Walker Monitor
Nancy Du and Shawn George
Department of Biomedical Engineering
University of North Carolina at Chapel Hill
ABSTRACT
Users of rolling walkers, who have Parkinson's disease, sometimes experience “freezing of gait” episodes in which a loss of balance causes serious injury when operating a walker. Inability to break the freeze and the consequent “forward-leaning” posture puts users in danger of falls as the walker rolls away. Visual stimuli, such as a laser line that cues the user to initiate a step, have proved successful in aiding to break a freeze. Current products that use this approach require the user to activate the cue, which many individuals with Parkinson’s disease are unable to do. We developed a device that constantly monitors the user’s position behind the walker, and automatically activates visual and vibrational stimuli to help the user break a freeze. Additionally, our device can prompt the user to maintain correct posture and position.
KEYWORDS:
Parkinson’s, freezing, laser cue, walker monitor
BACKGROUND
Parkinson’s disease (PD), a disorder affecting the nervous system, occurs in as many as one million Americans in the US, or every 1 in 272 people [1]. Prevalent in these diagnosed individuals is the onset of freezing of gait (FOG), which occurs in nearly 26% of patients in the early stages of PD, in addition to those in the more advanced stages. The duration of the freezing episode can range from seconds to a matter of minutes [2]. Individuals that experience this type of motor disability often use a rolling walker to assist in their movement. However, safety problems can result when the user freezes, as a prolonged loss of balance leads to falls, resulting in serious injury or even death.
In several different studies, it has been shown that a laser or visual cue is enough to liberate an individual with PD from their freezing episode [2,3]. Several commercially available devices use the laser technology to unfreeze patients, such as the U-Step Walker (In-Step Mobility Products Corp., Skokie IL), which allows the user to push a button to activate a laser mounted on the walker. However, the user must remember to activate the visual cue. PD individuals often experience memory trouble in the more advanced stages of the disease. As a result, voluntary activation of the cues is a considerable difficulty for them as noted with the U-Step Walker.
The goal of this project was to build a device that would detect when an individual with PD, using a rolling walker, was approaching a freezing event. The device would then automatically activate a visual cue (laser) and vibrational stimuli to aid in breaking the freeze. Using the distance between the patient’s torso and walker frame as an indicator of freezing, the device would activate both visual and vibrational cues when this distance became larger than a threshold. This threshold can be adjusted by the clinician according to the needs of the patient. The combination of a laser light shone horizontally in front of the patient’s feet and vibrational motors mounted under the patient’s palms would break the patient’s freeze by prompting him/her to take a step. In addition, the therapist would be able to adjust the distance threshold, allowing for the device to be used by many patients with distinct gait patterns.
DESIGN AND DEVELOPMENT
Overall Device Operation – Freezing of Gait Detection and Activation of External Cues
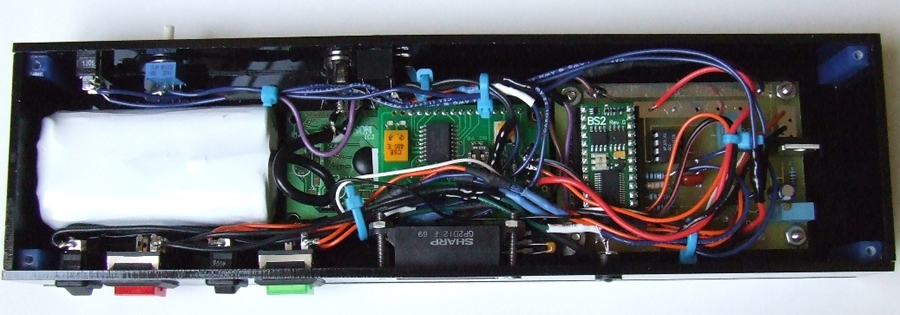 Figure 1 (Click for larger view)
Figure 1 (Click for larger view) Detecting freezing episodes was first determined in terms of quantitative parameters. As observed by physical therapist Linda Cates, the most common characteristic is for patient’s step length to shorten and while the upper body momentum pushes the walker out ahead. Hence, the distance between the patient’s torso and the front of their walker is a good indication of whether or not the individual is in danger of freezing.
A Sharp GP2D12 infrared distance sensor, with the ability to measure from 10-80cm at an accuracy of ±1 cm, continuously measures the distance between the torso and front of the walker and outputs this to a Basic Stamp 2 (BS2) microcontroller chip (Parallax, Inc., Rocklin CA). This distance is compared every 50ms to a “threshold” distance, which is set by the clinician and represents the upper limit of the “safe-zone.” When the measured distance exceeds the threshold, it is highly probable that the patient has frozen and/or is dangerously far away from the walker. The BS2 then activates external cues to remind the user to take a step closer, thus aiding the patient to break a freeze and regain proper position behind the walker.
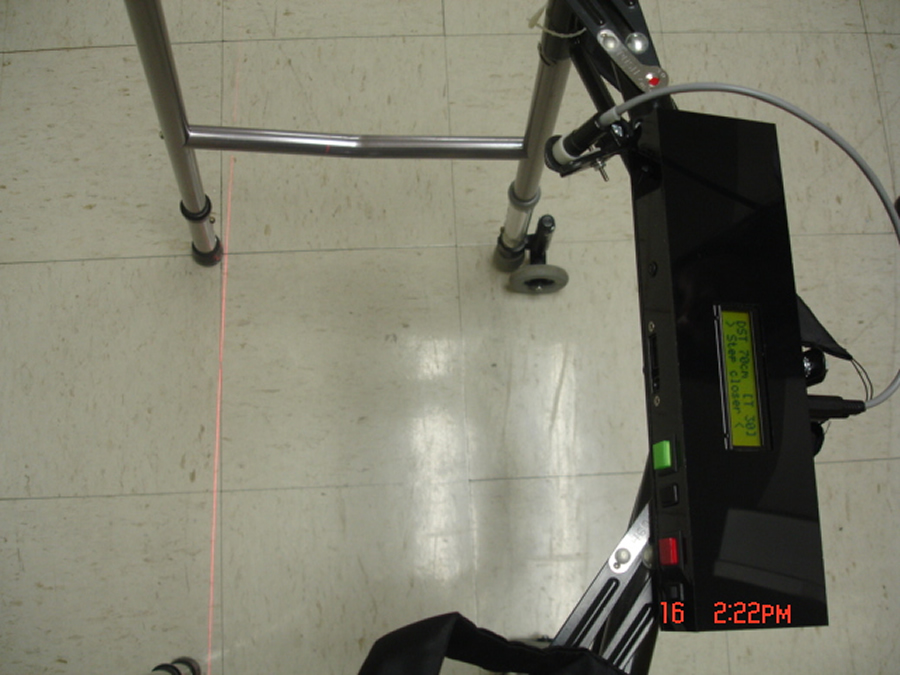 Figure 2. (Click for larger view)
Figure 2. (Click for larger view) One of the external cues is a horizontal laser light beamed on the ground in front of the patient’s feet to remind them to take a step. In addition, vibrating (pager) motors, sheathed in pads attached to the handles of the walker, are also used. This allows the patient to feel a tactile prompt when they should be taking a step, which is a more comfortable alternative for patients who prefer to focus their gaze on the path ahead instead of at the ground.
User Interface and Aesthetics
 Figure 3. (Click for larger view)
Figure 3. (Click for larger view) The clinician or user may set the threshold distance on the device by turning a knob attached to a potentiometer. The threshold distance (in cm) can be read on the LCD display of the device. The LCD also displays the distance being read from the distance sensor and instructs the user to “move away” when they are too close and to “step closer” when they are starting to get too far. Switches allow the user to choose between the laser cue and/or vibratory cue, in case one of the cues works better than the other. Diagnostic switches are used for testing and calibration of the laser and the motors, which allows the therapist to adjust the laser light position accordingly to the patient, and allows the patient to initially gain a sense of what the vibrational motors feel like. All components, except for the laser, were enclosed in a low-profile custom built box which mounts quickly and securely to the walker using bicycle light mounts.
 Figure 4. (Click for larger view)
Figure 4. (Click for larger view) The device has been designed to remain on continually. This was done to ensure that the user would not inadvertently forget to turn the device on. When the user steps away from the device, the walker monitor enters a low power “sleep” mode. When in sleep mode, the device will briefly wake up and read the sensor every four seconds to see if there is an individual in front of the device. When a patient is detected in front of the walker again, the device will turn return to operational mode, scanning every 50ms. This energy efficient function enables a battery life of more than three days when fully charged. A rechargeable, 7.4V Lithium-ion battery is used to power the device, and can be recharged by plugging in a detachable battery charger which also disconnects the main circuit from the battery during charging. A ‘low battery’ LED prevents from over-discharge of the battery, reminding the user to plug in the charger.
EVALUATION AND DISCUSSION
 Figure 5. (Click for larger view)
Figure 5. (Click for larger view) A preliminary evaluation of the device was done with two individuals with PD. Their responses were overwhelmingly positive and they found that the device to helped them maintain proper position behind the rolling walker. Observation by the physical therapist confirmed that the external cues did in fact improve overall posture, and that the vibration motors provided a discreet yet useful reminder to regain proper distance behind the walker.
In addition, our therapist believes that our device could help users of rolling walkers on a larger scale. Elderly individuals who use rolling walkers tend to ‘drift’ from their walker and often require constant oversight by their therapist, and our device serves as a preventive measure to remind the user to step forward and regain proper position behind their walker. The vibrational cue we additionally provided allowed the user to focus their gaze ahead without having to look at the floor for a laser light.
SUMMARY
All aspects of the device work as expected. The infrared distance sensor provides accurate and reliable distance measurements, and the vibration motors provides additional, discreet stimuli. The device can be retrofitted to any rolling walker, and the position of the sensor and laser can be independently adjusted to suit any user.
ACKNOWLEDGEMENTS
This project was funded by the NSF grant BES-0453339. The authors would like to thank Richard Goldberg, Kevin Caves and PT Linda Cates for their considerable assistance with the development and design of the device. A special thanks to Bob Dennis and Lauren Woods, who helped with several revisions of the construction and overall design of the casing.
Author Contact Information:
Nancy Du
700 Bolinwood Drive, Apt. # 40B
Chapel Hill, NC 27514
Cell #: 910-352-6891
EMAIL: dulittle@email.unc.edu
REFERENCES
- Statistics about Parkinson's Disease (n.d.). Retrieved April 15, 2007, from http://www.wrongdiagnosis.com/p/parkinsons_disease/stats.htm
- Laser Pointer Helps Parkinson's Patients Take Next Step (1999, April 22). Retrieved April 10, 2007, from http://www.sciencedaily.com/releases/1999/04/990422055736.htm
- Kompoliti, K., & Goetz, C. G. (2000). "On" Freezing in Parkinson's Disease: Resistance to Visual Cue Walking Devices [Electronic version]. Movement Disorders, 15(2), 309-312. from Wiley InterScience.