Functional Characterization of Disability and Interface Use
ABSTRACT
This paper presents a new approach for characterization of disabilities in terms that are specific to interface use and more practical than characterization by variables such as etiology, onset, progressive nature and severity. Characterization by these latter variables results in 100 - 200 different disability groups which is unworkable in research and product design. Researchers at Trace R&D Center are applying a new methodology for characterizing disabilities in terms that are specific to technology and interface use. The goal is to develop methods for characterizing disability and interface use that are both more useful to industry, and will lead to a much smaller set of functional categories than the 100-200 that result from traditional approaches.
KEYWORDS:
functional characterization; metrics; interface design; accessibility
BACKGROUND AND SIGNIFICANCE
A research priority of the National Institute on Disability and Rehabilitation Research (NIDRR) is to develop innovative technological solutions for, and promote universal access to, current and emerging information technologies and technology interfaces that promote a seamless integration of multiple technologies used by individuals with disabilities in the home, the community, and the workplace.
This is a huge undertaking and a key element of this priority is the ability to promote universal access . This is access by not just one type of disability, but all types of disabilities. To accomplish this task we need to understand the functional characterizations of the different types, degrees, and combinations of disability as well as their interface requirements.
Individuals with disabilities can be categorized as having vision, hearing, physical or cognitive impairments. If this type of categorization was sufficient for design, accessibility would be challenging, but at least there would only be four distinct groups to accommodate. In reality, these groups are even more diverse and their differences can affect product accessibility and design. There isn't one type of movement disorder but many (tremor, paralysis, spasticity, gross motor versus fine motor deficits, etc.) with completely different challenges occurring for operation of standard devices. A feature on a product that would make it accessible to someone having one type of physical impairment may be of little or no value to others with different physical impairments.
There are numerous metrics currently used for characterizing function in individuals with physical disabilities. Some commonly used measures include the Purdue Pegboard Test [1], the Extended Disability Status Scale [2], the Fugl-Meyer Assessment [3] and the Katz Index of Activities of Daily Living [4]. These tests provide information about functional abilities such as gross movements (hand to mouth), grasping and pinching activities and an individual's ability to perform ADL's (e.g. hygiene, dressing, etc). But it is difficult to relate results from these measures directly to interface requirements for information technology use.
APPROACH
From the human factors work system model, three domains were identified to use for functional characterization: (1) individual, (2) task, and (3) tools/technology. The individual domain was further broken down into the following categories: 1) impairment type, 2) severity of disability, 3) age of onset and 4) progressive nature of the disability. The domains of task and tools/technology are interrelated since the task execution is determined by the interface and the type and purpose of the technology device often dictates the interface. The physical characteristics and interface strategies (which dictates how the task is executed) of information technology devices that are currently available need to be cataloged. In addition, due to the rapid changes in technology, the anticipated characteristics of emerging devices also need to be considered. Examples of the physical properties of the device are weight, dimension, activation force and button characteristics. The interface strategies include control and display methods. The combination of individual disability characterizations, interface strategies, control and display methods and physical properties of the device result in the identification of the necessary elements for operation of information technology devices.
DIMENSIONS/CELLS
 |
|---|
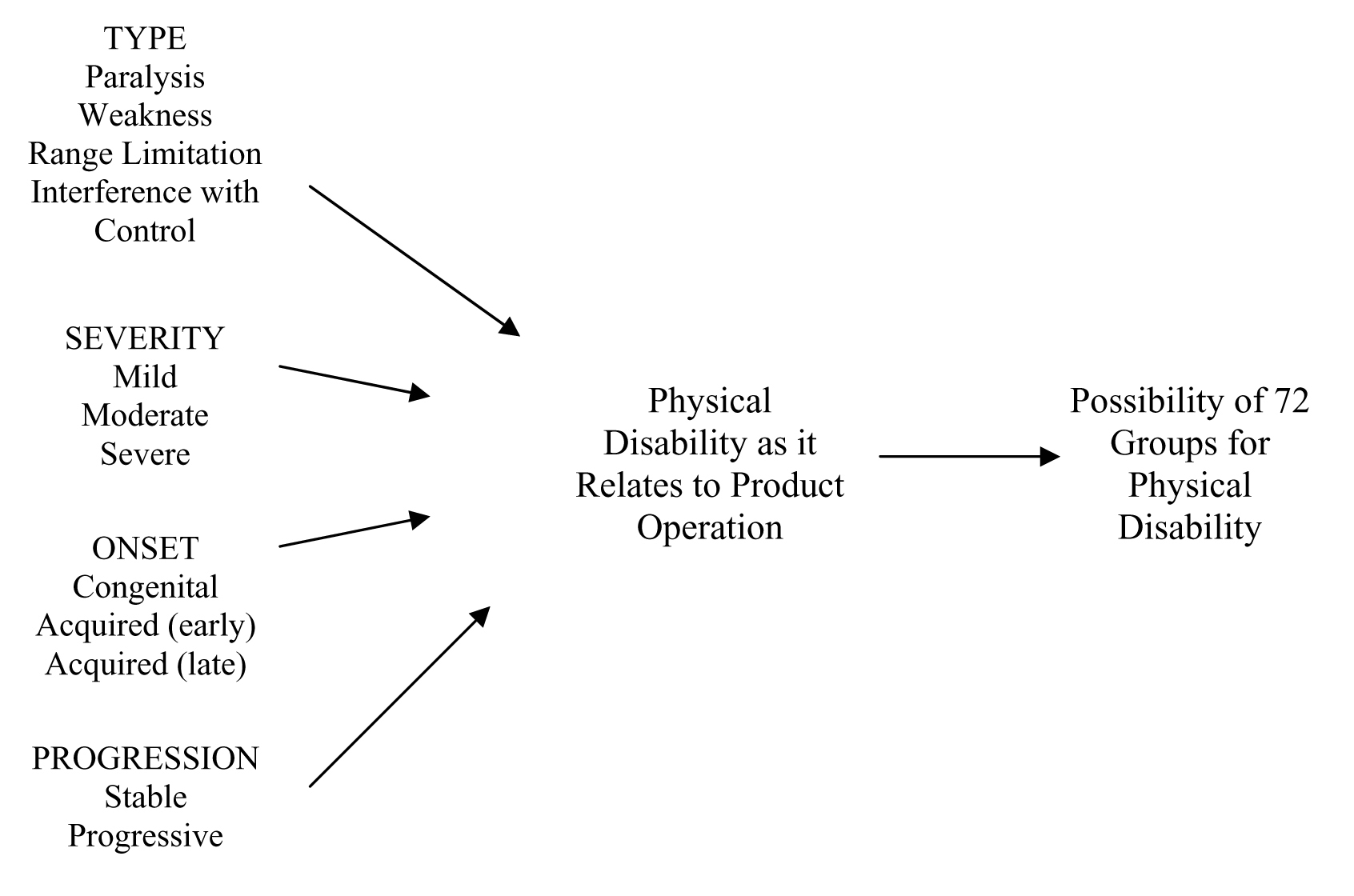
Classification of the different, distinct individual groups was done based on impairment type, severity, age of onset and progression of the disability (Figure 1). Specific to function, physical impairment type may be divided into four distinct subsets: 1) paralysis, 2) weakness, 3) range limitations, and 4) interference with control. Functional abilities and limitations may be affected by: 1) the severity of the disability, mild, moderate or severe, 2) the age of onset, congenital versus acquired and the age when the disability was acquired (young versus old) and 3) the progression of the disability (stable versus progressive). The combination of these four variables, 1) physical impairment type (4 subsets), 2) severity (3 levels), 3) age of onset (3 levels), 4) progression of disability (2 levels), may result in the possibility of 72 distinct groups just for physical disability. Each of the distinct groups may have different problems using products that need to be addressed and tested. In addition, some types of disabilities interact with others (e.g. physical and cognitive impairments, or deafness and blindness).
CELL REDUCTION
It is clear that designers or researchers cannot deal effectively with the topic of accessibility if it is going to require that they try to understand and/or test products with more than 100200 distinct groups of individuals. It is necessary to consider people with disabilities not in broad categories, but rather in terms of the specifics that impact the design of products. If individuals' disability type, age of onset, progression and severity is sufficiently different, such that the product or feature has to be designed differently in order for them to use it, then they should be considered as different groups, and the product design must be checked against these groups if access by them is intended.
Fortunately, just as careful examination shows that there is a tremendous diversity in disability, and that these differences are significant, this examination also reveals that at least some flexible interface strategies have been developed that work across broad ranges of individuals with varying types, degrees and onset of disabilities [5]. Therefore, it seems reasonable to assume that there is some way to collapse this large number of groups (defined by etiologies, severity, progression, and onset) into categories or characteristics that are more manageable in form and number (defined by their abilities to operate interfaces).
FUNCTIONAL EQUIVALENCE CONCEPT
To explore this we have developed a concept of Functional Equivalence. This is based on a hypothesis that different etiologies, can result in conditions that are functionally similar and have a common solution that can address the needs of all. This will be explored through the development of generalizable methods to characterize the functional abilities and limitations of individuals with disabilities in terms that are meaningful to interface developers and designers, and to develop a set of cross disability functional metrics. We are starting with one sub area, that being tremors, choreatic and athetotic movements. We are reporting our progress, hypothesis, and approach here to identify others interested in linking to this important and difficult endeavor.
IMPLICATIONS
This research can ultimately lead to metrics that will be used for characterization of functional abilities and deficits of individuals with varying disabilities that will be useful to researchers and product designers. In addition, if this research is successful, we will have a model that has the capacity to characterize functional abilities of individuals with disabilities along dimensions that are more practical than individuals' etiologies. This project will develop better quantification and characterization of tremors, choreatic and athetotic movements and a better means to relate the characteristics of these disabilities to the functional requirements of the interface of information technology.
REFERENCES
- Spreen, O., Strauss, E. (1991). A compendium of neuropsychological tests. New York: Oxford University Press.
- Cohen, J.A., Kessler, H.R., Fischer, M. (1993). The extended disability status scale (EDSS) as a predictor of functional activities of daily living in multiple sclerosis. Journal of the Neurological Sciences, 115, 132-135.
- Berglund K, Fugl-Meyer AR. (1986). Upper extremity function in hemiplegia: a cross validation study of two assessment methods. Scand J Rehabil Med,18, 155-175.
- Brorsson B, Asberg KH. (1991). Katz Index of Independence in ADL: reliability and validity in short-term care. Scand J Rehabil Med , 23,187-191.
- Vanderheiden, G. C., Law, C. M., & Kelso, D. (1999). EZ access interface techniques for anytime anywhere anyone interfaces. Proceedings of the Association for Computing Machinery Conference on Human Factors in Computing Systems (ACM CHI 99) , 3-4.
ACKNOWLEDGEMENT
This work was primarily funded by the National Institute on Disability and Rehabilitation Research (NIDRR) through the U.S. Dept. of Education, grant number H133E030012. The opinions expressed here do not necessarily represent the policy of the U.S. Dept. of Education.
CONTACT
Mary Sesto, P.T., Ph.D.,
sesto@trace.wisc.edu
Trace Research and Development Center
2107 Engineering Centers Bldg,
1550 Engineering
Drive,
Madison, WI 53706