Ergonomic Redesign of Elliptical Trainer to Promote Greater Safety, Comfort and Usability
1 Institute for Rehabilitation Science and Engineering, Madonna Rehabilitation Hospital
2 Creighton University
3 University of Nebraska-Lincoln
ABSTRACT
Regaining or retaining walking ability and improving cardiovascular fitness are central goals for many individuals living with chronic conditions and physical disabilities. This presentation highlights ergonomic findings from the second year of a project aimed at developing ICARE, an affordable Intelligently Controlled Assistive Rehabilitation Elliptical trainer and therapeutic program to help individuals with disabilities regain walking ability and physical fitness in healthcare settings and community based fitness facilities. The impact of seven elliptical trainer modifications on safety, comfort, likelihood of achieving a good workout, and overall usability was evaluated by 20 individuals, and findings are summarized.
Keywords:
exercise, physical disability, walking
BACKGROUND
Physical activity is essential to promoting health and improving function,[(1), (6), (7), (11), (14)] yet many individuals with disabilities face barriers to maintaining a physically active lifestyle. [(6), (13)] Additionally, for those seeking to regain or retain walking capacity, the ability to practice independently a task that simulates gait and enables the mass repetition thought to be essential for long-term learning, can be difficult when weakness, numbness, and coordination problems are present. Resources often available during formal rehabilitation, such as specialized equipment and extensive hands-on assistance from therapists, are seldom available in the community. For example, the expense of robotic devices available in select rehabilitation settings and research centers (i.e., ~ $275,000 for the Lokomat), prohibits widespread use in fitness facilities or homes. Likewise, the need for one or two clinicians to lift and advance a client’s legs during partial body weight support treadmill training,[(5), (8), (10)] reduces feasibility of using this technology in non-therapeutic settings. This is concerning, as many individuals living with conditions such as a stroke, brain injury, incomplete spinal cord injury, multiple sclerosis, cerebral palsy or amputation would benefit from the opportunity to continue working on improving cardiovascular fitness and walking.
To address the need for an inexpensive and accessible tool that could be used to help individuals with physical disabilities improve walking function and cardiovascular fitness, our team pursued redesigning an elliptical trainer (also called a cross-trainer) to improve access, comfort and usability. The similarity to walking of movement patterns and muscle demands while exercising on an elliptical trainer that we documented in our earlier work,[(2), (3), (4)] suggested that beyond serving as an exercise tool, elliptical training could help people regain the strength and flexibility required for walking.[(12)] However, as initially designed, elliptical trainers resisted movements for individuals with adequate strength who were attempting to further increase strength/endurance. They did not, yet, have the capacity to adapt to and assist movements for clients with weakness, joint pain, or movement initiation problems. Nor were they easily accessible for those with weakness and balance deficits.
The above factors served as the basis for developing ICARE, an Intelligently Controlled Assistive Rehabilitation Elliptical trainer and therapeutic program to help physically challenged individuals regain and/or retain their walking ability and physical fitness. As conceived, we hypothesized that a low-cost set of ICARE adaptations (< $750) could be added to an elliptical trainer to improve comfort, safety, usability and likelihood of achieving a beneficial workout for individuals with a disability. In addition to the benefits for individuals with a disability, we hypothesized that the modifications would not hinder use of the device by those without known disability. This latter requirement was believed to be important if the modifications were to be adopted widely into fitness facilities. The need to develop effective, accessible and affordable walking interventions is clear. Given an estimated 15 million adults living in the United States who experience difficulty with walking,[(9)] it is essential to develop accessible and appropriately challenging exercise equipment to enhance walking and cardiovascular function after discharge from therapy.
METHOD
Twenty adults volunteered to participate. Ten had chronic diseases or physical disabilities (e.g., stroke, diabetes, multiple sclerosis, traumatic brain injury, amputation, or arthritis), while ten were free from known physical disability. All were able to walk independently. Six required use of an assistive device (e.g., a cane, walker, unilateral/bilateral ankle-foot orthoses). One individual used a transfemoral prosthesis and one required both a transtibial and a transfemoral prosthesis.
The ICARE ergonomic assessment included two sessions separated by at least 24 hours. During the first session, participants were oriented to the elliptical trainer, the design modifications, and were provided with an opportunity to exercise on the device (with and without modifications). The elliptical trainer selected for study was the SportsArt Fitness E870. The device was equipped with both static as well as dynamic (moveable) handles. Additionally, based on feedback received during the first year of the ICARE study, a set of modifications was developed, refined and added to the SportsArt. Specifically, a two-step staircase was added to either side to improve access to the device as the pedals were 38 cm above the ground. A bench that straddled the pedals provided a location for clients to sit and eliminated the need to dismount between each exercise bout. Foot straps helped secure the feet to the pedals and prevented sliding or rolling on the footplates. A middle handle and two side rails were added to facilitate stability in those fearful of falling. A one-handed heart rate monitor enabled individuals with limited hand function (e.g., might arise from a stroke) to monitor their heart rate even if they could not grasp the manufacturer installed heart rate monitors. An intelligently controlled motor provided customized assistance to move the pedals when clients lacked sufficient strength or endurance to do so independently. This modified elliptical trainer was called “ICARE”.
During the second session, participants again trained on the SportsArt without modifications and with the ICARE redesign. After use of each device, participants responded to a series of questions aimed at determining to what extent each modification improved or hindered ability to use the machine. While the prime goal was to identify modifications that would improve use of the equipment by individuals with disabilities, it was also deemed important to understand the degree to which a modification might hinder the use of the device by individuals without a disability as this might reduce the likelihood of future implementation by manufacturers or fitness club owners. Additionally, for both the SportsArt and ICARE, participants completed a 10 cm visual analog scale (VAS) rating of their perceived safety, comfort, likelihood of achieving a good workout, and the usability of each device. Ratings approximating zero reflected perceptions of reduced safety, comfort, likelihood of achieving a good workout and overall usability, while values approximating 10 reflected positive perceptions of these attributes (Figure 1).
Descriptive statistics were performed for key variables using SigmaPlot 11.0 software. Frequency counts were used to describe the extent to which modifications improved or hindered device usage. Separate one-way analyses of variance with repeated measures (2 x 2 ANOVAs) identified significant differences in VAS scores of perceived safety, comfort, usability, and likelihood of achieving a good workout between the unmodified SportsArt and the ICARE in individuals with and without a disability.
RESULTS
Prior to modifying the device, one individual with physical disabilities could not get on the elliptical even with assistance, while three others required one to four examiners to physically assist. None without a disability required assistance. Following modifications, only one to three examiners were required to assist the four more physically disabled clients to access the device.
Table 1 summarizes the impact of select modifications on individual’s ability to use the device. The steps and bench notably increased ease of access for individuals with and without disabilities and did not hinder use by any of the participants tested. While the foot straps and side rails improved use in over 50% of participants tested, one individual found that the modifications hindered machine usage. The middle handle was of assistance to approximately half of individuals with a disability and one-third of those without a disability. The one-handed heart rate monitor benefitted less than half of those using the device. The motor improved the ability of 90% of those with a disability to use the elliptical and 60% of those without a disability. One participant with a disability indicated that the motor hindered equipment use.Participants with a disability felt less safe when exercising than those without a disability when averaged between elliptical conditions (VAS, disability = 6.4 vs. non-disability = 9.3; p=0.004; Figure 2). The ICARE modifications significantly improved perceptions of safety when averaged between the two groups (VAS, pre-modification = 7.0 vs. post-modification = 8.8; p=0.005), primarily due to a significant increase from pre to post modification in those with a disability (pre = 4.6, post = 8.3) compared to the minimal gain posted in those without a disability (pre = 9.3, post = 9.4; interaction p=0.006).
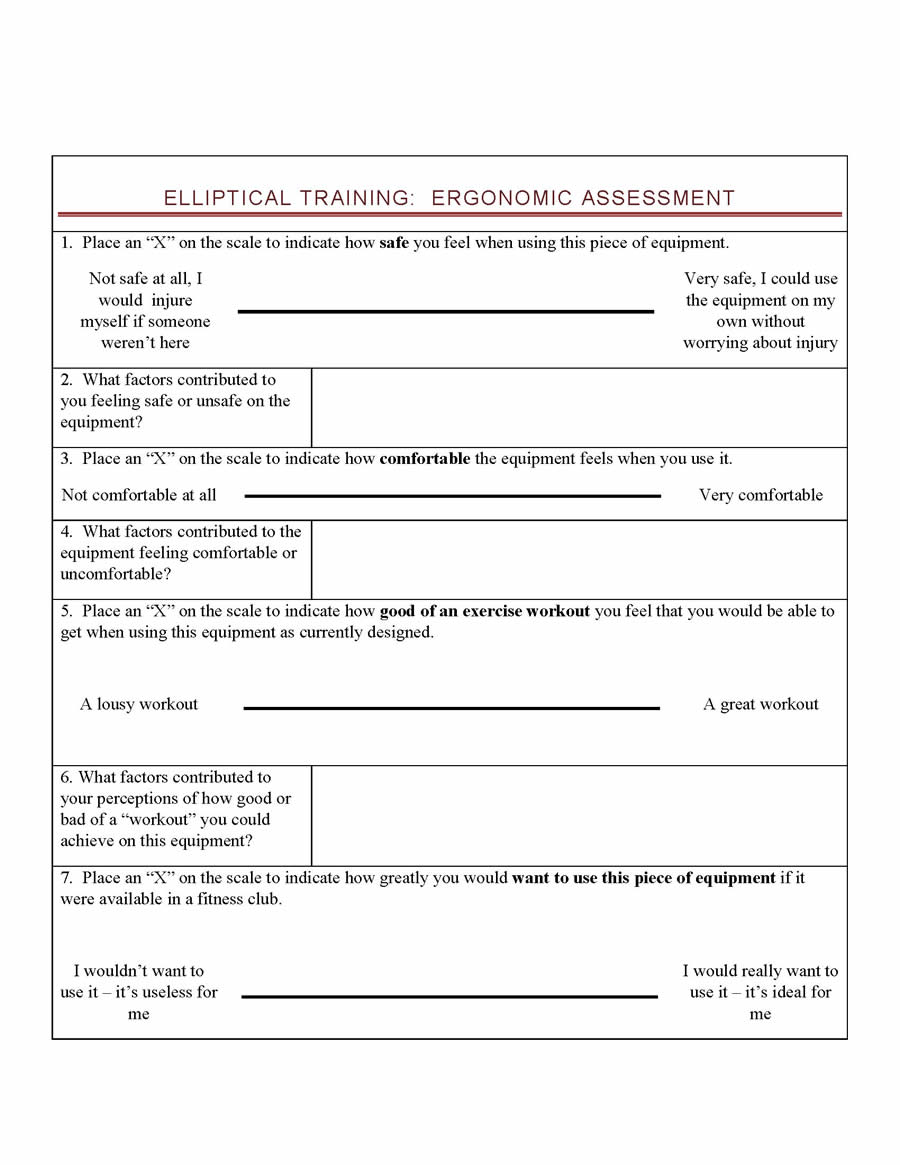 Figure 1. Visual Analog Scale
Figure 1. Visual Analog ScaleWhile individuals with a disability on average rated that they were less comfortable than those without a disability when averaged between elliptical conditions, these differences did not reach the level of statistical significance (VAS, disability = 7.1 vs. non-disability = 8.4; p=0.187). The ICARE modifications significantly improved perceptions of comfort when averaged between groups (VAS, pre-modification = 7.1 vs. post-modification = 8.5; p=0.045). Those with a disability experienced a significant increase in comfort from pre to post modification (pre = 5.7, post = 8.6) compared to the minimal decrease identified in individuals without a disability after the modification (pre = 8.5, post = 8.3; interaction p=0.028).
When averaged between the two elliptical conditions, there were no significant differences between the participant groups perceptions of being able to achieve a good workout (VAS, disability = 7.9 vs. non-disability = 8.5; p=0.384). The ICARE modifications demonstrated a trend towards improving likelihood of achieving a good workout when averaged between groups (VAS, pre-modification = 7.4 vs. post-modification = 9.0; p=0.075). The trend arose primarily from the increased perceptions of being able to achieve a good workout in those with a disability (pre = 6.1, post = 9.6) compared to the minimal decrease documented in those without a disability (pre = 8.7, post = 8.3; interaction p=0.025).
|
With Disability |
Without Disability |
||||
|---|---|---|---|---|---|---|
|
Yes |
No |
Not Needed |
Yes |
No |
Not Needed |
Steps |
|
|
|
|
|
|
Does the steps improve your ability to use the machine? |
10 |
0 |
0 |
6 |
1 |
3 |
Does the steps hurt your ability to use the machine? |
0 |
10 |
0 |
0 |
7 |
3 |
Bench |
|
|
|
|
|
|
Does the bench improve your ability to use the machine? |
7 |
2 |
1 |
3 |
0 |
7 |
Does the bench hurt your ability to use the machine? |
0 |
10 |
0 |
0 |
8 |
2 |
Foot Straps |
|
|
|
|
|
|
Does the foot straps improve your ability to use the machine? |
10 |
0 |
0 |
4 |
3 |
3 |
Does the foot straps hurt your ability to use the machine? |
0 |
10 |
0 |
1 |
8 |
1 |
Side Rails |
|
|
|
|
|
|
Does the side rails improve your ability to use the machine? |
8 |
1 |
1 |
5 |
1 |
4 |
Does the side rails hurt your ability to use the machine? |
1 |
9 |
0 |
0 |
7 |
3 |
Middle Handle |
|
|
|
|
|
|
Does the middle handle improve your ability to use the machine? |
5 |
3 |
2 |
3 |
1 |
6 |
Does the middle handle hurt your ability to use the machine? |
0 |
10 |
0 |
0 |
7 |
3 |
One-Handed Heart Rate Monitor |
|
|
|
|
|
|
Does the One-Handed Heart Rate monitor improve your ability to use the machine? |
4 |
0 |
6 |
2 |
4 |
4 |
Does the One-Handed Heart Rate monitor hurt your ability to use the machine? |
0 |
7 |
3 |
0 |
7 |
3 |
Motor Assist |
|
|
|
|
|
|
Does the motor assist improve your ability to use the machine? |
9 |
0 |
1 |
6 |
1 |
3 |
Does the motor assist hurt your ability to use the machine? |
1 |
9 |
0 |
0 |
9 |
1 |
Finally, when averaged between the two elliptical conditions, individuals with a disability rated that they were less likely to use the devices than those without a disability; however, these differences did not reach the level of statistical significance (VAS, disability = 7.5 vs. non-disability = 8.5; p=0.216). The ICARE modifications significantly improved perceptions of usability when averaged between groups (VAS, pre-modification = 7.0 vs. post-modification = 9.1; p=0.010). Those with a disability perceived of a greater increase in usability from pre to post modification (pre = 5.6, post = 9.5) compared to the more modest increase identified in individuals without a disability (pre = 8.3, post = 8.9; interaction p=0.032).
 Figure 2: Interaction of Subject Groups and Modifications
Figure 2: Interaction of Subject Groups and ModificationsDISCUSSION
The Healthy People 2010 agenda includes targets for improving the cardiovascular fitness of individuals with and without disabilities living in the United States. A recent review of progress towards these objectives indicates that while both groups have not yet achieved these goals, individuals with a disability are notably lagging compared to their non-disabled counterparts. Lack of accessible and usable equipment prevents some with disabilities from pursuing a more physically active lifestyle.
In the current study, we modified an elliptical trainer to help reduce barriers that individuals with physical disabilities experience when trying to use the device. Overall, the modifications substantially improved perceptions of safety, comfort, ability to achieve a good workout and overall usability for those with a disability. The impact of the modifications on those without a disability was minimal. Collectively, these data suggest that implementation of the modifications could enable a greater number of individuals to use the device without hindering the “traditional” user.
REFERENCES
- Albright, A., Franz, M., Hornsby, G., Kriska, A., Marrero, D., Ullrich, I., et al. (2000). American College of Sports Medicine postion stand: exercise and Type 2 diabetes. Medicine and Science in Sports and Exercise, 32(7), 1345-1360.
- Burnfield, J., Buster, T., Provorse, A., & Takahashi, S. (2007). Muscular demands during elliptical training compared to overground walking. CD of Abstracts, World Physical Therapy 2007, World Confederation for Physical Therapy.
- Burnfield, J., Shu, Y., Buster, T., & Taylor, A. Similarity of joint kinematics and muscle demands between elliptical training and walking: Implications for practice. In press, Physical Therapy.
- Buster, T., Ginoza, L., & Burnfield, J. (2006). Comparison of lower extremity sagittal plane kinematics during overground gait, treadmill walking and elliptical training Proceedings CD, American Society of Biomechanics, 30th Annual Meeting.
- Da Cunha, I., Lim, P., Qureshy, H., Hensen, H., Monga, T., & Protas, E. (2001). A comparison of regular rehabilitation with supported treadmill ambulation training for acute stroke subjects. Journal of Rehabilitation Research & Development, 38, 245-255.
- Durstine, J. L., Painter, P., Franklin, B. A., Morgan, D., Pitetti, K. H., & Roberts, S. O. (2000). Physical activity for the chronically ill and disabled. Sports Medicine, 30(3), 207-219.
- Eng, J. J., Chu, K. S., Kim, C. M., Dawson, A. S., Carswell, A., & Hepburn, K. E. (2003). A community-based group exercise program for persons with chronic stroke. Medicine and Science in Sports and Exercise, 35(8), 1271-1278.
- Laufer, Y., Dickstein, R., Chefez, Y., & Marcovitz, E. (2001). The effect of treadmill training on the ambulation of stroke survivors in the early stages of rehabilitation: a randomized study. Journal of Rehabilitation Research and Development, 38(1), 69-78.
- Lethbridge-Cejku, M., Rose, D., & Vickerie, J. (2006). Summary health statistics for U.S. Adults: National Health Interview Survery, 2004. National Center for Health Statistics. Vital and Health Statistics 10(228).
- Miyai, I., Fujimoto, Y., Ueda, Y., Yamamoto, H., Nozaki, S., Saito, T., et al. (2000). Treadmill training with body weight support: its effect on Parkinson's disease. Archives of Physical Medicine & Rehabilitation, 81(7), 849-852.
- Penninx, B. W. J. H., Messier, S. P., Rejeski, W. J., Williamson, J. D., DiBari, M., Cavazzini, C., et al. (2001). Physical exercise and the prevention of disability in activities of daily living in older persons with osteoarthritis. Archives of Internal Medicine, 161(19), 2309-2316.
- Perry, J., Burnfield JM (2010). Gait Analysis, Normal and Pathological Function, 2nd Edition. Thorofare, NJ: Charles B. Slack.
- Rimmer, J. H., Riley, B., Wang, E., Rauworth, A., & Jurkowski, J. (2004). Physical activity participation among persons with disabilities: barriers and facilitators. American Journal of Preventitive Medicine, 26(5), 419-425.
- U.S. Department of Health and Human Services. (2000). Healthy People 2010. 2nd Edition. With understanding and improving health and objectives for improving health. 2 vols. Focus Area 22. Physical activity and fitness. Washington, DC: U.S. Government Printing Office.
ACKNOWLEDGEMENT
This work was supported in part by a grant from the Department of Education, NIDRR grant number H133G070209.