal surface electromyography (SEMG). Previous control schemes in commercial devices regulated the force or speed applied by the prosthetic in a manner proportional to the magnitude of the EMG signals or using a simple on/off control. Although these methods are commonly used in myoelectric prosthetics, it has been suggested that positional control, switching to force control on contact, is more appropriate for grasping. Another recent study found that a non-linear control algorithm was more effective than either of the two commonly used algorithms (Arenas 2015).
This paper describes the design of a simple, cost-effective hand prosthetic meant for stabilization and less dexterous components of a bi-manual task together with a dexterous, healthy hand. The design is simplified by coupling the movement of the fingers to each other, reducing the number of actuators needed. Control of the hand is through a biomimetic agonist-antagonist impedance controller, which allows for the automatic modulation of grip stiffness of the prosthetic, while allowing the user to control the position of the thumb-fingers grasp. The desirable stiffness is based on measured properties provided by sensors on the fingertips. Position control is achieved from a nonlinear relationship to 2 distal SEMG inputs.
Device Design
System Hardware
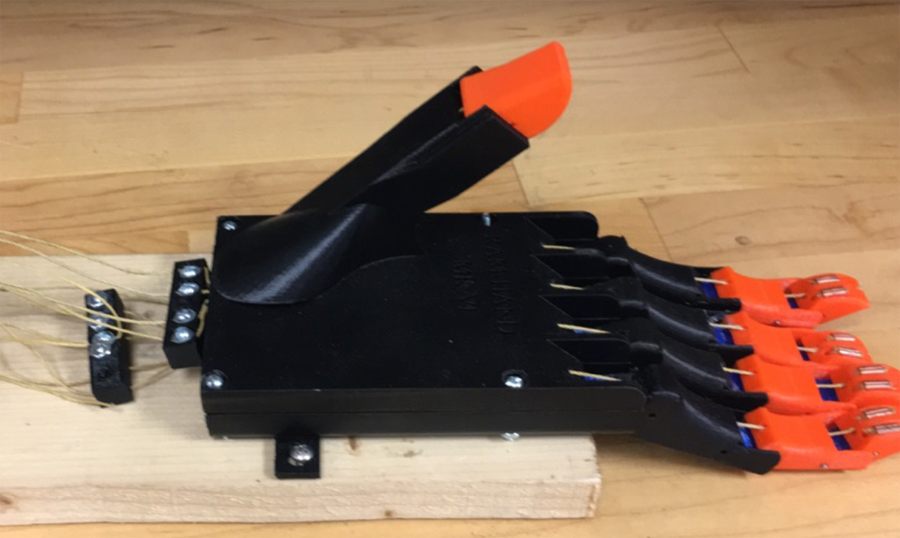
The prosthetic hand was printed using a Fused Deposition Modeling (FDM) 3D Printer using PLA and NinjaFlex™. The design has 13 degrees of freedom. Each finger has two interphalangeal joints and one metacarpal joint, while the thumb only has one degree of freedom at the interphalangeal joint. Only one hand configuration, a cylindrical grasp with the thumb in opposition, is implemented for specialized use as a complimentary hand for bimanual ADLs. Each of the fingers is connected to the other by flexible NinjaFlex™ joints that allow for flexion and extension movements.
A two channel bipolar electrode SEMG system is utilized as the user interface to control the position of the tip of the thumb and the tips of the fingers, respectively. One electrode is placed toward the end of the wrist as a ground, while electrode pairs are located on the wrist flexors and extensor of the user’s left (non-dominant) arm. The electrodes are placed in standardized locations. The SEMG system is calibrated for each user to recognize flexion and extension signals from the muscles as myoelectric input commands to be passed to the prosthetic. A non-linear control scheme is implemented for translating user EMG activity to positional commands (Arenas 2015).
The entire system is controlled using an Arduino Mega which is responsible for receiving sensory data, organizing the response to EMG signals, and directing behavior of the servos according to the desired motion.
Control System Architecture
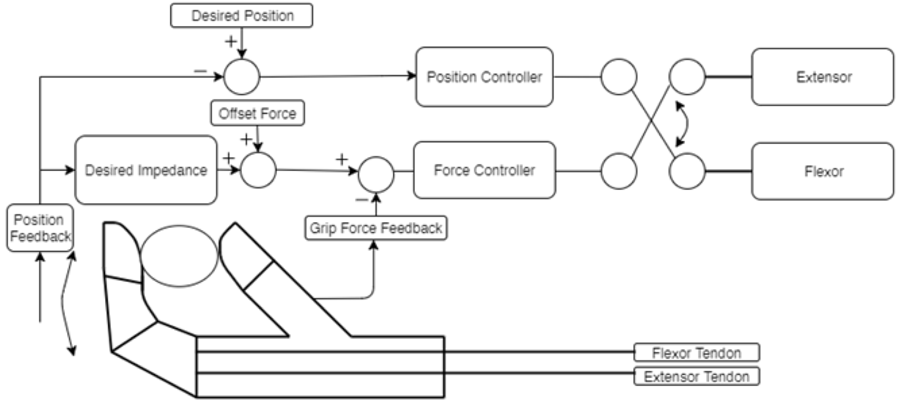
The prosthetic operates using a Switching Position/Impedance controller (Villalpando 2008). Depending on the prehensile state of the prosthetic and the desired action, the two motors, acting in opposition, will be operated by either a position controller or an impedance controller.
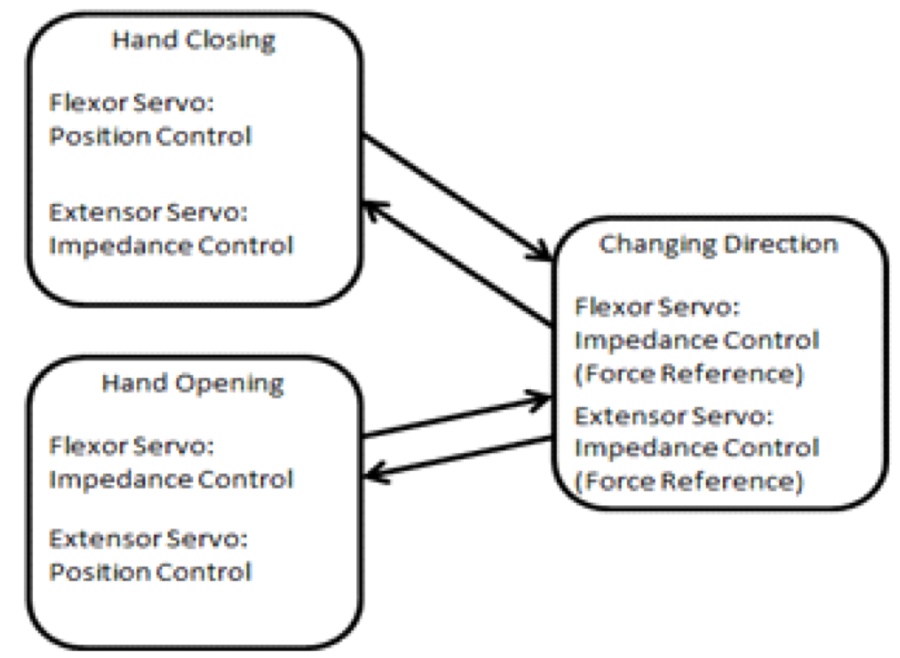
For example, when the user wants to grasp an object, the servo attached to the flexors will act as a position controller, while the opposing motor will control the stiffness of the hand by acting as an impedance controller. When opening the hand, the reverse will be true; the extensor will use positional control, while the flexor controls the impedance. The act of switching directions requires a more purposeful co-contraction in order to prevent tendon slackening, which can result in a loss of energy. In this case, both motors are controlled using an adaptive force reference within their impedance controllers (Syetozarevic 2011). A two channel EMG system will be used to collect the user’s movement intentions for motions from the user’s residual wrist flexors or extensors.
Outcome and Discussion
The proposed method is intended to provide improved performance over control schemes using fixed stiffness levels or schemes where users actively modulate co-contraction (Sesinger 2008). This will be shown through improved success at completing tasks, reduced mental load, and increased usability.
A prototype of the design and control has been implemented and is in its initial testing stage. The design was simplified by reducing the degrees of freedom and then coupling the finger and thumb movements together to reduce the complexity of use and cognitive load. This simplified design should still allow the prosthetic hand to succeed in many bimanual tasks for unilateral amputees, where it plays a supporting role to a more active and dexterous human hand: the goal of our prosthetic hand design.
The agonist-antagonist impedance controller was used to allow the prosthetic to modulate its stiffness in a way that mirrors the human hand in response to objects of various compliances. Information about the impedance of the object to be interacted with comes from the fingertip sensors, while the position is controlled by the user through two SEMG electrodes. The method is intended to provide improved performance and reduced cognitive load over control schemes where users actively modulate co-contraction. This comparison will be performed in future work.
Future Work
Assessment of the prosthesis is currently underway. The main objective is to compare the performance using an agonist-antagonist impedance controller for bi-manual tasks that involve stiffness modulation to that of other controllers both in terms of performance and usability. A fully self-contained wearable version of the device will also be developed for usage by trans-radial amputees. User testing and future device testing are planned with this target group.
Future plans also include investigating the tradeoffs between the number of degrees of freedom controlled and functionality. For example, one consideration is to utilize additional extensor lines actuated using solenoids in the palm in order to allow greater control over impedance through actuator redundancies. This will also grant the ability to lock the metacarpal joints in place for more direct control of the interphalangeal joints.
Finally, the incorporation of additional sensors (such as slip sensors) in the fingertips and wrist are planned in order to give the control algorithm greater insight into the texture, weight, shape, and size of the grasped object for more accurate manipulation.
References
Arenas, J.A. (2015). Evaluation of a Novel Myoelectric Training Device. Biomedical Engineering and Bioengineering Commons.
Sensinger, J., & Weir, R. (2008). User-Modulated Impedance Control of a Prosthetic Elbow in Unconstrained, Perturbed Motion. IEEE Transactions on Biomedical Engineering,55(3), 1043-1055. doi:10.1109/tbme.2007.905385
Spires, M. C., Kelly, B., & Davis, A. J. (2014). Prosthetic restoration and rehabilitation of the upper and lower extremity. New York: Demos Medical.
Svetozarevic, B., & Jovanovic, K. (2011). Control of Compliant Anthropomimetic Robot Joint. Serbian Journal of Electrical Engineering,8(1), 85-95. doi:10.2298/sjee1101085s
Tennent, D.J., Wenke, J.C., Rivera, J.C. and Krueger, C.A. (2014). Characterisation and Outcomes of Upper Extremity Amputations. Injury, 45 (6), 965-969.
Villalpando, E. C., Weber, J., Elliott, G., & Herr, H. (2008). Design of an agonist-antagonist active knee prosthesis. 2008 2nd IEEE RAS & EMBS International Conference on Biomedical Robotics and Biomechatronics. doi:10.1109/biorob.2008.4762919