UniTherapy: Software Design and Hardware Tools of Teletherapy
ABSTRACT
This paper presents the design and implementation of Unitherapy, a platform utilizing mass-marketed force-reflecting joysticks and other input devices to provide interactive upper limb assessment and therapy. Included among the input devices is the TheraJoy, a larger version of a remodeled joystick that includes additional motors, and operation in both horizontal and vertical modes. UniTherapy includes a Patient Interface (PI) and Local Practitioner Interface (LPI) /TelePractitioner Interface (TI), with assistive and accessibility features. This software suite includes a number of control modes and assessment protocols, all aimed at making Computer-Assisted Motivating Rehabilitation (CAMR) techniques more viable for home-based upper limb neurorehabilitation with teleassessment capabilities.
KEYWORDS:
Telerehabilitation, input devices, neurorehabilitation, impedance control, joysticks
BACKGROUND
The prevalence of stroke in American society is increasing, and over half of those who survive have arm impairment. Clinical trials with upper limb rehabilitators developed by several groups have provided evidence of improvement in the subjects' motor recovery of performance (1,2). However, with the dramatic reduction of inpatient rehabilitation length of stay following stroke, as well as inadequately supported self-therapy protocols for outpatients, it is now critical to develop cost-effective, easily used and scientifically-validated interventions (2,3). There is also evidence that carefully-designed computer-assisted home-based rehabilitation programs can work (1, 4), and that telerehabilitation-based therapeutic interventions can be effective (5). This project builds on other efforts at web-based therapy (6), and targets software development for Computer-Assisted Motivating Rehabilitation (CAMR) technologies (1) intended specifically for individuals with stroke-induced disability.
METHOD
To maximize input device connectivity within the Windows environment, we use Microsoft's DirectX SDK, a library of multimedia development tools that is now used widely in the PC gaming industry. Coding is mostly in C#, within the Visual Studio .Net programming environment. Input devices can be connected to a single PC or multiple PCs. UniTherapy software (see Figure 1) supports multiple platforms, which include desktop, laptop, tablet PC and PDA touchscreen pointers (PocketPC).
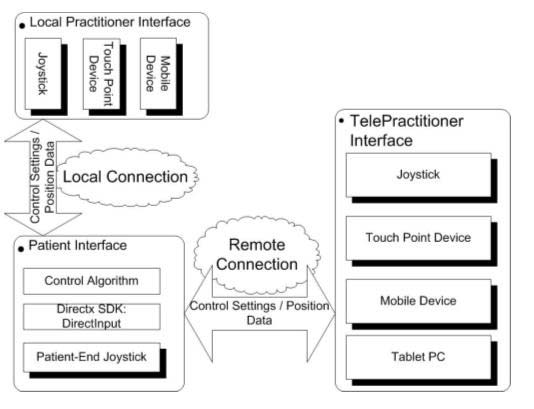 |
An infrastructure between PI and LPI/TI is successfully implemented. PI supports force-reflecting joysticks, which are used as upper limb rehabilitators. LPI/TI supports a variety of interfaces, which range from joysticks to touch screen pointers on a mobile device. Both PI and TI support a network connection. The local practitioner/telepractitioner can change the patient's force-field and rehabilitator impedance settings. Wireless connectivity (WLAN IEEE 802.11 or Bluetooth) is also supported, as is a simple voice-control mode. It also includes graphics tools for displaying targets and signals in various forms.
Four modes of robot assistance are defined; fine-tuning these modes remains an ongoing research and development activity: (1) Bi-manual mode : The subject at the PI uses two force-reflecting joysticks together, with the non-impaired arm able to assist and feel the impaired arm. (2) Assessment mode : The subject at the PI completes goal-directed tracking tasks intended to evaluate neuromotor performance, with the practitioner able to selectively observe and record patient's performance data and change control settings. (3) Passive training mode : The subject at PI uses one force-reflecting joystick with his impaired arm, with a predefined therapy program prescribed for the joystick that provides automated therapy (under supervision by practitioner). (4) Interactive control mode : Telepractitioner participates in therapy by cooperative assistance or resistance with the subject during goal-directed computer-assisted therapy.
Performance data is displayed in real-time, with additional approaches for viewing data available afterward for both patients and practitioners to observe, including through telerehabilitation. Accessible features are to be integrated into the design. One example, already implemented, is the use of voice control for the force-reflecting joystick. Also, the user can take advantage of embedded mouse accessibility features (e.g., to adjust the mouse pointer's speed).
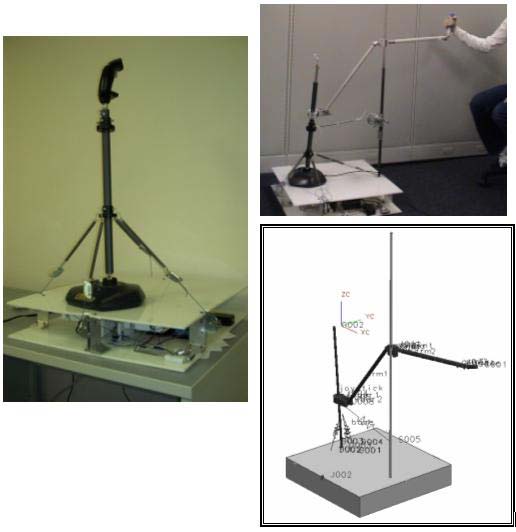 |
In addition to use of standard commercial computer input device, our group has designed a larger, customized device called the TheraJoy (7). This device extends a commercial mass-market force-reflecting joystick so that it is applicable to arm movements that include the shoulder. The joystick shaft and handle were lengthened to roughly 1 meter to accommodate a larger range of motion, with a telescoping component allowing shorter or longer lengths. Springs were added to create a mild potential energy field that more than compensates for a slight inverse pendulum linkage effect in what are nearly horizontal plane movements (Figure 2, left), and thus the device automatically returns to a centered resting position. In a second-generation version, linear motors were added, controlled through the parallel port, which added a user-centered potential energy field effect that could move within the user's workspace. Also, an arm attachment, first designed with a three-dimensional mechanical modeling package, has been added to convert this motion into the vertical plane as well (Figure 2, right). Kinematic mapping between the new hand interface and the original joystick has been accounted for through the use of a combination of sliding and pin joints. An additional variable spring has been added from the joystick to the fixed post to allow the device to be tuned to remain at its centered resting position with the addition of telescoping extension or for persons who need anti-gravity assistance to hold up their arm. The user may also adjust the handle grip angle for ease of use.
RESULTS AND DISCUSSION
While our primary focus has been on force-reflecting joysticks (of which the TheraJoy is one example), we now can access any Windows USB plug and play device that interfaces to the joystick and mouse ports, as well as pointing devices on PocketPC devices and certain technologies interfacing through the parallel port. With basic controller settings, the unloaded joystick at PI can be made to follow the position of TI closely. Further work is needed to refine impedance controller modes. Software interface windows have been customized for both PI and TI, with the telepractitioner terminal having more features and the ability to change options for the patient/client terminal. By using forces, we have taken advantage of DirectX capabilities to implement stiffness, dashpot and inertia modes for each terminal device, and can additionally pass forces that depend on the kinematics of the initial device.
A variation of this software has been used in a study involving six subjects with varying degrees of stroke-induced hemiparesis that were first assessed by several standard neurorehabilitation assessment instruments. The assessment tasks started with systematic marker tracking to identify the subject's arm workspace. This was repeated with different force assist settings for subjects lacking a full range. In this way subsequent tracking tasks could be adjusted so that targets didn't move into regions that were impossible for the subject. This study focused on usability and performance for a suite of two-dimensional tracking tasks. Performance metrics were quite similar to those used for Java Therapy (6), such as movement times and path errors were gathered for a protocol of tasks. Subjects also completed a questionnaire, and were found to be quite enthusiastic about the potential of the TheraJoy technology.
In summary, a basic software infrastructure for a low-cost rehabilitator platform has been successfully implemented. Further work is necessary to provide interactive assessment and therapy. UniTherapy provides a universal interface for all DirectX-compliant joysticks and pointing devices, and other rehabilitators or wireless sensors could integrate into this platform seamlessly.
REFERENCES
- Bach y Rita P, Wood S, Leder R, Paredes O, Bahr D, Bach-y-Rita EW, Murillo N. (2002) Computer assisted motivating rehabilitation for institutional, home, and educational late stroke programs. Top Stroke Rehabil. 8(4):110.
- Reinkensmeyer D, Lum P, Winters JM. (2001) Emerging Technologies for Improving Access to Movement Therapy following Neurologic Injury. In Emerging and Accessible Telecommunications, Information and Healthcare Technologies , ed. JM Winters C Robinson, R Simpson, G Vanderheiden, Arlington : RESNA Press.
- Winters, J.M., Wang, Y. and Winters, J.M. (2003) Wearable Sensors and Telerehabilitation: Integrating Intelligent Telerehabilitation Assistants With a Model for Optimizing Home Therapy, IEEE/EMBS Magazine, Special Issue on Wearable Medical Techn ., 22: 56 -65.
- Widén-Holmqvist L, von Koch L, Kostulas V, Holm M, Widsell G, Tegle RH, Johansson K, Almazan J, & de Pedro Cuesta J. (1998). A randomized controlled trial of rehabilitation at home after stroke in south-west Stockholm . Stroke , 29, 591-597.
- Rosen MJ, Lauderdale D, Winters JM. (2002) Summary of the State of the Science Conference on Telerehabilitation, in Emerging and Accessible Telecommunications, Information and Health Technologies, ed, JM Winters, C. Robinson, R. Simpson, G. Vanderheiden. Chapter 18, pp. 220-245, Arlington : RESNA Press
- Reinkensmeyer, D.J., Pang, C.R., Nessler, C.A., Painter, C.C. (2002) Web-based telerehabilitation for the upper-extremity after stroke, IEEE Trans Neural Science & Rehabil. Engng. , 10: 102-108.
- Ellsworth C. and Winters JM. (2003) An Innovative System to Enhance Upper-Extremity Stroke Rehabilitation, Proc. IEEE/EMBS , 4 p, Cancun , IEEE Press.
ACKNOWLEDGMENTS
This work is supported in part by the Falk Medical Trust Foundation, Rehabilitation Engienering Research Center on Accessible Medical Instrumentation H133E020729, and the Rehabilitation Engineering Research Center on Telerahabilitation H133E99007.
Author Contact Information:
Xin Feng , MS ,
Marquette University ,
Department of Biomedical
Engineering,
206 Olin Engineering,
1515 W. Wisconsin Ave,
WI
, 53233 ,
EMAIL: xinfeng@mu.edu