Rule-Based Neuro-Fuzzy Models for Event-Driven Adaptive Prognosis and Context Prediction
ABSTRACT
This paper describes a dynamic recurrent neuro-fuzzy system for creating dynamic models that are rule-based and event-driven. It is intended mainly for clinical prognosis prediction, but it also can be used to provide the type of context-awareness that is need for an intelligent personal assistant for consumers or practitioners, and as a tool for creating a range of nonlinear dynamic models and controllers . Four layers are implemented as clusters of artificial neurons: input, rule-state, output, and outcome. The system is designed with an interactive graphical user interface to facilitate rule creation by clinical experts. Interactive sensitivity analysis is available to help users understand how changing rules or describing parameters affects predictive behavior. Both supervised learning and reinforcement learning approaches are adopted for optimization, enabling tuning of system parameters based on feedback from the user or error between predicted and measured outcomes .
KEYWORDS:
Decision-support, neuro-fuzzy, prognosis, telerehabilitation, outcomes prediction
INTRODUCTION
This project builds on the Intelligent Telerehabilitation Assistant (ITA) technology, which was initially motivated by the need for mobile telerehabilitation tools (1, 2). This was based on the recognition that a dynamic modeling framework is needed to help clinical decision-makers impart evidence-based and experience-based knowledge of how human change occurs due to spontaneous recovery and rehabilitation or assistive technology interventions (3). There was also a realization that for an ITA to behave as a helpful mobile assistant for a client, it needs to have context-awareness, and use changes in context (e.g., where a person is) to change the rules governing its behavior. It also would be useful for it to have a predictive capacity. Finally, the marketplace has shown that rule-based fuzzy controllers are robust and effective, and it makes sense to design ITA controllers that could interface to electronic aids to daily living.
As a start, our focus has been on modeling the clinical plan of care. The American Physical Therapy Association (APTA) identifies six elements of patient/client management: Examination, Evaluation, Diagnosis, Prognosis, Intervention and Outcomes (4). According to APTA, prognosis is the determination of the level of optimal improvement that might be attained through intervention and the amount of time required to reach that level. In this context, pro gnosis represents a complex dynamic nonlinear process that involves sets of clinical, experimental, and social factors, and multi-variable interactions between them. This can be clinically challenging: During the early days of either evolving or completed stroke, neither progression nor ultimate outcome can be predicted (5). There is a need for interactive predictive tools that assist with prognosis estimation over time, can be updated based on new information (interventions, outcomes assessments), and have acceptable levels of sensitivity and specificity (3). The initial target application has been for stroke rehabilitative therapy.
METHOD
The first goal is to identify a collection of fuzzy states that can capture changes in key human variables and outcomes of interest that simulate aspects of interest from the real dynamic human system, based on expert rules. The system behavior is a function of both spontaneous recovery mechanisms and a sequence of therapeutic interventions. The user can explore different intervention plans and have the fuzzy expert system provide a prognosis in the form of predicted outcomes, with each outcome presented as a curve that is a function of time. Users can, for instance, determine through heuristic iteration the sequence of interventions (controls) that are predicted to optimize (maximize or minimize) an outcome of interest. As has been seen by the explosion of fuzzy controllers within consumer products, the fuzzy framework also adds robustness.
 |
|---|
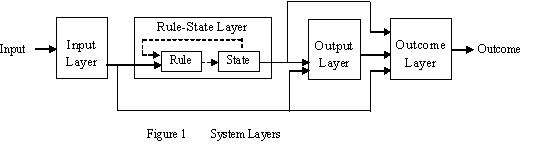
There are five categories of objects in this system (see also Figure 1): input, rules, state, output, and outcome, which are represented by four nuclei (i.e., clusters of artificial neurons, commonly called layers in neural networks). A Graphic User Interface (GUI) for each layer helps facilitate interactive user input of structure and parameters for a given model. By implementing this fuzzy dynamic system using a neural network framework, the infrastructure is in place for subsequent studies of neural learning (e.g., tuning healing dynamics to a specific subject; user preferences).
Input Layer :
There are two kinds of inputs: status data and events. Normally the status data is from the history record and observation. It can be the general patient data, result of diagnostic test, and/or present diagnosis. An event is the occurrence of certain interventions, environmental events or specific tasks. Certain events require user input or confirmation, or degree of agreement.
Rule-State Layer :
Through the interactive GUI, the expert implements fuzzy rules. The expert is required to add temporal dynamics in the implementation of the core logic of the rule. The states are included in this layer, which includes two kinds of neurons:
- Rule-neuron that implements a rule from expert knowledge
- State-neuron that represents a physical/physiological state of patient
The output of a rule-neuron depends on both its input and connections with other rule-neurons that are complementary (excitatory connections) or competitive (inhibitory connections). The logic for rules is normally associated with state, i.e., for each state, find all the factors that may have effect on this state, and then organize those factors into rules. The output of a rule is a function of the input signals and/or states (see Figure 1 ), through a mapping process that implements fuzzy rule operations that include any combination of and and or operators or fuzzy variables. Each rule-neuron connects to a state-neuron (or to a small cluster of neurons providing sub-states). The state of a state-neuron is not only a function of the fuzzy rules, but also of a temporal dynamic process that depends on some time constants.
Output Layer :
Outputs typically perform an action (e.g., prompt user, initiate communication, store data in an electronic record) or provide a prediction of performance (e.g., predict an independence scale such as FIM (Functional Independence Measure) score (6)) that relates to decision-support information for the user. Normally predictive outputs are variables that are measurable and thus are sampled on occasion, and thus any error between the predicted output and the actual output becomes an error signal that could be used to improve the model. The output of a neuron in this layer is a function of the states of the rules and the input events.
Outcome Layer :
Outcomes are defined as scalars or curves that relate to what in engineering optimization is called performance sub-criteria or cost functions, and can be a function of events, fuzzy states, and outputs. Examples of rehabilitative outcomes are numerical representations of terms such as impairment, disability, independence, quality of life, satisfaction, and cost (6).
Parameter Adaptation and Intervention Optimization
Interactive sensitivity analysis is available to assist the expert designer in understanding the sensitivity of behaviors of interest to adjustments in strategic model parameters. The error between a predicted outcome and an actual outcome can be used to tune the model, as long as the user can attribute error to certain parameters that are to be tuned. This is essentially an interactive neuro-fuzzy reinforcement learning approach in which the user functions as the adaptive critic who determines which membership function or rule parameters to adapt (or assign credit), so as to learn to improve its optimal estimate of the prognosis. Ultimately a tuned system could become an interactive decision-support system that helps the practitioner design optimal intervention plans, compare progress to expectations, and gradually tune itself to its consumer .
This system is implemented in C# and designed as a stand-alone package, or to be embedded in web-based mobile ITA modules that include multimedia conferencing and data collection capabilities.
RESULTS AND DISCUSSION
The system framework and GUI interfaces have been field-tested by a group of students in a rehabilitation engineering class, who used the system to develop a range of rehabilitation-related dynamic models, including models in neuro-, orthopedic and cardiopulmonary rehabilitation. This included evaluation of interfaces that are intended to help give users an intuitive understanding of the parameters, for instance the shape of membership functions. The rules and parameters for the stroke rehabilitation project are currently evolving, with clinician input that includes Nicole Sirota, D.O., a fellow on a training grant from the National Institute on Disability and Rehabilitation Research.
Expert knowledge is crucial when establishing the system. The next step of the planned approach is the use a focus group consisting of experts in stroke rehabilitation who use the prototype system and suggest ways to improve it. This will include use of case studies to help articulate rules that capture evidence or expert practice, what the consequences or outcomes of specific courses of action might be, and what impact manipulation of other variables might have on altering outcomes.
ACKNOWLEDGMENTS
The financial support from The Ralph and Marian Falk Medical Trust Foundation and the Rehabilitation Engineering Research Center on Telerehabilitation (U.S. Department of Education, NIDRR #H133A990008) is gratefully acknowledged. All opinions are those of the authors.
REFERENCES
- Wang Y, Winters JM. (2002) Implementation of Multimedia Conferencing and Neurofuzzy Expert Modules in an Intelligent Telerahab Assistant. , Proc. 2 nd EMBS/BMES Conf ., Houston, pp 1863-1864
- Winters JM, Wang Y, Winters JM. (2003). Wearable Sensors and Telerehabilitation, EMBS Magazine , vol 22, 56-65.
- Winters JM (2002). Telerehabilitation Research: Emerging Opportunities, Ann. Rev. Biomed. Engng ., vol. 4, pp. 287-320..
- American Physical Therapy Association (1997), Guide to Physical Therapist Practice , Ch1.
- Tegos TJ, Kalodiki E, Sabetai MM, Nicolaides AN Stroke: pathogenesis, investigations, and prognosis--Part II of III , Angiology. 51(11):885-94, Nov.
- Granger CV, Brownscheidle CM (1995). Outcome measurement in medical rehabilitation , Int J Technol Assess Health Care, vol. 11, pp. 262-268.
Author Contact Information:
Yu Wang,
Department of Biomedical Engineering,
Marquette University,
Milwaukee, WI 53233 USA.
Phone: (414)288-6277,
email: yu.wang@marquette.edu