Wrist Range of Motion & Wheelchair Pushrim Kinetics: Their Impact on Nerve Health
ABSTRACT
Our previous research found that subjects using a greater range of motion (ROM) showed better nerve function than those subjects propelling with a smaller ROM (1). This was opposite of what we expected, therefore we performed this follow up study on wrist ROM and pushrim kinetics. We found a negative correlation between wrist flexion/extension ROM and stroke frequency (r = -0.372, p < 0.05) and resultant force (r = -0.362, p < 0.05). This shows that a larger ROM is associated with decreased force and frequency required to propel the wheelchair at a given speed and explains our previous research, which concluded that an increased range of motion might benefit nerve health.
KEYWORDS:
wheelchair, wrist, kinematics, nerve injury
OBJECTIVE
Manual wheelchair users are commonly diagnosed with carpal tunnel syndrome (CTS) as well as ulnar nerve injury with the prevalence of CTS ranging from 49% to 63%. The highly repetitive task of propelling a wheelchair has been associated with the development of CTS (2,3). The basic cause of CTS is injury to the median nerve. High repetition, high-force actions of the wrist, as well as large joint excursions have been implicated as leading to injury (4). Wheelchair propulsion requires these high-force, high-repetition wrist actions (5). Our previous research analyzed median and ulnar nerve function and their relationship with wrist ROM during wheelchair propulsion and found larger ROM to be correlated with less nerve damage, which was contrary to our hypothesis (1). This study sought to explain these opposing results by comparing wrist ROM with pushrim kinetics. A previous study found that pushrim biomechanics were related to median nerve function. Specifically, larger forces were associated with more median nerve damage (6). We hypothesized that subjects using a larger ROM would use less total force to propel their wheelchair and fewer strokes to maintain a desired speed.
METHODS
Subjects
Thirty-five subjects were recruited for this study. Subjects were between the ages of 18-65. All subjects were required to have a traumatic spinal cord injury at or below the second thoracic vertebrae. The injury must have occurred more than one year before they entered the study. All subjects used a manual wheelchair as their primary means of mobility. No restrictions were place on subject race or gender.
Kinematic & Kinetic Data
The Optotrak was used for the collection of kinematic data. The Optotrak collected data at a rate of 60 Hz. The markers were placed bilaterally on specific bony landmarks of each subject. The SMART Wheel was used for kinetic data collection. The SMART Wheel has a precision of 2 Newtons and a resolution of 0.2 Newtons at a collection rate of 240 Hz. (7) A SMART Wheel was placed on both sides of every subject's wheelchair. The SMART Wheels did not alter the camber, diameter, or tire size of the subject's normal wheels. Once the SMART Wheels were attached, each subject's wheelchair was secured on a dynamometer and subjects were instructed to propel their wheelchair to get acquainted to the dynamometer. Subjects were then asked to propel at two different speeds: 0.9 m/s (2mph) and 1.8 m/s (4mph). Once the subject reached the desired steady state speed, both kinematic and kinetic data were collected for 20 seconds. Subjects were given approximately one minute of rest between trials.
Data Analysis
The kinematic data was analyzed as described previously (1). Briefly, using marker data, a local coordinate system for the wrist was developed. The first axis was defined as a line pointing from the midpoint between the radial and ulnar styloids to the third metacarpophalangeal joint. The second axis was defined as perpendicular to axis one and pointed out of the back of the hand/wrist. The third axis was perpendicular to the plane formed by the first two axes, and pointed from the midpoint of the wrist through the radial styloid. By determining the rotations about these axes, ROM variables were developed. The SMART Wheel was used to determine the forces and moments applied to the pushrim as well as the stroke frequency. Specifically, we analyzed the total force applied to the pushrim, and the stroke cadence (5) . From the SMART Wheel data we determined the resultant force by averaging the peak total force across the strokes of a trial. Correlations between left and right sides were found to be significant (r > 0.941, p < 0.01), therefore the left and right side data were averaged together to develop one force variable and one frequency variable for each speed. Correlations between the two speeds were analyzed and found to be significant (r > 0.702, p < 0.01), therefore the speed data were averaged together. The final result was one force variable and one frequency variable representing left and right sides and both speeds. All correlations were done using SPSS.
RESULTS
Subjects
 |
Thirty-five subjects, eight females and twenty-seven males, were recruited for this study. Subjects were between the ages of 18-65, with an average age of 38.9 years. The average time from injury date to test date was 12.2 years (range 1.4 30.4). Subjects' average weight was 77.5 (±16.8) Kg and height was 176 (± 9.7) cm.
Wrist kinematics and Pushrim Kinetics
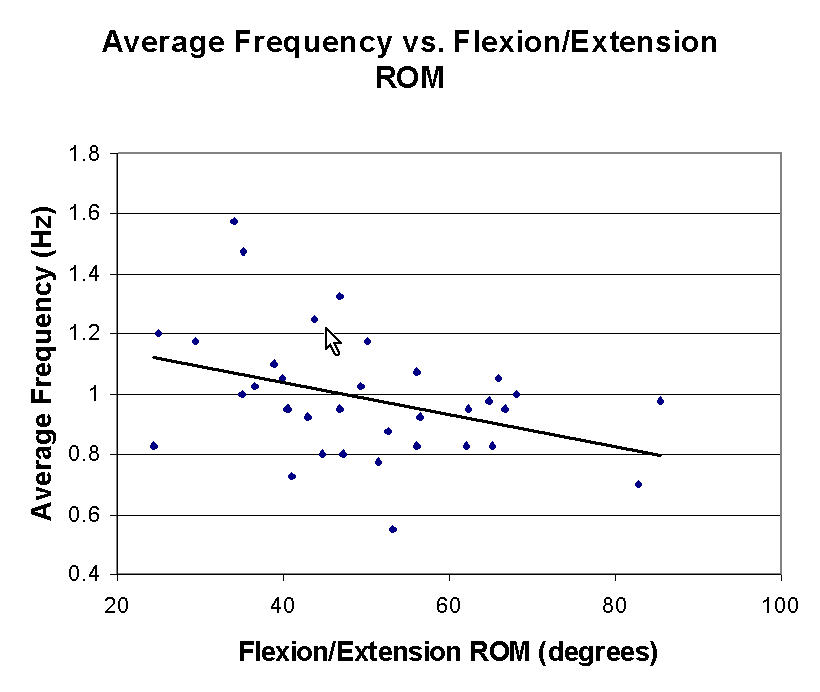
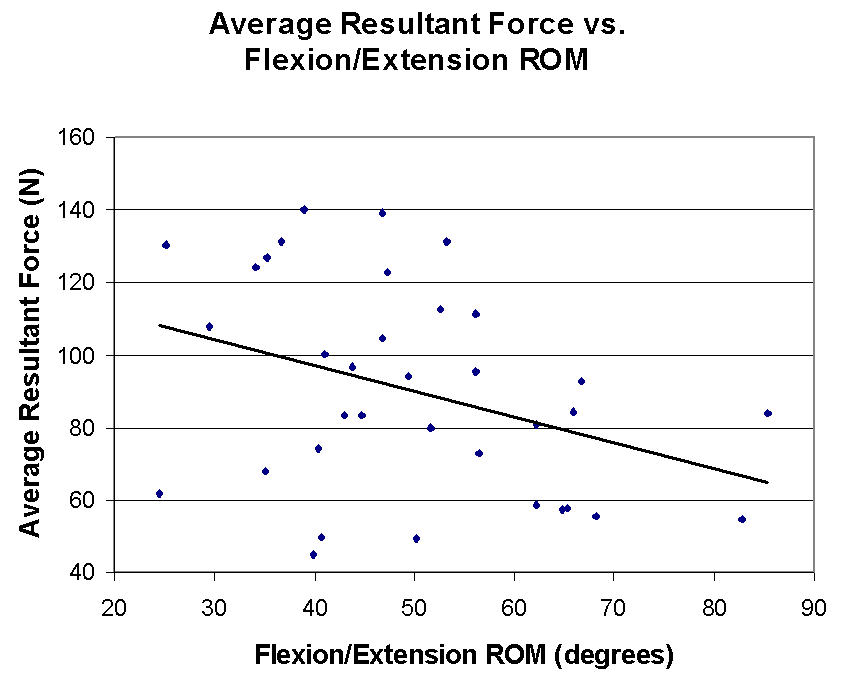
The mean resultant force was 90.3 N and the mean stroke frequency was 1.0 Hz. We found significant negative correlations between wrist flexion/extension range of motion and: stroke frequency (r = -0.372, p < 0.05, see Figure 1) and resultant force (r = -0.362, p < 0.05, see Figure 2).
 |
DISCUSSION
Previous research has stated that high-repetition, high-force actions, as well as large joint excursions at the wrist may be detrimental to nerve health (4). Regarding wrist ROM, we found subjects using a larger ROM to propel their wheelchair were not at a higher risk of damaging their median and ulnar nerves. In fact, large excursions were correlated with less injury (1). This study found that wrist ROM was significantly related to force applied to the pushrim and frequency of propulsion. We found that people propelling with a larger ROM pushed at a slower frequency, or contacted the pushrim less often, and used less force to propel their wheelchair at a given speed. Previous studies have found that persons propelling their wheelchair with longer, smoother strokes may be less likely to injure the median nerve (6,8). A longer, smoother stroke, in most cases, means a greater range of motion over the stroke. This study supports these previous findings since subjects using a greater range of motion were found to have better median and ulnar nerve performance as well as decreased force applied to the pushrim and decreased stroke frequency. When performing a high-repetition, high-force task such as wheelchair propulsion, it appears that using a larger range of motion is actually beneficial as it is associated with decreased forces and frequency necessary for propulsion. This may also have implications in other areas of ergonomics research. When performing highly repetitive tasks using the hands and wrists, if possible, it may be advantageous to use a larger ROM if decreased forces and frequency can be achieved.
CONCLUSION
This study showed that propelling with a larger ROM decreased both the force applied to the pushrim and the number of strokes necessary to maintain a given speed. Therefore, manual wheelchair users should consider using a long, smooth stroke, which implies a larger ROM, to propel their wheelchair since this may reduce damage to the median and ulnar nerves. A larger study population would help to support these findings. Further analysis could be done to investigate the benefits of training people proper propulsion techniques.
REFERENCES
- Impink B, Boninger M, Cooper R, Koontz A. Median & Ulnar Nerve Function Related to Wrist Range of Motion During Wheelchair Propulsion. Proceedings of the RESNA 26 th International Conference on Technology & Disability ; 2003 June19-23, Atlanta (GA). RESNA Press; 2003:CD-ROM.
- Aljure J, Eltorai I, Bradley W, Lin J, & Johnson B. Carpal tunnel syndrome in paraplegic patients. Paraplegia , 1985; 23: 182-186.
- Gellman H, Chandler D, Petrasek J, Sie I, Adkins R, & Waters R. Carpal tunnel syndrome in paraplegic patients. The Journal of Bone and Joint Surgery , 1988; 70-A (4): 517-519.
- Szabo R. Carpal tunnel syndrome as a repetitive motion disorder. Clinical Orthopaedics and Related Research , 1998; 351: 78-89.
- Boninger M, Cooper R, Roberston R, & Shimada S. 3-D pushrim forces during two speeds of wheelchair propulsion. Am J Phys Med Rehabil , 1997; 76: 420-26.
- Boninger M, Cooper R, Baldwin M, Shimada S, & Koontz A. Wheelchair Pushrim Kinetics: Body Weight and Median Nerve Function. Arch Phys Med Rehabil , 1999; 80(8): 910-15.
- Cooper, R. A., Robertson, R. N., VanSickle, D. P., Boninger, M. L., Shimada, S. D., Kinetics, Propulsion, Upper limb biomechanics, and Wheelchair. Methods for Determining Three-Dimensional Wheelchair Pushrim Forces and Moments - A Technical Note. Journal of Rehabilitation Research & Development 1997; 34(2): 162-70.
- Boninger M, Souza A, Cooper R, Fitzgerald S, Koontz A, & Fay B. Propulsion patterns and pushrim biomechanics in manual wheelchair propulsion. Arch Phys Med Rehabil , 2002; 83(5): 718-723.
ACKNOWLEDGEMENTS
This study was supported by the Department of Veterans Affairs (CULPSCI: #CDF84:133A and VACULPSCI: #B3057T)
Author Contact Information:
Bradley Impink
Human Engineering Research Laboratories
7180 Highland Drive
Building 4, 2nd Floor, East Wing, 151R-1
Pittsburgh, PA 15206
Phone: 412-365-4850
E-mail: bgist@pitt.edu