Movement-based Gameplay Therapy for a Child with Cerebral Palsy: A Single subject study
Sharon Stansfield1, Carole Dennis2, Hélène Larin3, Courtney Gallagher4
1Computer Science, 2Occupational Therapy, 3Physical Therapy Departments
Ithaca College, Ithaca, NY
4Spaulding Rehabilitation Hospital, Boston, MAINTRODUCTION
Children with cerebral palsy (CP) often present asymmetrical or unilateral impairments that limit the use of their upper extremity, a condition known as learned nonuse or developmental disregard. Children may be unable to perform daily functional tasks that require the coordinated use of both arms. Some form of constraint-induced movement therapy (CIMT) is frequently used as a treatment strategy. CIMT is designed to improve function in children with motor impairment by constraining the less-affected limb and having the child practice repetitive tasks with the more-affected limb. The purpose of CIMT is to increase spontaneous use of the affected limb and limit the effects of learned nonuse. CIMT has been shown to be useful in children with CP (Y.-P. Chen, Pope, Tyler, & Warren, 2014). Unfortunately, it is not especially child-friendly (Wu, Hung, Tseng, & Huang, 2013). In this paper we present a single-subject study in which a non-immersive, motion tracking-based game is the mechanism for delivering CIMT-like therapy. The game, which was designed to elicit desired therapeutic movements, provides the intensive, structured training required by CIMT in a fun and competitive environment. Repeated measures assessed were speed of reach with the affected upper extremity, dissociation of movement for enhanced upper extremity skills and bilateral integration of the upper extremities in a functional task. The subject’s performance improved in all measures, implying that motion-based gameplay may be as effective as CIMT, while being far more enjoyable for the child.
Related work
Research on the effectiveness of VR therapy for motor impairment has been on-going for several years, with mixed results. Of particular relevance to this work are the studies that have addressed the use of VR therapy for upper extremity impairment. (Y. Chen, Lee, & Howard, 2014) (Reid & Campbell, 2006), (You et al., 2005), (Green & Wilson, 2012) and those that have used various motion-based games for the same purpose (Li, Lam-Damji, Chau, & Fehlings, 2009), (Y. Chen, Kang, Chuang, Doong, & Lee, 2007), (Levac, Miller, & Missiuna, 2012). In this paper we present a single subject study with the following differences from most previous work: The motion-based system used was a “general purpose,” noncommercial platform used in multiple previous academic and research projects, but the game developed was targeted specifically toward eliciting the movements desired by the therapist ― these requirements were developed prior to programming the game.
Methods and Procedures
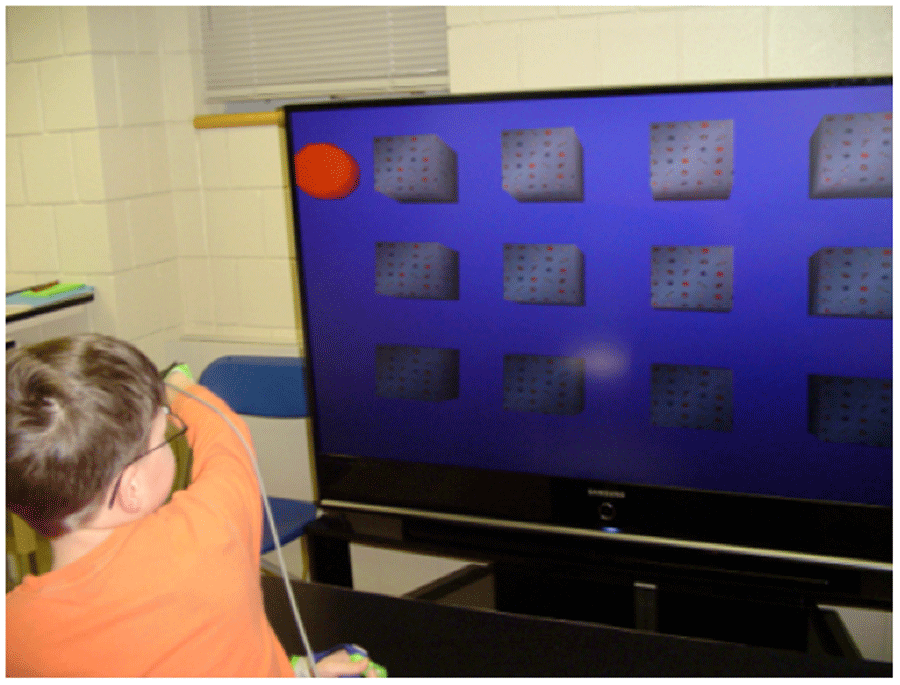 Figure 1: Child playing memory game
Figure 1: Child playing memory game
The video game developed for this study was a three-dimensional version of the traditional “memory” game in which the player must find six matching pairs of animal images on the faces of cubes arranged in a grid. The position of the blocks was calibrated to the measured limits of the child's right arm reach. A 55-inch HD TV was used as the display, and a Polhemus Liberty™ magnetic motion tracking system was used to track the child’s right hand and to update the position of a red sphere representing his hand movement in the game. Since the motion of his left hand could not affect the game, it was unnecessary to constrain this arm. Figure 1 shows this experimental platform.
A single-subject AB design was utilized to assess within-subject performance. Measures of performance across baseline and intervention phases were used to determine whether the intervention resulted in changes in any of the following repeated measures.
- Speed of reach with the affected upper extremity, calculated from motion tracker data. Speed was measured in mm/sec.
- Enhanced upper extremity skills, measured using the dissociated movement subscale from the Quality of Upper Extremity Skills Test (QUEST) (DeMatteo et al., 1993). The dissociated movement subscale includes measures of the limitations of the active range of motion. Raw scores for QUEST range from 50-100; scores are normalized to a range of 0-100.
- Bilateral integration of the upper extremities in a functional task, measured using the Goal Attainment Scale (GAS) which scores between -2 and +2. Hand-washing was the child’s chosen task.
 Figure 2: “Dangling Fish” used to measure speed of reach. The position tracker is attached to the subject’s hand.
Figure 2: “Dangling Fish” used to measure speed of reach. The position tracker is attached to the subject’s hand.
Results and Conclusion
Speed of reach to and from the target fish was analyzed using the two standard deviation band method (Nourbakhsh & Ottenbacher, 1994). To use this method, the mean and standard deviation are calculated for the baseline data. Bands are drawn at ±2 standard deviations on a graph containing the post-intervention data points. If two or more consecutive data points fall outside of the two standard deviation range, then a statistically significant change in performance has occurred. Using this method, a statistically significant change in the speed of reach was found for all three positions between the pre-baseline and post-intervention assessments.
QUEST dissociated movement scores were 81.25 at pre-baseline, 92.88 at post-baseline, and 100 at post-intervention, demonstrating a ceiling effect. Limitations of range of motion were noted in right shoulder abduction, elbow flexion and extension, and wrist extension at pre-baseline. Limitations persisted in elbow flexion and extension, and wrist extension at post-baseline. These limitations were resolved at post-intervention, when the child demonstrated full range of motion in all planes of movement.
The child scored a -1 on the GAS for bilateral integration at the initial baseline assessment, completing 6 of 15 subtasks. At post-baseline, he scored a 0, completing 9 of 15 subtasks. At post-intervention, he scored a +2, the highest possible score, completing all 15 subtasks independently.
In conclusion, these results imply that motion-based gameplay may an effective adjunct to interventions, such as CIMT, while presenting a more enjoyable experience for the child: The subject rated his satisfaction with the game as a 5 (maximum score) after both the first and last sessions in which it was used. The fact that the game is more enjoyable than traditional CIMT may further encourage continued compliance with the prescribed regimen, as a child is more likely to continue with an activity that is enjoyable than with one that is not.
REFERENCES
Chen, Y., Kang, L., Chuang, T., Doong, J., & Lee, S. (2007). Upper-Extremity Control in Children With Cerebral Palsy : A Single-Subject Design. Physical Therapy, 87(11), 1441–1458.
Chen, Y., Lee, S.-Y., & Howard, A. M. (2014). Effect of virtual reality on upper extremity function in children with cerebral palsy: a meta-analysis. Pediatric Physical Therapy : The Official Publication of the Section on Pediatrics of the American Physical Therapy Association, 26(3), 289–300. doi:10.1097/PEP.0000000000000046
Chen, Y.-P., Pope, S., Tyler, D., & Warren, G. L. (2014). Effectiveness of constraint-induced movement therapy on upper-extremity function in children with cerebral palsy: a systematic review and meta-analysis of randomized controlled trials. Clinical Rehabilitation, 28(10), 939–53. doi:10.1177/0269215514544982
DeMatteo, C., Law, M., Russell, D., Pollock, N., Rosenbaum, P., & Walter, S. (1993). The Reliability and Validity of the Quality of Upper Extremity Skills Test. Physical & Occupational Therapy in Pediatrics, 13(2), 1–18.
Green, D., & Wilson, P. H. (2012). Use of virtual reality in rehabilitation of movement in children with hemiplegia--a multiple case study evaluation. Disability and Rehabilitation, 34(7), 593–604. doi:10.3109/09638288.2011.613520
Levac, D., Miller, P., & Missiuna, C. (2012). Usual and virtual reality video game-based physiotherapy for children and youth with acquired brain injuries. Physical & Occupational Therapy in Pediatrics, 32(2), 180–95. doi:10.3109/01942638.2011.616266
Li, W., Lam-Damji, S., Chau, T., & Fehlings, D. (2009). The development of a home-based virtual reality therapy system to promote upper extremity movement for children with hemiplegic cerebral palsy. Technology and Disability, 21(3), 107–113.
Nourbakhsh, M. R., & Ottenbacher, K. J. (1994). The Statistical Analysis of Single-Subject Data: A Comparative Examination. Physical Therapy, 74(8), 768–776.
Reid, D., & Campbell, K. (2006). The use of virtual reality with children with cerebral palsy: a pilot randomized trial. Therapeutic Recreation Journal, 40(4), 255–268. Retrieved from http://www.mendeley.com/research/virtual-reality-children-cerebral-palsy-pilot-randomized-trial/
Wu, W., Hung, J., Tseng, C., & Huang, Y. (2013). Group constraint-induced movement therapy for children with hemiplegic cerebral palsy: a pilot study. The American Journal of Occupational Therapy : Official Publication of the American Occupational Therapy Association, 67(2), 201–8. doi:10.5014/ajot.2013.004374
You, S. H., Jang, S. H., Kim, U.-H., Kwon, O.-H., Barrow, I., & Hallett, M. Case report Cortical reorganization induced by virtual reality therapy in a child with hemiparetic cerebral palsy, 47 Developmental Medicine & Child Neurology 2005 628–635 (2005).
Acknowledgements
The authors would like to thank the child and his mother for their participation in this study, as well as the undergraduate students who worked on all aspects of the project with us.