Quantitative Assessment Of Compensatory Movements During Upper Limb Functional Performance
Sophie Wang1,2, Kimberly Kontson2, Eugene Civillico2
1University of Maryland, College Park, MD
2U.S. FDA, Center for Devices and Radiological Health, Office of Science and Engineering Labs, Division of Biomedical Physics, Silver Spring, MDAbstract
The Jebsen-Taylor Hand Function Test (JHFT), which is widely used in clinical settings, consists of seven standardized tasks based on activities of daily living. Although originally developed for individuals with neurological and musculoskeletal conditions, JHFT has also been utilized in the upper limb amputee population to evaluate rehabilitation progress and functional performance. Currently, the standard endpoint for each JHFT task is completion time. For upper limb prosthetic users, it is also important to assess how the subject performs each task: the completion time endpoint for JHFT is not sufficient to evaluate the potential compensatory movements (CMs) employed by subjects due to the loss of distal degrees-of-freedom (DoFs) in the arm. Through the use of motion capture technology, quantitative information on how the subject moves can be used to derive measures of movement quality, introducing assessments that are potentially more clinically meaningful than completion time alone. In this work, we demonstrate the use of motion capture data to capture quantitative information about how subjects complete three out of the seven tasks from the JHFT. To assess the ability of our motion capture system to capture CMs, subjects performed these tasks with the right hand under normal conditions, and under braced conditions in which the wrist DoFs were reduced.
Introduction
For persons with upper limb disabilities due to stroke, musculoskeletal disorders, or other conditions, there exist a number of validated observational outcome measures to assess functional capabilities. These types of measures are critical to characterizing the efficacy of a specific treatment or rehabilitation regimen. Only three of these measures have been specifically developed and validated for individuals with upper limb amputations (Lindner, Natterlund, & Hermansson, 2010; Wright, 2009). Others are not yet validated but have begun to be studied in the upper limb amputee population (Jebsen, Taylor, Trieschmann, Trotter, & Howard, 1969; Mathiowetz, Volland, Kashman, & Weber, 1985; Rider & Linden, 1988; Wright, 2009). One such example is the Jebsen-Taylor Hand Function test (JHFT) (Jebsen et al., 1969; Rider & Linden, 1988). In this test, subjects are asked to perform seven activities of daily living (ADLs): writing, page turning, picking up small objects, simulated feeding, stacking checkers, moving large light objects, and moving large heavy objects. Currently, the standard endpoint for each JHFT task is completion time. The quality of movement of the participant is not taken into consideration. Because the long-term consequences for prosthetic users will depend not only on the acquisition of certain environmental targets, but on the nature of the movements employed to do so, it is important to incorporate standardized, quantitative movement analysis into the assessment of function for the upper limb amputee population.
One way to acquire detailed analysis of movement is through the use of motion capture (Carey, Jason Highsmith, Maitland, & Dubey, 2008; Gates, Walters, Cowley, Wilken, & Resnik, 2016; Hebert & Lewicke, 2012; Kontson, Marcus, Myklebust, & Civillico, 2017; Major, Stine, Heckathorne, Fatone, & Gard, 2014; Metzger, Dromerick, Holley, & Lum, 2012). Motion capture enables the quantitative analysis of how segments of the body move relative to each other and to a global coordinate system. While there are several examples of studies that have investigated the use of this technology for the assessment of upper body function, none have collected kinematic data of subjects performing the JHFT.
In this work, we demonstrate the use of motion capture data to capture quantitative information about how subjects complete the JHFT. To assess the ability of motion capture to capture CMs during administration of the JHFT, subjects performed these tasks with the right hand under normal conditions, and under braced conditions in which the wrist DoFs were reduced. For the current analysis, only three of the seven JHFT tasks are presented. In addition to determining any differences in the kinematic trajectories of subjects under normal and braced conditions, this pilot study also serves to provide a preliminary normative data set for the JHFT tasks.
Methods
Subjects
For the pilot study, 4 subjects (2 males, 2 females, mean age 24.5 years, SD 1.7 years) with no upper limb disability were asked to perform the JHFT. All subjects were right-hand dominant. The study was approved by the Institutional Review Board (Research Involving Humans Subjects Committee) at the U.S. Food and Drug Administration (RIHSC #14-086R). All subjects provided written informed consent prior to participating in the study.
Tasks
Each subject completed all seven JHFT tasks twice with the dominant hand while in a seated position. Each of the tasks (except for Task 1 – writing) requires transport or manipulation of multiple objects. For the current analysis, only data from Tasks 2 (simulated page turning), Task 3 (picking up small objects), and Task 4 (simulated feeding) are presented. Future work will incorporate all tasks. A brief description of these tasks is given below. More detailed descriptions of all the tasks can be found in (Jebsen et al., 1969).
- Task 2- Page turning: The subject flipped over five 3x5 cm notecards arranged in a row with any technique, starting with the leftmost card and moving across.
- Task 3- Picking up small objects: The subject picked up six small objects (2 paperclips, 2 bottle caps, & 2 pennies) arranged two inches apart on the dominant side of the subject, five inches from the edge of the table, and placed them in an empty can individually. The subjects were asked to start with the rightmost object and work inward.
- Task 4- Simulated feeding: The subject picked up five kidney beans total (one at a time) arranged two inches apart on the dominant side of the subject with a spoon and dropped them in the empty can, starting with the rightmost bean.
Data Acquisition and Analysis
An eight-camera passive ViconTM motion analysis system was used to acquire and preprocess the motion data (Vicon, Oxford, UK). The Bonita B10 motion capture cameras collected data at a sampling rate of 150 Hz. Prior to each data collection session, the motion system was calibrated according to the manufacturer’s guidelines.
Twenty-seven reflective markers were placed on the upper body of each subject to create wrist, forearm, upper arm, head, neck, thorax and pelvic segments. The table on which the tasks were performed was adjusted such that the subject’s arms were positioned at a 90° angle when resting on the table. After calibrating the subject to the upper body model, the subject was given instructions for each task of the JHFT.
Three angles (right elbow flexion, right shoulder abduction, torso lateral flexion) were calculated from the Vicon upper body model using YXZ Euler angles derived from the comparison of relative orientations of two segments (Vicon Plug-In-Gait, Oxford, UK). These data were filtered using a 4th order, zero lag, lowpass Butterworth filter at 6 Hz. The motion capture data for each subject were segmented into trials: trial start was defined as the initiation of the approach to pick up an object and trial end was defined as the release of the object. For the three tasks presented in the current work, the last trial from each subject was used to determine the range of motion (RoM) and maximum angle value. Wilcoxon’s rank sum test was applied to test for statistical differences in completion time, RoM, and maximum angle between normal and braced conditions.
Results
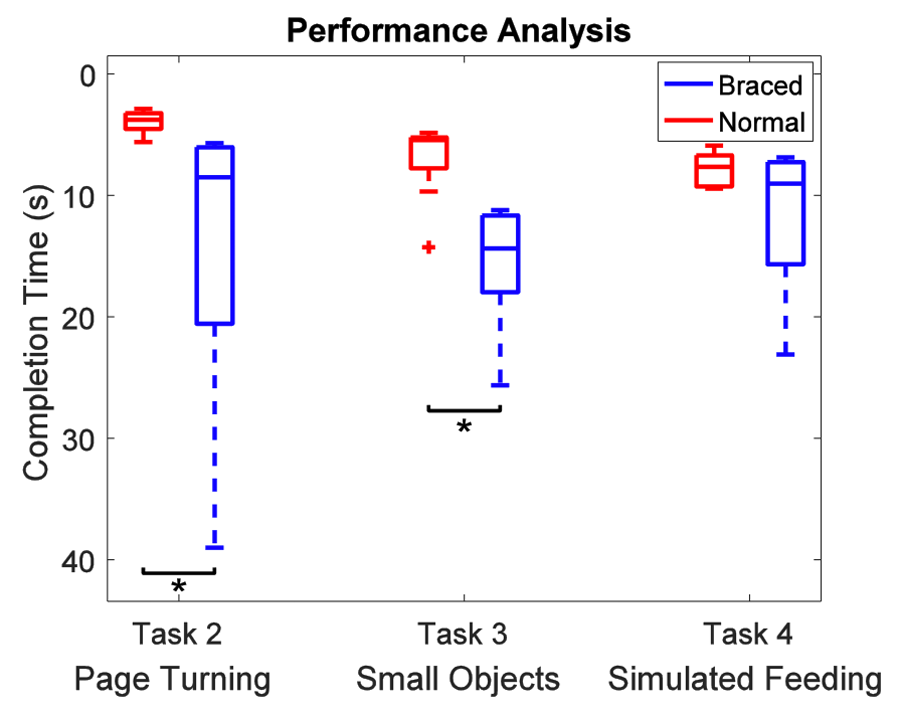
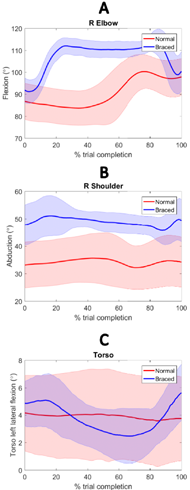
Kinematic trajectories for right elbow flexion, right shoulder abduction, and torso left lateral flexion were calculated for the last trial of each task. RoM and maximum angle from each subject’s trajectory for each task were computed for normal and braced conditions and are shown in Table 1. For Task 2, significant increases in the maximum torso lateral flexion and elbow flexion angles were seen when subjects performed the task under braced conditions. In Task 3, significant increases in both RoM and maximum angle value were observed in all calculated angles, except maximum angle of torso left lateral flexion. This can be seen in Figure 2 showing the average trajectories for Task 3. For example, Figure 2A shows elbow flexion remains fairly constant prior to subjects dropping the object in the can under normal conditions. Under braced conditions, subjects significantly increased elbow flexion at the beginning of the trial in order to pick up the object before transporting and releasing it in the can. There were no significant differences between normal and braced conditions for Task 4.
| Range of Motion | Max Angle | ||||
|---|---|---|---|---|---|
| Normal | Braced | Normal | Braced | ||
| R Sho Abduction | Task 2 | 9.5 ± 6.7 |
14.6 ± 8.1 | 46.2 ± 18.0 | 66.2 ± 21.1 |
| Task 3 | 5.8 ± 1.4 | 11.2 ± 3.1 * | 36.8 ± 9.2 | 54.8 ± 5.3 * | |
| Task 4 | 11.6 ± 8.8 | 21.0 ± 11.5 | 51.4 ± 21.1 | 56.4 22.8 | |
| R Elb Flexion | Task 2 | 18.1 ± 6.1 | 32.3 ± 16.6 | 93.0 ± 7.8 | 118.2 ± 7.1 * |
| Task 3 | 17.9 ± 2.3 | 26.7 ± 3.1 * | 100.8 ± 7.7 | 116.3 ± 5.5 * | |
| Task 4 | 25.4 ± 11.3 | 28.9 ± 16.1 | 108.0 ± 13.4 | 110.7 ± 11.8 | |
| Torso Left Lateral Flexion | Task 2 | 1.4 ± 0.8 | 4.8 ± 3.3 | 1.1 ± 1.5 | 3.6 ± 0.9 * |
| Task 3 | 0.9 ± 0.5 | 3.7 ± 1.3 * | 4.3 ± 3.0 | 6.1 ± 1.9 | |
| Task 4 | 2.2 ± 2.8 | 3.0 ± 1.6 | 1.8 ± 1.8 | 7.0 ± 4.3 | |
Discussion
References
Carey, S. L., Jason Highsmith, M., Maitland, M. E., & Dubey, R. V. (2008). Compensatory movements of transradial prosthesis users during common tasks. Clin Biomech (Bristol, Avon), 23(9), 1128-1135. doi: 10.1016/j.clinbiomech.2008.05.008
Gates, D. H., Walters, L. S., Cowley, J., Wilken, J. M., & Resnik, L. (2016). Range of Motion Requirements for Upper-Limb Activities of Daily Living. Am J Occup Ther, 70(1), 7001350010p7001350011-7001350010p7001350010. doi: 10.5014/ajot.2016.015487
Hebert, J. S., & Lewicke, J. (2012). Case report of modified Box and Blocks test with motion capture to measure prosthetic function. Journal of Rehabilitation Research & Development, 49(8), 1163-1174. doi: 10.1682/JRRD.2011.10.0207
Jebsen, R. H., Taylor, N., Trieschmann, R. B., Trotter, M. J., & Howard, L. A. (1969). An objective and standardized test of hand function. Arch Phys Med Rehabil, 50(6), 311-319.
Kontson, K., Marcus, I., Myklebust, B. M., & Civillico, E. (2017). An integrated movement analysis framework to study upper limb function: A pilot study. IEEE Trans Neural Syst Rehabil Eng(accepted).
Lindner, H. Y., Natterlund, B. S., & Hermansson, L. M. (2010). Upper limb prosthetic outcome measures: review and content comparison based on International Classification of Functioning, Disability and Health. Prosthet Orthot Int, 34(2), 109-128. doi: 10.3109/03093641003776976
Major, M. J., Stine, R. L., Heckathorne, C. W., Fatone, S., & Gard, S. A. (2014). Comparison of range-of-motion and variability in upper body movements between transradial prosthesis users and able-bodied controls when executing goal-oriented tasks. J Neuroeng Rehabil, 11, 132. doi: 10.1186/1743-0003-11-132
Mathiowetz, V., Volland, G., Kashman, N., & Weber, K. (1985). Adult norms for the Box and Block Test of manual dexterity. Am J Occup Ther, 39(6), 386-391.
Metzger, A. J., Dromerick, A. W., Holley, R. J., & Lum, P. S. (2012). Characterization of compensatory trunk movements during prosthetic upper limb reaching tasks. Arch Phys Med Rehabil, 93(11), 2029-2034. doi: 10.1016/j.apmr.2012.03.011
Rider, B., & Linden, C. (1988). Comparison of standardized and non-standardized administration of the Jebsen Hand Function test. Journal of Hand Therapy, 1(3), 121-123. doi: http://dx.doi.org/10.1016/S0894-1130(88)80036-X
Wright, V. (2009). Prosthetic Outcome Measures for Use With Upper Limb Amputees: A Systematic Review of the Peer-Reviewed Literature, 1970 to 2009. Journal of Prosthetics and Orthotics, 21(4S), P3.
Acknowledgements
The authors would like to thank Laura Woznicka and Sydney Barovsky for assistance in data acquisition. This work was funded in part by an interagency agreement with DARPA-BTO (IAA 224-14-6009), and by the FDA Critical Path Initiative (CPOSEL13).
Disclaimer: The mention of commercial products, their sources, or their use in connection with material reported herein is not to be construed as an actual or implied endorsement of such products by DHHS.