A New Conceptual Model for Predicting Assistive Technology Use and Impact
ABSTRACT
This article proposes a user-centered conceptual model that predicts AT usage as a function of the perceived relative advantages of AT. Device usage is not modeled as a one-time, all-or-nothing proposition, but as a decision process recurring over time. The influence of parallel interventions is a central consideration that ultimately drives AT use.
Keywords:
outcomes, research, model
BACKGROUND
Predictive models help frame research questions, interpret results, and guide clinical practice. For assistive technology (AT) practitioners and researchers, a valid predictive model would answer essential questions posed by evidence-based practice, e.g. identifying causal relationships between populations of AT users and outcome indicators [1]. Although numerous conceptual models have appeared in the assistive technology (AT) literature [2], none has been shown to predict AT usage [2-4]. In the absence of a valid predictive model, clinicians rely on a process of trial and error to evaluate intervention options [5], which hampers research progress [3]. This article proposes a user-centered conceptual model that predicts AT usage as a function of the perceived relative advantages of AT.
OVERVIEW OF NEW CONCEPTUAL MODEL
Description
 |
|---|
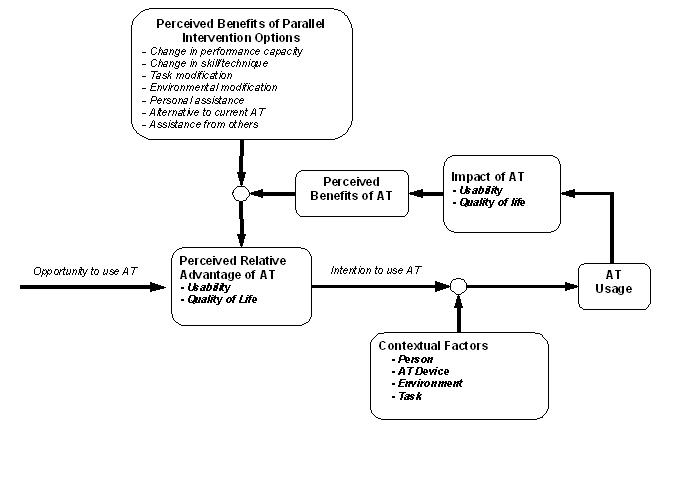
The proposed predictive model (Fig. 1) begins with a person's opportunity to use AT. The individual perceives a relative advantage (or disadvantage) to AT in terms of usability and quality of life impacts, based on prior information regarding the benefits of AT. The perceived relative advantage, as it bears on completion of meaningful tasks, creates an intention to use AT that is subsequently modified by the associated contextual factors: physical and cognitive abilities, motivation; activity demands; intensity of the AT intervention, including characteristics of the device and associated services; and physical environment and social context [4]. The ensuing AT usage patterns (including non-use) engender usability and quality of life impact of AT, e.g., effectiveness, efficiency, satisfaction, and subjective well-being. The perceived benefits (or drawbacks) of AT are then weighed against the perceived benefits of alternative options to AT use, so-called parallel interventions . The comparison between AT and alternative options yields a perception of relative advantage, expressed in terms of usability and quality of life impact, which determines future intentions regarding AT usage.
Conceptual Heritage of the New Model
The salient features of the new model are derived from three perspectives on human behavior: social cognition models, Smith's parallel interventions model, and the Perceived Attributes Theory. Social cognition models assert that the perceived benefits associated with a particular behavior, in this case AT use, are ultimately predictors of the behavior [6]. For our purposes, the theory suggests that perceived impact of AT is influenced by expected benefits of AT use, the perceived effort and costs of AT use, and the perceived consequences of not using AT. Smith [7] identifies six potential categories of parallel intervention that contribute to an individual's activity performance: (a) change in underlying performance capacity, (b) change in technique for performing the task, (c) task modification, (d) environmental modification, (e) personal assistance from others, and (f) use of AT devices and services. Figure 1 depicts the comparison between perceived benefits of AT use and perceived benefits parallel interventions, resulting in the perceived relative advantage of AT use. The Perceived Attributes Theory, a component of Everett Rogers' Diffusion of Innovations model [8], identifies seven factors influencing an individual's choice to adopt a product for his or her own use: (a) relative advantage, (b) compatibility, (c) complexity, (d) trialability, (e) observability, (f) re-invention, and (g) change agent contact [9]. Rogers describes two reasons for discontinued product use: replacement and disenchantment. All nine factors have clear analogues with respect to AT device adoption or rejection [2].
Descriptive Traits
The proposed model does not include detailed descriptions of human, task, and environmental factors. Validation studies will need to account for these factors at levels that are appropriate to each study's context and hypotheses. Related treatment factors (e.g., assessment, training, and maintenance services) also merit examination in order to account for their modifying influences on outcomes.
Implicit Outcome Measures
The principal outcome indicator for the new model is AT usage. Quality of life and usability impacts resulting from AT usage are secondary outcome indicators that subsequently influence future behavioral intentions regarding use of AT and parallel intervention options. Usage is often measured dichotomously in terms of AT "use" and "non-use", or "abandonment". Other dimensions of device usage are meaningful: frequency of use , measurable in uses per day, week, or month; duration of use , measurable in minutes or hours per day; environments of use , e.g., social or community contexts of use; the tasks for which a device is used (e.g., writing reports, entering data, or composing email).
Usability indicators include: device usage, physical and cognitive effort, ease of use, learnability, adjustability of features, hassle, frustration, confusion, fatigue, comfort, pain, independence, level of assistance, stigma or embarrassment, goal attainment, productivity, task completion, time required for task completion, performance, errors, quality of the end product, quality of performance (e.g., technique or skill), participation, relative advantage of AT compared to alternative options, locus of control, being in control, environments of use, reasons for non-use, safety, cost, and user satisfaction.
Quality of life (QOL) impact is perhaps the most important outcome indicator from the AT user's perspective. QOL domains have been variously characterized in terms of standard of living, health-related quality QOL, health status, quality adjusted life years, social relationships, social role performance, and subjective well being [10-11].
Predictive Features
The predictive features of the new model are derived from social cognition models [6], Smith's parallel interventions model [7], and Rogers' Perceived Attributes Theory [8]. As applied here, the perceived value of AT is compared against the perceived value of parallel intervention options, resulting in a perceived relative advantage that predicts AT usage via causal relationships that are modified by human, task, AT, and environmental factors.
Validation
As described extensively elsewhere [12], elements of the model receive substantial support in the AT literature. Research is needed to test the model in its entirety.
Utility for Practitioners, Users, and Developers
The proposed model offers an intuitive schema for AT practitioners, many of whom have been raised in the holistic traditions of occupational therapy or human factors engineering. Consideration of an AT device's perceived value would foster consumer empowerment and guide clinical decision-making, while mitigating the potential to view AT as a false panacea for addressing performance needs. Similarly, product designers would benefit from considering the relative advantages and perceived value that consumers experience during usability testing of new product designs. Practitioners and consumers would find it mutually instructive to discuss the benefits of AT in relation to parallel intervention options at the time of AT assessment, recommendation, and training. Although AT users may not consciously consider parallel intervention trade-offs without prompting, the daily human experience is rife with decision-making processes that require comparison of perceived benefits among competing options.
SUMMARY
The proposed conceptual model does not depict AT usage as a one-time, all-or-nothing proposition. Rather, usage is modeled as a recurring decision process influenced by the utility of parallel interventions. Usage is shown as a proximal influence on AT impact, and AT impact is shown to be a predictor of future use. Further validation will require studies in which sample characteristics and treatment strength [13] are clearly described, so that their influence as outcome modifiers [14] can be interpreted in the context of the model.
REFERENCES
- Holm, M.B. (2000). Our mandate for the new millennium: Evidence-based practice . American Journal of Occupational Therapy, 54, 575-585.
- Lenker, J.A. and V.L. Paquet. A review of conceptual models for assistive technology outcomes research and practice. Assistive Technology . In press.
- Jutai, J.W. (2002). Occupational therapy and assistive technology: The research challenge. The Israel Journal of Occupational Therapy, 11 , E3-E22.
- Fuhrer, M. J., Jutai, J. W., Scherer, M. J., & DeRuyter, F. (2003). A framework for the conceptual modeling of assistive technology device outcomes. Disability & Rehabilitation, 25 (22), 1243-1251.
- Light, J. (1999). Do augmentative and alternative communication interventions really make a difference?: The challenges of efficacy research. Augmentative and Alternative Communication, 15 , 13-24 .
- Armitage, C.J., & Conner, M. (2000). Social cognition models and health behaviour: A structured review. Psychology and Health, 15 , 173-179.
- Smith, R. O. (2002). Assistive technology outcome assessment prototypes: Measuring "INGO" variables of "outcomes". In R. Simpson (Ed.) RESNA 25th Annual Conference Proceedings (pp. 239-241). Washington: RESNA Press.
- Rogers, E.M. (1995). Diffusion of Innovations (4th ed). New York: Simon & Schuster.
- Carr, V. H. (1999). Technology adoption and diffusion . National Library of Medicine, The Collaboratory for High Performance Computing and Communications. Retrieved November 11, 2003, from the World Wide Web: http://collab.nlm.nih.gov/tutorialspublicationsandmaterials/sourcebook/ adoptiondiffusion.html
- Fuhrer, M.J. (2000). Subjectifying quality of life as a medical rehabilitation outcome. Disability & Rehabilitation, 22 , 481-489.
- Gill, T.M., & Feinstein, A.R. (1994). A critical appraisal of the quality of quality-of-life measurements. JAMA, 272 , 24-31.
- Lenker, J.A., & Paquet, V.L. A new conceptual model for assistive technology outcomes research and practice. Assistive Technology, In press.
- Keith, R.A. (1997). Treatment strength in rehabilitation. Archives of Physical Medicine and Rehabilitation, 78 , 1298-1304.
- Baron, R.M., & Kenny, D.A. (1986). The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology, 51, 1173-1182.
Contact:
Jim Lenker,
Department of Rehabilitation Science,
School of Public Health and Health Professions,
University at Buffalo,
14214-3079.
(716) 829-3141, x109;
lenker@buffalo.edu