Gabrielle Lemire![]() 1,2
1,2![]() , Simon Latour
, Simon Latour![]() 1
1![]() , Andréanne Blanchette
, Andréanne Blanchette![]() 1,3
1,3![]() , Véronique Flamand
, Véronique Flamand![]() 1,3
1,3![]() , Alexandre Campeau‑Lecours
, Alexandre Campeau‑Lecours![]() 1,2
1,2![]()
![]() 1
1![]() Centre interdisciplinaire de recherche en réadaptation et intégration sociale (Cirris), Quebec City, Quebec, Canada,
Centre interdisciplinaire de recherche en réadaptation et intégration sociale (Cirris), Quebec City, Quebec, Canada, ![]() 2
2![]() Robotics Laboratory, Laval University, Quebec City, Quebec, Canada,
Robotics Laboratory, Laval University, Quebec City, Quebec, Canada, ![]() 3
3![]() Department of Rehabilitation, Laval University, Quebec City, Quebec, Canada
Department of Rehabilitation, Laval University, Quebec City, Quebec, Canada
ABSTRACT
This paper presents the development of a low-cost active planar upper limb rehabilitation robotic device, which aims to help in the rehabilitation process of people living with movement disorders. Many people living with conditions such as cerebral palsy, stroke, spinal cord injury or muscular dystrophy experience upper limb impairments (muscle spasticity, lack of selective motor control, muscle weakness or tremors), and require physical and occupational therapy to maintain or gain motor performance. The proposed device is designed to be fixed on a table. Direct current (DC) motors control the two degrees of freedom (DOF) of the mechanism. The user interacts with the device using a handle. The device is designed so that the handle stays in the same orientation all the time. The device offers different levels of assistance to guide planar movements, going from a complete assistance, where the user is guided by the mechanism that performs predefined movements recorded by the therapist, to the addition of resistance during the movement, where the user moves the end effector without the help of the mechanism and the latter adds perturbations.
INTRODUCTION
The inability for people to use their arms to grab, manipulate or move objects limits their daily life and professional activities [1] . Such limitations are due to upper limb impairments, which can result from many causes [1] such as stroke, spinal cord injury, cerebral palsy and muscular dystrophy. Motor development or recovery can greatly improve the quality of life of people living with these conditions [2] . Furthermore, for acquired injuries such as stroke and spinal cord injury, which respectively affect approximately 795,000 [3] and 17,900 persons [4] every year in the United States alone, the recovery depends, to a great extent, on the intensity and frequency of rehabilitation therapies during the first months after the event/accident [1] . For instance, both the spinal cord and the brain have a certain plasticity, and can recover from a loss of capacity with activity-based repetitive movement training [5].
One important challenge is that rehabilitation therapies need to be supervised and assisted by healthcare professionals, but since needs are high and resources are limited, users may not be treated in a timely and optimal manner. This will exacerbate with the ageing of the population since we will have to collectively take care of more people with reduced independence, but with fewer active resources [6], [7].
In the past few years, robotic rehabilitation devices have gained in popularity. These devices are not intended to replace healthcare professionals, but rather to be used as additional tools to provide patients with increased opportunities to perform repetitive movements [2] . Commercially available rehabilitation devices for the upper body include the Kinarm , the REAplan and the ReoGo . Similarly to motorized assistive technologies where the main limitation to accessibility is cost [8]–[11], the available devices are expensive, ranging from $40,000 to $265,000.
OBJECTIVES
The objective of this article is to present the preliminary design of a low-cost active planar upper limb rehabilitation robotic device. The specific objectives are 1) the development of the robotic hardware and 2) the development of algorithms allowing to adapt to the user's capacities and to propose a progression in the levels of difficulty during the rehabilitation.
DEVELOPMENT
Hardware
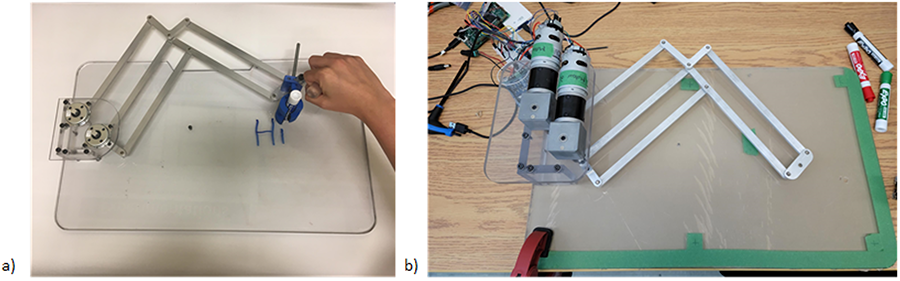
The mechanism is inspired by the passive assistive handwriting device shown in Figure 1a [12]. The design is made of a five-bar mechanism and has two degrees of freedom (DOF). The mechanism has two angular DOFs, and the end effector moves on a Cartesian plane. Two parallelograms were added, one for each bar. This limits the rotation of the end effector. Another parallelogram was added to transfer control of the second rotation to the base. This created an assistive handwriting device where the pen (and the end effector) is always maintained in the same orientation relative to the user, and the control of the two DOFs is located at the base of the mechanism. Two rotary dampers were added to the device joints. As a result, the dampers suppress the rotary motions of the mechanism's bar. As these dampers are linked directly to the bars that control the two DOFs, they move proportionally to each DOF. The user interacts through a handle placed at the end effector.
Then, as seen in Figure 1b, the mechanical dampers were replaced by two DC motors (T-MOTOR AK60-6) that control the two DOFs of the mechanism. The bars and the pivot points are optimized so that each joint works almost at the same level anywhere in the working plane [12].
Figure 1 – a) passive handwriting mechanism with dampers at the joints, b) active mechanism inspired by the passive version with DC motors at the joints.
Algorithms
As motor skills of the upper limb vary from one person to another, and along time for any given person, the development of the algorithms must adapt to the users' capacities, evolve with the users' recovery, and help them make progress. The algorithms were thus designed to represent a progression in difficulty, from complete assistance (where the user is guided by the device that is moving according to a predefined motion) to added resistance during motion (where the user moves the end effector without help from the device, and the device adds disturbance). These levels are described as follows.
1- Automatic execution of a predefined motion
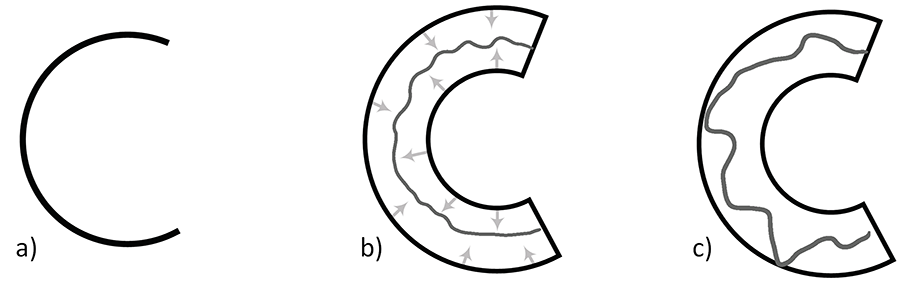
The first level is the one with the most assistance. The mechanism executes a predefined motion. Some movements like the formation of alphabet letters are pre-recorded. It is also possible to add new motions (e.g., square, triangle, number, etc.). Figure 2 a represents this level of assistance for the letter C. The device performs the whole motion autonomously, thus guiding the user's hand.
For now, predefined motions are all capital letters. The shapes and the order of execution of the different lines and curves are based on the same method that is taught in kindergarten and first years of elementary schools, and were reviewed by an occupational therapist.
2- Assistance for a predefined shape with lateral stiffness
This level uses the same predefined shapes as in level 1, but the mechanism does not move for the user. Thanks to virtual stiffness, it rather allows some flexibility to guide the user on the right path. There is no resistance to go forwards. When the user tries to go sideways, a virtual spring applies a force on the end effector towards the right path. The algorithm is developed so that it is impossible for the user to go backwards. This is represented in Figure 2b with arrows representing the repulsion from the virtual springs. The stiffness of the virtual springs can be modified in the software and through a user interface.
3- Assistance for a predefined shape with barriers
Similarly to the previous level of assistance, motion is impossible backwards and there is no resistance to go forwards. The main difference is with the side movements. Instead of a virtual spring for side to side movements, the user is allowed to move sideways with no resistance up to a certain distance from the prescribed path. At that point, the mechanism blocks the motion thanks to a virtual wall. Figure 2c shows the effects of those barriers on the writing of the letter C. The distance between the virtual wall and the original line can be modified in the software and via a user interface.
4- Free movement with damping for uncoordinated movements
This level allows the user to move freely, without any restriction, but adds damping to the movements in order to limit the effect of uncoordinated movements. The damping is added only when uncoordinated movements are detected. The mechanism can detect uncoordinated movements by analyzing the end effector speed, acceleration and jerk.
5- Free movement without disturbance
This level allows the user to move freely, without any restriction. Furthermore, the friction from the actuators is compensated by an algorithm in order to increase movement transparency.
6- Free movement with disturbance
The last level of assistance is similar to level 5, but disturbances are added in every direction, in order to create a challenging environment, and a form of sensorimotor training for the user.
DISCUSSION
In this paper, the design of a low-cost active planar upper limb rehabilitation robotic device was presented. The objectives were to develop the hardware or the mechanism, and to create algorithms to control the device with different levels of assistance. This device aims to extend treatment time and help in the recovery process of individuals living with movement disorders. Up to now, the first three levels and level 5 are completed, and the algorithms are ready to be tested out by potential users. The other two levels, 4 and 6, are under development. Future work will consist of evaluating the prototype with potential users in order to assess its efficacy to help in the improvement of writing or drawing skills.
CONCLUSION
This paper has presented the design of a low-cost active planar upper limb rehabilitation robotic device. The mechanical design was presented along with six algorithms that create a progression in difficulty and assistance. It starts from the device that moves by itself to the user controlling the device with added disturbances. The objectives were 1) the development of the robotic hardware and 2) the preliminary development of algorithms allowing progressive difficulty in rehabilitation therapies. In the short term, future work includes completing the implementation of the algorithms, and preclinical validation with potential users.
REFERENCES
[1] A. T. Silveira, M. A. de Souza, B. L. Fernandes, and P. Nohama, "From the past to the future of therapeutic orthoses for upper limbs rehabilitation," Res Biomed Eng, vol. 34, no. 4, pp. 368–380, 2018.
[2] H. Singh et al., "Robot-assisted upper extremity rehabilitation for cervical spinal cord injuries: a systematic scoping review," Disabil Rehabil Assist Technol, vol. 13, no. 7, pp. 704–715, 2018.
[3] CDC, "Stroke facts," 2021. https://www.cdc.gov/stroke/facts.htm#:~:text=Stroke Statistics&text=Every year%2C more than 795%2C000,are first or new strokes.&text=About 185%2C000 strokes—nearly 1,have had a previous stroke. (Accessed Jan. 28, 2022.)
[4] NSCISC, "Spinal cord injury facts and figures at a glance." https://www.nscisc.uab.edu/Public/Facts and Figures - 2021.pdf.
[5] Z. Kadivar et al., "RiceWrist robotic device for upper limb training: feasibility study and case report of two tetraplegic persons with spinal cord injury," Int J Biol Eng, vol. 2, no. 4, pp. 27–38, 2012.
[6] H. F. M. Van Der Loos, D. J. Reinkensmeyer, and E. Guglielmelli, "Rehabilitation and health care robotics," in Springer Handbook of Robotics, Springer International Publishing, 2016, pp. 1687–1728.
[7] R. Choinière, Vieillissement de la population, état fonctionnel des personnes âgées et besoins futurs en soins de longue durée au Québec. Institut national de santé publique Québec, 2010.
[8] A. G. Dell, D. A. Newton, and J. G. Petroff, Assistive technology in the classroom: Enhancing the school experiences of students with disabilities. Pearson, 2008.
[9] Stat, "Participation and Activity Limitation Survey: Assistive aids and devices for adults," 2008.
[10] Statistics Canada, "Disability in Canada : initial findings from the Canadian Survey on Disability," 2013.
[11] R. Arim, A profile of persons with disabilities among Canadians aged 15 years or older. Statistics Canada, 2012.
[12] G. Lemire, T. Laliberté, K. Turcot, V. Flamand, and A. Campeau-Lecours, "Preliminary design of a device to assist handwriting in children with movement disorders," in Rehabilitation Engineering and Assistive Technology Society of North America (RESNA), Aug. 2019, accessed: Aug. 21, 2019. [Online.] Available: http://arxiv.org/abs/1908.02221.