The People’s Stander: A Pediatric Therapy Stander For The Children Of Botswana
1) Problem Statement and Background
Ohio University 2016-2017 Senior Design Team 8 was tasked with designing, manufacturing, and assisting with the implementation of a pediatric physical therapy standing frame as their Senior Capstone Project. The standing frame must: fit a range of patients 2-8 years of age, be easily manufactured and assembled with hand tools and limited power tools, be inexpensive with respect to the current market for such devices with an initial target cost of $100 without labor, be able to move the patient from the prone to the fully upright position with a preference for additional supine position capability, be able to assist patients with a wide variety of disabilities (i.e. from pliant to stiff joints), comfortably support the patient for up to 2 hours of use, have an activity tray for the patient to use during therapy sessions, be user friendly for the caregivers to interact with the patient, be able to fit through a standard doorway, be liquid resistant in the case of patient accidents, preferably be transportable to Gaborone, Botswana by carry-on luggage but at least able to be implemented in Gaborone with detailed manufacturing and assembly plans. This project must be completed before the next annual Ohio University sponsored Physical Therapy trip to the Mariri Clinic in Gaborone, Botswana in July 2017.
2) Method/Approach/Solutions Considered
The team began the project with background research about standing frames for therapy, any relevant patents for related projects, and the economy and infrastructure of Botswana. At the first meeting with project partner, Dr. Janice Howman, the scope of the project was agreed on and the problem statement narrowed down to target specifications. The team was then able to begin designing with targets in mind. There were several steps the team took to create the final design.
The second step was to converge together and explain individual ideas to the team. Each member would talk about the why behind their sketches, what are the big benefits, and how it will achieve project goals. Other teammates examined the ideas and were instructed to discuss only the positives and advantages of each design. Each member received comments and suggestions for additions from the team. After the discussion each member had their eyes opened to improvements and deeper and further thoughts about their designs.
Next the team diverged again and each person worked to evolve their design(s) to ultimately obtain one final design. This design would be a mixture of their initial ideas, any new ideas, and comments from team members. The focus in this step is improving or combining to reach the final design. This final ideation step was crucial because it had a large impact on the decision of the final design that would be prototyped.
For the final convergence there were two important activities: Four-Blocker analysis and Decision Making Matrix. The Four-Blocker compares the effectiveness of a solution against the feasibility of implementing it. The team viewed effectiveness as a percentage of how many goals the design could accomplish and feasibility as the expected cost and level of difficulty to produce. This tool helped to visually determine what designs may be the best bet to proceed with. The final activity was the Decision Making Matrix. Team members voted on the individual final designs using a rubric to rate the designs for estimated cost, simplicity, and the ability to achieve specific targets. Each rating was weighted for its overall importance in the project as well (must have vs. nice to have) and the results were added. The final standing frame that is described in this brief was voted highest in all categories by each team member. After the decision for a final design was made by the team it was presented to the project partner and advisors. The team was approved to advance to engineering analysis and to build a budget.
3) Description of Final Approach and Design
Once the final frame and bed design was decided upon the team transitioned to deeper analysis and detailed design of joints, supports, and the patient bed. Material choices were first made for the frame, bed, and tray as these constitute the majority of the device. 2”x4” soft pine dimensional lumber and OSB plywood were used for these components to continue with the theme of simplicity and low-cost. Soft pine and OSB plywood is also readily available in the Botswanan economy. It was determined through calculation that 1”x2” lumber would be much more than was required to withstand fracture failure but the deflection of the beams would be a concern. 2”x4” lumber was used to reduce the estimated deflection to an unnoticeable level. 0.5” thickness OSB plywood was used for the activity tray and footplate for similar reasons. Simple straight and 45° angle cuts were specified for the lumber to eliminate the need for complex fabrication tools. It was deemed necessary to create a standing frame specifically for Mariri Clinic that featured quicker adjustability between patients and increased durability. This frame was named the Clinical Version and is displayed in the image below.

Sanding was required for the patient’s inner leg support to create a smooth, rounded end for the foam to contour to and reduce risk of injury to the patient if they were to impact it suddenly. The activity tray was extensively sanded to a very smooth surface finish to prevent any injury from splinters and to allow for the best paint adhesion. Further cutting was also required for the heel cups to reach the dimensions provided by the physical therapy team. The device was coated with bare wood primer, latex paint, and non-toxic poly-acrylic once all wood fabrication and major component assembly was complete. The patient bed on the Clinical Grade was upholstered by Ohio University Interior Services to ensure a professional level of craftsmanship for comfort and durability. Both the Individual and Clinical version were tested by the Physical Therapy team with young patients to determine the successfulness of the project.
4) Outcomes
| Clinical Version | Individual Version | |||
| Part Name | Cost | Part Name | Cost | |
| Threaded Galvanized Pipe | $20.04 | Threaded Galvanized Pipe | $20.04 | |
| Hex Head Zinc-Plated Screws | $9.63 | Hex Head Zinc-Plated Screws | $9.63 | |
| Nylon-Insert Locknuts | $4.55 | Nylon-Insert Locknuts | $4.55 | |
| Zinc-Plated Steel Washers | $2.46 | Zinc-Plated Steel Washers | $2.46 | |
| Galvanized Pipe Fittings | $9.14 | Galvanized Pipe Fittings | $9.14 | |
| Zinc-Plated Phillips Screws | $7.41 | Zinc-Plated Phillips Screws | $7.41 | |
| Hitch Pins | $21.76 | Zinc-Plated Steel Eyebolts | $6.84 | |
| Nylon Inserts | $26.73 | Easy Splice Rope | $5.00 | |
| Zinc-Plated Steel Eyebolts | $6.84 | Casters | $30.88 | |
| Easy Splice Rope | $5.00 | PVC | $3.55 | |
| Casters | $43.88 | Polyacrylic Wood Finish | $19.23 | |
| Paint & Primer | $17.96 | Wood Glue | $2.08 | |
| PVC | $3.55 | Lumber | $43.02 | |
| Polyacrylic Wood Finish | $19.23 | 1" Super Lux Foam | $26.98 | |
| Wood Glue | $2.08 | Polypropylene Straps | $28.63 | |
| Lumber | $43.02 | Vinyl | $19.99 | |
| 1" Super Lux Foam | $26.98 | Staples | $5.44 | |
| Polypropylene Straps | $28.63 | - | - | |
| Vinyl | $19.99 | - | - | |
| Staples | $5.44 | - | - | |
| - | - | - | - | |
| Total Cost | $324.32 | Total Cost | $244.87 | |
Two prototypes were constructed, initially a model of the individual, “People’s” stander, and then a fully operational clinical grade standing frame. The detailed design for the patient support and footplate sub-assemblies were created using ASTM standards for children between the specified ages of two and eight years old. Construction of the prototype was carried out following dimensions created in the detailed 3D Computer Aided Design (CAD) model; this was adequate for creating the general frame and making it adjustable throughout the specified patient range, but was less effective at simulating how patients might fit with foam and vinyl on the patient bed. Also, the ergonomics with regards to how a patient might utilize the activity tray were somewhat difficult to model, depending on different patient ailments and sizes. The foam and vinyl upholstering for the first prototype was done by the engineering team, with limited experience in this kind of work. Testing the initial prototype with children was necessary to ensure proper patient fit as well as proper function of the overall design.
The first round of testing was carried out with the project partner Dr. Janice Howman and assisted by Shandra Hamilton, our physical therapy student teammate. The two test subjects were normally developing children at the ages of three and seven years old. Upon testing with these children and the physical therapists, a number of issues were found that were not obvious from examining the Failure Modes and Effects Analysis (FMEA) or CAD model. The frame design was mostly adequate in general. The engineering team determined that the joint between the A-frame gusset and upright was not as strong as initially modeled. This weakness was due to wood splitting at the screwed joint; this was mitigated by designing a plate from the remaining stock wood to fasten the two boards together.
The main design flaws found in the initial testing with children were with how patients fit in the patient support bed and footplate assembly. The prototype upholstering was crude and although it properly protected the patient from open wood surfaces and the foam from moisture it needed improvement. The foam required better contouring to the patient’s body to properly support patients in the lateral direction. Another issue was the location of the heel cups and footplate gussets, which limited the position of both patients’ feet so that their knees were hyperextended, making the stander uncomfortable to use. The location of the footplate gussets limited the range of adjustability so that the patients on the younger end of the age range would not be able to reach the footplate with their feet; their groin would be resting on the inner lateral support.
To fix these design flaws, the patient bed was shortened to accommodate smaller sized children. The team had the patient bed professionally upholstered with thinner foam to properly support the patient, limit hyperextension of the knees, and appear more professional and medical grade. The footplate assembly was redesigned to fully alleviate the hyperextension of patient’s knees; this was done by fabricating thinner heel-cups, elongating the footplate rearward towards the heels, and adding additional holes for four total ranges of heel-cup adjustability. The footplate gussets were redesigned to be placed on the bottom of the footplate to increase adjustability for patient height without sacrificing strength or rigidity of the footplate. The tray was also shortened to mitigate a pinch point risk between the swinging patient bed and the edge of the tray, which was also more ergonomic for patients to reach the activity tray. These design changes were implemented in the second clinical grade prototype. The second prototype was tested both with normally developed children, as well as a young person with Down’s syndrome; it was determined to be a complete success for children within the size range that was intended.
5) Cost to Produce
The tables below detail the cost breakdown of the Clinical and Individual Versions. The Clinical Version is designed be adjusted multiple times a day for the use in a clinical setting, whereas the Individual Version is designed for only one patient such as in the home. The initial target cost of $100.00 was not sufficient to build either the Clinical or the Individual version. The project partner agreed that the cost to produce is acceptable although it is higher than the target cost. Due to the exchange rate of the value of goods the People’s Stander will cost less to produce in Botswana than in the US (the US cost is above). In comparison to an affordable stander on the market that meets the same needs as the clinical stander, the People’s Stander Clinical Version is a 600% cost reduction.
6) Significance
The People’s Stander will have a significant impact on the people of Gabarone, Botswana. Children at the Mariri Speech and Hearing Clinic with disabilities like cerebral palsy or muscular dystrophy are unable to bear weight on their legs unless supported by a standing frame. As previously stated, The People’s Stander was designed with simplicity in mind so that it can be recreated by the families in Botswana for a reasonable price. Current standing frame models range from about $1,500-$4,000 US. Due to the high poverty rate in Botswana, it would take an above average earning family many years to be able to afford a stander on the low end of the cost range. The inexpensive People’s Stander will provide the clinicians with a wider range of therapy to improve the lives of the children overseas.
There are both physiological and psychological benefits to using The People’s Stander as opposed to the current method used at the Clinic (Picture shown below). Using The People’s Stander will improve skeletal development, circulation, respiration, bowel and bladder function, as well as range of motion. It will also decrease muscle contractures and reduce swelling in lower extremities. In addition, The People’s Stander will also promote social interaction with others by enabling eye-to-eye communication, which then improves the patient’s alertness and energy in general.
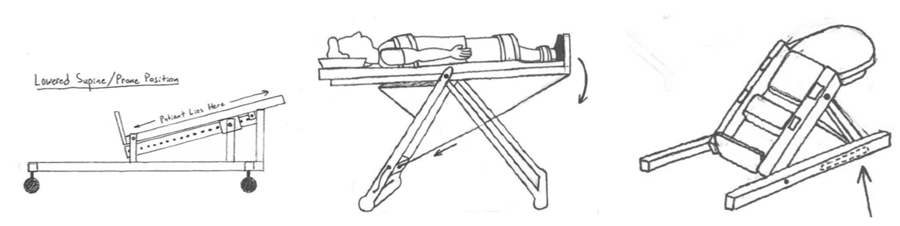
The People’s Stander will immediately improve the lives of those who use it. Since the device is capable of multiple positions, it has the ability to adjust based on the patient’s needs. The stander can reach prone position, where the patient is on his or her stomach tilting slightly forward, which promotes head control and increases upper body strength. The device can also move to the upright position, which replicates natural standing posture. Because The People’s Stander has a wide range of motion, as well as patient size adjustability, it can be used to treat any child that walks through the doors of the Mariri Clinic.
References:
"Child Growth Standards." World Health Organization. Accessed September 7, 2016. http://www.who.int/childgrowth/standards/en/.
“Medical equipment in general.” ISO 11.040.01. Accessed September 8, 2016. https://www.iso.org/ics/11.040.01/x/.
7) Acknowledgements
The team would like to give a very special thanks to the following individuals:
Dr. Gregory Kremer, Ohio University Mechanical Engineering Department Chair
Dr. Timothy Cyders, Ohio University Mechanical Engineering Department
Dr. Janice Howman, Ohio University Physical Therapy Division
Dr. Gary Chleboun, Ohio University Physical Therapy Division Director
Dr. Robert Wayner, Ohio University Physical Therapy Division
Zoe and Owen Wayner, Test Patients
Duane Perpich, Ohio University Interior Services
Trisha Putman, Ohio University Interior Services
Rich Tumbleson, Team Mentor
Suzanne Tkach, Team Mentor