Effect of a Pushrim Activated Power Assist Wheelchair on the Functional Capabilities of Individuals with Tetraplegia
ABSTRACT
The purpose of this study was to test differences between a pushrim activated power-assisted wheelchair (PAPAW) and a traditional manual wheelchair for individuals with cervical level spinal cord injuries (tetraplegia) while performing common driving activities. Fifteen fulltime manual wheelchair users propelled both their own manual wheelchairs and a PAPAW three times over an activities of daily living (ADL) course. Analyzed variables included: the time to complete the course, mean heart rate, and participant responses to a visual analog scale survey. Participants showed a significant (p < 0.05) decrease in mean heart rate and rated ten out of the eighteen obstacles in the ADL course to be significantly easier to complete when using the PAPAW. For individuals with tetraplegia, PAPAWs have the potential to improve the functional capabilities during certain ADLs, especially when propelling up ramps, over uneven surfaces, thick carpet, and for extended distances.
KEYWORDS:
Activities of daily living; tetraplegia; power assist wheelchairs
BACKGROUND
Due to reduced physical capacity and upper extremity muscle weakness, manual wheelchair users (MWUs) with cervical level spinal cord injuries (tetraplegia) often find it difficult to independently complete activities of daily living (ADLs). Furthermore, when using a manual wheelchair as one's primary means of mobility, performing necessary activities of daily living can put significant stresses on the upper extremities. It is therefore common for MWUs to experience upper extremity pain and injuries. In a cross sectional survey study of 192 MWUs, Curtis noted that 78% of individuals with tetraplegia reported having some form of shoulder pain since becoming a MWU. (1) This was a significantly higher reported incidence than those with paraplegia.
MWUs with tetraplegia are typically less efficient when propelling than MWUs with paraplegia. With values of gross mechanical efficiency rarely exceeding 10%, alternative methods of manual wheelchair mobility have been proposed. (2) While alternative, more efficient devices such as crank-propelled and lever-propelled wheelchairs have been developed, they are typically more useful for outdoor mobility and have fallen short in presenting feasible and commercially appealing solutions. Pushrim Activated Power Assist Wheelchairs (PAPAWs) offer an alternative between manual wheelchairs, lever-drive systems, and powered mobility devices. These devices are typically manual wheelchairs with a motor linked to the pushrim in each rear hub, where the user's manual pushrim input is supplemented proportionally by the motor.
Very few studies have been performed that assess the functional capabilities of MWUs when using a PAPAW to complete ADLs. Cooper et. al. tested MWUs when using a PAPAW over an ADL driving course. (3) However, the participants included in this study were individuals with paraplegia, and the tasks included in the study were limited. Best et. al. compared a PAPAW to a manual wheelchair using the Wheelchair Skills Test. (4) Though there was positive feedback from individuals when using the PAPAW, this was a pilot study, and the participants used in the study had no disability. No study to date has been conducted that focuses on ADL task completion of MWUs with tetraplegia, a population who may significantly benefit from PAPAWs.
RESEARCH QUESTION
The purpose of this study was to compare the functional differences of MWUs with tetraplegia when propelling a PAPAW and their own manual wheelchair over an ADL driving course. The ADL course was constructed to include obstacles and tasks that that are typically encountered by MWUs.
METHODOLOGY
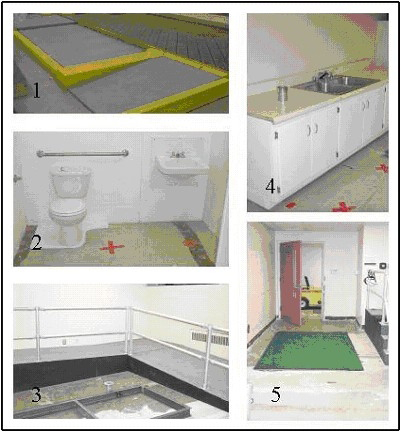
This study received prior approval by the appropriate human studies institutional review boards. Each participant was provided with information about the safety and intent of the tests, and signed informed consent was obtained prior to any testing. Fifteen fulltime MWUs with tetraplegia propelled both their own manual wheelchair and a PAPAW three times (six total trials) over an ADL simulation course. The protocol and layout of the course is similar to that described by DiGiovine et. al. ; however, more obstacles have been added. (5) The course was constructed indoors on a tile floor and consisted of eighteen obstacles. Table 1 lists the eighteen obstacles, and Photo 1 shows a picture of some obstacles.
Propelling down a 61 meter tiled hallway |
Opening and going through a door with an accessible handle |
Propelling across a 2.4 meter strip of high pile carpet |
Propelling across a 2.4 meter dimple strip (guide strip for individuals with visual impairments.) |
Propelling up and down a 4 degree sloped ramp that was 6.7 meters long |
Propelling over a sinusoidal bump that was 50 mm high (simulating a speed bump) |
Propelling up a 1.2 meter long , 7.3 degree curb cut |
Propelling up and down a 5.1 centimeter high curb |
Propelling over a door threshold |
Propelling across a deck surface |
Maneuvering through a tight bathroom setup (toilet, sink and bathtub) |
Turning on a kitchen faucet |
Picking up a can of soup and placing it in a different location |
Maneuvering into a simulated bus docking space (0.76 meters x 1.2 meters) |
 |
|---|
Participants were instructed to complete the course at a comfortable pace (i.e. freely chosen speed). A spotter followed each participant throughout the course and provided assistance when requested by the participant. A second investigator videotaped the participants throughout the trials to monitor data collection, and a third investigator observed each the participant and rated their ability to complete each obstacle. Time to complete the course and heart rate were recorded continuously during each trial. The PAPAW available for this study was a Yamaha JWII mounted to a Quickie 2 folding frame manual wheelchair. PAPAWs were selected to match each participant's own wheelchair seat dimensions.
After the first, third, fourth and sixth trial, participants were asked to fill out a portion of the survey questioning certain aspects of the wheelchair or the ADL driving course. The survey consisted of three parts: questions pertaining to the difficulty of completing the obstacles, questions pertaining to the ergonomics of the wheelchairs, and questions specifically related to the PAPAW. Statistics performed on the collected data included: descriptive statistics, a within-test repeated measures, paired sample t-tests, and a mixed model analysis of variance (ANOVA). A repeated measures test was used to ensure that differences observed in completing the obstacles was not occurring due to a learning effect of the ADL course, but because of differences when propelling the two different wheelchairs. A mixed model ANOVA was performed because it allowed for comparison between the two wheelchairs, even though the same participant performed the testing of the wheelchairs.
RESULTS
The participant demographics included: 11 males and 4 females, mean age 36.0 years (SD 8.3), mean height 178.1 cm (SD 12.3), mean weight 77.7 kg (SD 20.9), and mean years post injury 11.8 (SD 8.1). Tables 2 and 3 show the participants' ratings for completing each obstacle when using each wheelchair and responses to the ergonomic questions, respectively.
Obstacle |
First Trial |
Third Trial |
||
|---|---|---|---|---|
Own |
PAPAW |
Own |
PAPAW |
|
1. Hallway |
1.4 ± 1.8 |
0.6 ± 0.7 |
1.6 ± 2.0 |
0.4 ± 0.3 |
2. Door |
2.1 ± 2.0 |
1.6 ± 1.1 |
1.8 ± 2.1 |
1.0 ± 0.7 |
3. Carpet |
4.2 ± 2.2 |
1.0 ± 1.1 |
3.5 ± 2.8 |
0.7 ± 0.7 |
4. Dimple strips |
2.6 ± 2.1 |
0.8 ± 0.8 |
2.1 ± 1.7 |
0.6 ± 0.6 |
5. Up the ramp |
5.2 ± 2.7 |
1.5 ± 0.9 |
5.2 ± 3.0 |
0.9 ± 0.7 |
6. Down the ramp |
2.0 ± 2.5 |
1.2 ± 0.9 |
1.7 ± 2.2 |
0.8 ± 1.0 |
7. Speed bump |
3.3 ± 2.4 |
2.0 ± 1.2 |
3.0 ± 2.3 |
1.1 ± 0.9 |
8. Curb cut (up) |
5.5 ± 3.1 |
2.1 ± 1.6 |
5.2 ± 3.1 |
1.1 ± 0.7 |
9. 2 Curb (down) |
2.2 ± 2.1 |
1.8 ± 1.4 |
2.0 ± 1.7 |
1.1 ± 1.0 |
10. 2 Curb (up) |
5.3 ± 3.0 |
3.9 ± 2.8 |
5.5 ± 3.3 |
3.6 ± 3.0 |
11. Door threshold |
2.6 ± 2.4 |
1.4 ± 1.9 |
2.7 ± 2.5 |
0.7 ± 0.7 |
12. Deck surface |
1.9 ± 1.7 |
0.8 ± 0.7 |
1.7 ± 1.7 |
0.5 ± 0.4 |
13. Toilet |
1.7 ± 1.5 |
1.1 ± 0.9 |
1.5 ± 1.6 |
0.6 ± 0.5 |
14. Bathroom sink |
1.6 ± 1.5 |
1.3 ± 1.0 |
1.6 ± 1.8 |
0.6 ± 0.5 |
15. Bathtub |
1.7 ± 1.6 |
1.4 ± 1.2 |
1.6 ± 1.7 |
1.1 ± 1.2 |
16. Kitchen faucet |
1.6 ± 1.5 |
1.2 ± 1.0 |
1.7 ± 1.7 |
0.6 ± 0.6 |
17. Kitchen counter (can) |
2.1 ± 1.7 |
1.5 ± 1.2 |
1.9 ± 1.7 |
0.9 ± 1.3 |
18. Bus space |
1.6 ± 1.6 |
1.8 ± 1.7 |
1.6 ± 1.7 |
1.1 ± 1.3 |
Third Trial |
||
|---|---|---|
Own |
PAPAW |
|
1. How supported and stable did you feel? |
7.2 ± 1.9 |
6.8 ± 2.2 |
2. How easy was it to propel the wheelchair? |
4.0 ± 2.6 |
1.3 ± 1.9 |
3. How easy was it to maneuver the wheelchair? |
3.6 ± 2.7 |
2.2 ± 1.8 |
4. How easy was it to control the wheelchair? |
3.6 ± 2.6 |
3.0 ± 2.0 |
5. How comfortable was your hand on the pushrim? |
5.8 ± 2.9 |
7.9 ± 1.6 |
6. How would you rate the overall ride comfort? |
6.6 ± 2.1 |
7.5 ± 1.2 |
7. Rank this wheelchair based on looks. |
7.1 ± 2.4 |
6.4 ± 2.0 |
After the third trial with each wheelchair, participants rated ten obstacles to be significantly easier (p < 0.05) to complete when using the PAPAW. When comparing the PAPAW to itself, between the first and third trial, users rated eight obstacles to be significantly easier to complete: carpet, up ramp, bump, curb cut, toilet, bathroom sink, turning on the kitchen faucet, bus docking space. In response to ergonomic questions, after the third trial, participants reported that the PAPAW was significantly easier to propel and the pushrim was more comfortable than their own manual wheelchair. Additionally, participants needed assistance in completing tasks a total of 35 times with their own wheelchair and 14 times when using the PAPAW, though these numbers were not significantly different (p > 0.05). For all three trials, mean heart rate was significantly lower when using the PAPAW when compared to the participant's own manual wheelchair. Though slightly lower with the PAPAW, the mean time to complete the course was not significantly different between the two wheelchairs.
DISCUSSION
Following a similar study, Cooper suggested that future ADL lab testing with PAPAWs should include individuals with impaired upper extremities, more difficult tasks, and an older population of participants. (3) This was primarily suggested because, in the previous study, participants were individuals with paraplegia, and there were no significant differences between PAPAWs and participants' own manual wheelchairs for the majority of the variables tested. In the current study, more tasks were included, and the participants selected had impaired upper extremities, since they had tetraplegia. Results observed here were consistent to Cooper's suggestion that a population group with impaired upper extremities would prefer the PAPAW to their own manual wheelchair. By the third trial, participants rated 10 of the 18 obstacles significantly easier to complete when using the PAPAW.
Interestingly, results from the survey suggested a short learning curve when using the PAPAW, since participants rated eight obstacles to be significantly easier to complete from the first to the third trial when using the device. Three of these tasks can be construed as maneuvering in tight areas: two bathroom tasks, the toilet and the sink, and maneuvering into the bus-docking situation. This revealed that the users were becoming more comfortable maneuvering the PAPAW in tight spaces, and after only using it for a few minutes. It was encouraging to note that participants were able to complete the ADL course in the same amount of time between the two wheelchairs, but maintained a lower heart rate when using the PAPAW. Conserving energy during routine tasks, such as propelling uphill or across a carpeted hallway, might allow a MWU with tetraplegia to maintain function while performing other necessary activities, such as transferring to a different surface. The higher rating that the PAPAW received for the ease of propulsion question is intuitive, given the assistance that the wheels provide. The higher level of pushrim comfort indicated by the participants could possibly be attributed to participants exerting less force on the pushrims when propelling the PAPAWs. Results of the repeated measures statistical testing showed that there were no significant differences due to participants learning the ADL course. From this, combined with the results of the mixed model ANOVA, we concluded that propelling the PAPAW was the cause of observed differences in dependent variables.
Limitations of the study included a male-biased population and a relatively young age of participants. The young age of participants can likely be attributed to MWUs with tetraplegia transitioning to powered mobility devices as they get older. Additionally, the tasks that were included in this testing are not all inclusive for obstacles that MWUs face on a daily basis. ADL task completion is not the only factor to consider when addressing one's overall seating and mobility needs. PAPAWs should be recommended when users can safely and effectively propel them throughout all daily activities and obstacles. While the results of this study yielded positive feedback from the participants when using the PAPAW, a more thorough test of the device's effectiveness would be a home evaluation. Future studies with this device should focus on the ability of MWUs with tetraplegia to perform necessary activities of daily living within their home environment and community.
REFERENCES
- Curtis KA, Drysdale GA, Lanza D, Kolber M, Vitolo RS, West R. Shoulder pain in wheelchair users with tetraplegia and paraplegia. Arch Phys Med Rehabil 1999; 80(4):453-457.
- van der Woude LHV, Hendrich KM, Veeger HE, van Ingen Schenau GJ, Rozendal RH, de Groot G. Manual wheelchair propulsion: Effects of power output on physiology and technique. Med Sci Sports Exerc 1988; 20:70-78.
- Cooper RA, Fitzgerald SG, Boninger ML, Prins K, Rentschler AJ, Arva J. Evaluation of a pushrim-activated, power-assisted wheelchair. Arch Phys Med Rehabil 2001; 82(5):702-708.
- Best KL, Kirby RL, Smith C. Comparison of a pushrim activated power assist wheelchair and a manual wheelchair on the wheelchair skills test. Conference Proceedings of the 26 th International RESNA Conference 2003; 26: Papers\SM\Best_SM.htm.
- DiGiovine MM, Cooper RA, Boninger ML, Lawrence B, VanSickle DP, Rentschler AJ. User assessment of manual wheelchair ride comfort and ergonomics. Arch Phys Med Rehabil 2000; 81(4):490-494.
ACKNOWLEDGMENTS
We would like to acknowledge Yamaha Motor Corporations, USA for providing the JWII hubs used in this study. Additional funding was provided by the National Institute for Disability and Rehabilitation Research, SCI Model Systems Program (H133N000019).
David Algood,
Center of Excellence for Wheelchairs & Related Technologies,
7180 Highland Drive, 151R-1,
Pittsburgh, PA 15206,
(412) 365-4850,
(412) 365-4858
(fax),
algoodd@herlpitt.org