Pressure Ulcer's Prevention Approach Used the Interpretive Structural Modeling and the Nominal Group Technique
ABSTRACT
The seating clinic at National Rehabilitation Center for Persons with Disablities has a program to prevent repeated pressure ulcers (PU) in persons with spinal cord injury (SCI). For a systematic approach in presenting such a course in consideration of risk factors to patients, Interpretive Structural Modeling (ISM) and the Nominal Group Technique (NGT) were used for analysis of PU factors and course structure.
KEYWORDS
Pressure ulcers ; risk factor; spinal cord injury
BACKGROUND
Many persons with SCI suffer repeated PU and must remain in hospital for long periods of time in Japan. Kitagawa and Kimura reported that 12.2% of 95 patients in one SCI center already had PU and that PU recurred an average of 9 times(1-26 times). Also, they reported that patients with PU had an increased average length of hospital stay and total medical expenses in comparison with patients not having PU (1).
In 2002, the Ministry of Health, Welfare and Labor, Japan, requested hospitals to take actions to prevent PU. These actions would also include prevention of PU in wheelchair-bound patients.
In our center, we developed a seating clinic four years ago. In the clinic, we have a program to prevent repeated PU in persons with SCI. Purpose of the program is devise a course on PU and to teach methods of prevention of PU. We studied a course on PU in 52 persons and half of the persons who received the program were in wheelchairs and the other half not (2)
We used a person-to-person approach in presenting their course according to the individual patient. In contrast to this person-to-person approach, a course based on a systematic approach and risk factors is now recommended. We believe the systematic approach will be more effective in preventing PU.
RESEARCH QUESTION
The objective of this study was to reach a consensus on the complex issues in each group and analyze the structure of the issues using ISM and NGT. The course on PU involves various issues and complex relationships. System engineering, the ISM and NGT, are good methods to facilitate opinions of physical therapist staffs that work in the PU prevention program in the seating clinic and to solve the problem of PU.
METHOD
Interpretive Structural Modeling (ISM)(3)was used as a process that forces participants to focus on the importance of one idea in light of a competing idea. The ISM is an effective methodology for dealing with complex issues. Process of ISM is as follows:
- Organize a team
- Frame a question
- Select some sub factors using NGT.
- Each member writes down within 5 minutes keywords regarding factors within the question.
- All keywords are shown to all members. If some keywords are the same, those key words each count as one.
- Team members discuss keywords and reduce the number of keywords.
- Relationship between each sub factor s.
- Comparison between two keywords.
- Graphic representation and structural modeling
The NGT (Nominal Group Technique) is a technique to identify some sub factors using opinions of team members.
RESULTS
Step 1. Profiles of the four physical therapists who attended the program and take care more than 100 SCI persons are shown in Table 1.
Step 2. Half of the subject matter in the course on PU involves persons in a wheelchair.
The Question is Risk of Pressure ulcers in a wheelchair
Step 3. The keywords include 65 items, including lower sitting balance and misplacing objects on a cushion.
Then, the team discussed the keywords two times and reduced the number from 65 to 13 keywords.
The 13 keywords were:
- Heat and moisture of cushion (HMC) in the summer
- Durability of cushion (DC)
- Education on cushion (EC) and its use
- Selection guidelines for cushion (SGC)
- Carelessness mistake (CM) minimizing THE SORE
- Education on pressure relief (EPR)
- Design of wheelchair for Pressure ulcer prevention (DWPUP)
- Management of daily life presenting risk (MDL)
- Spinal deformity (SD)
- Sitting balance (SB)
- Supply system of wheelchair tilting system (SSWTS)
- Boundary level for push-offs (BLPO)
- Sports (or S)
Step 4. Pairs of keywords, 13*12=156, which represents combinations of all keywords, are compared.
Age (Years old) |
PT Experience(Year) |
Clinic Experience (Year) |
|
|---|---|---|---|
PT |
45 |
22 |
4 |
PT |
40 |
18 |
4 |
PT |
25 |
3 |
2 |
PT+Engineer |
48 |
20 |
4 |
First, for each pair, we decided which is the more significant using consensus by the group. But the structure was very complicated because one keyword does not always represent a clear definition and the numbers of significant pairs were too many (Table 2, 46 circles are more significant.)
Second, each member decided which was more significant of the pair, and then the sum of the decisions would indicate the more significant (Table 2, number shows the sum).
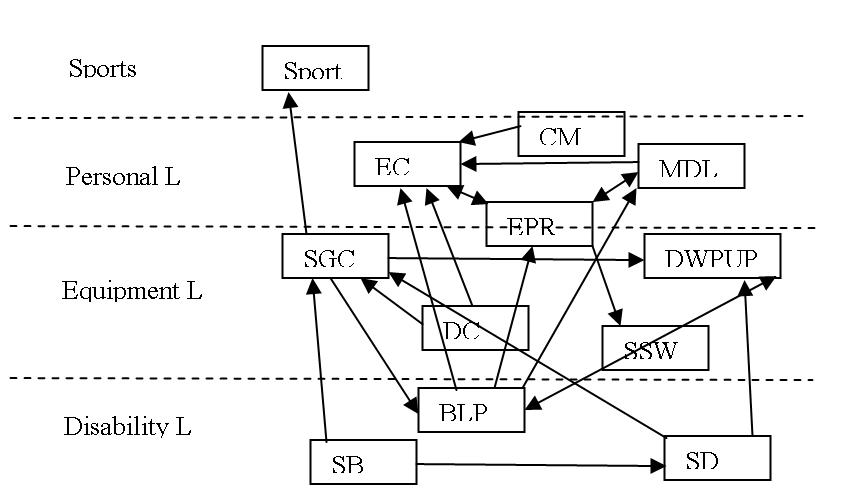
Step 5. Figure 1. Four risk levels for keywords were classified from the structure of the keywords. Sports Level is in sports activity. Personal Level includes education and information for person with SCI. Equipment Level is in performance, selection and provision of a cushion and the wheelchair, including a tilting mechanism. Disability Level is in insufficient ability to push-up due to the degree of disability, age and another disability.
| Solution of | Promotion of | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HMC | DC | EC | SGC | CM | EPR | DWPUP | MDL | SD | SB | SSWTS | BLPU | S | ||
| HMC | O | O | O | O | O | |||||||||
| DC | O6 | 4 | O | |||||||||||
| EC | O | 8 | O | O6 | 6 | |||||||||
| SGC | O | O | O | 4 | O | 4 | 4 | |||||||
| CM | O4 | O | O4 | O | ||||||||||
| EPR | O4 | 4 | O4 | |||||||||||
| DWPUP | O | O | O | O6 | 5 | |||||||||
| MDL | O | O6 | O | O6 | O4 | O | ||||||||
| SD | O5 | O7 | ||||||||||||
| SB | 4 | 4 | ||||||||||||
| SSWTS | O | O8 | ||||||||||||
| BLPU | O4 | O | O | O5 | O4 | 4 | O | |||||||
| S | O | O | O | O | O | O | ||||||||
 |
|---|
DISCUSSION
ISM's weaknesses include: 1) identifies static relationships; 2) is qualitative, not quantitative; and 3) is simplistic and not very powerful. This method makes consensus among our members to be of importance for cushion because there are four keywords for cushion among the 13 keywords. We have a design method for the wheelchair but no cushion selection guide. Now ISOTC173SC1WG11 makes wheelchair seating which includes a tissue integrity management cushion. This standard will be important in resolving cushion problems, make cushion selection guidelines and preventing PU.
The structural models will show that one factor has some sub factors. For example, EC, Education on cushion, includes the content of DC, CM, EPR, MDL and BLPO. Selection guideline of cushion, SGC, includes DC, EC, SD and SB. It is very useful to decide on content using keywords.
In the structural model, the four levels, sports, personal, equipment and disability, show the level of PU risk. Our results are very different from the risk analysis of Byrne and Salzberg including diseases and smoking(4). For example, in sports there is a difference in PU risk between wheelchair marathon and table tennis. We must approach the prevention of PU according to performance of sports.
When we approach the subject of PU prevention to a client, this method based on our experience and discussion will be more systematic than the person-to-person approach. Structural modeling will induce inclusion of a PU course classification of wheelchair for persons with SCI.
REFERENCES
- T Kitagawa and T Kimura. (2002). The Influence of Complications on Rehabilitation of Spinal Cord Injuries; Economical Minus Effects and Physical Disadvantages Caused by Urinary Tract Infection and Decubitus Ulcer,J Nippon Med Sch, 69-3,268-277..
- H Hirose, J Niitsuma, R Iju, Y Iwasaki, H Seki.(2001).Pressure Sore Prevention Program in our Center, The Japan Medical Society of Paraplegia, 14-1,30-31. (Japanese)
- http://www.bsu.edu/classes/flowers2/rlo/tainterpretive.htm
- W Byrne and CA Salzberg.(1996): Major Risk Factors for Pressure ulcers in the spinal cord disabled: a literature Review, Spinal Cord, 34 , 255-263.
Author Contact Information:
Hideyuki Hirose,
National Rehabilitation Center for Persons with Disablities
,
4-1, Namiki,
Tokorozawa, Saitama,359-8555 ,
Tel:-81-42-995-3100,
E-mail:hirose@rehab.go.jp