Caregiver Pushing Versus Pulling An Occupied Wheelchair In A High-Rolling-Resistance Setting: Validation Of A Biomechanical Model
R. Lee Kirby![]() 1
1![]() , Kim Parker
, Kim Parker![]() 2
2![]() , Eric Poon
, Eric Poon![]() 3
3![]() , Cher Smith
, Cher Smith![]() 4
4![]() , Michel Ladouceur
, Michel Ladouceur![]() 5
5![]()
![]() 1
1![]() Division of Physical Medicine and Rehabilitation, Dalhousie University;
Division of Physical Medicine and Rehabilitation, Dalhousie University; ![]()
2![]() Assistive Technology Program, Nova Scotia Health;
Assistive Technology Program, Nova Scotia Health; ![]()
3![]() Class of 2023, Faculty of Medicine, Dalhousie University;
Class of 2023, Faculty of Medicine, Dalhousie University;
![]() 4
4![]() Department of Occupational Therapy, Nova Scotia Health;
Department of Occupational Therapy, Nova Scotia Health;
![]() 5
5![]() Kinesiology, School of Health and Human Performance, Dalhousie University; Halifax, NS, Canada
Kinesiology, School of Health and Human Performance, Dalhousie University; Halifax, NS, Canada
ABSTRACT
Introduction: Caregivers experience difficulties in getting occupied wheelchairs over soft surfaces. Because rolling resistance is inversely proportional to wheel diameter, the less force on the smaller-diameter wheelchair casters (front wheels) the better.
Objective: To test the hypothesis that forward forces ("pushes") horizontally applied to the push-handles would push the casters into the surface and backward forces ("pulls") would lift the casters from the surface.
Methods: We developed a biomechanical model to compare forward forces ("pushes") with backward forces ("pulls") horizontally applied to the push-handles from the perspective of the vertical forces between the casters and the surface. To empirically validate the model, we positioned.the casters of an occupied manual wheelchair on a force platform. The rear wheels were prevented from moving by chocks. Horizontal forces were gradually increased from 0 to maximal over a period of about 15 seconds. The forces from a push-handle-mounted load cell and the force platform under the casters were continuously recorded at 200 Hz.
Results: Forward forces caused the force under the casters to gradually increase until the wheelchair shifted. Backward forces caused the force under the casters to gradually decrease until they lifted off the surface.
Conclusion: This empirically validated biomechanical model suggests that caregivers should pull rather than push occupied wheelchairs when high rolling resistance is encountered.
INTRODUCTION
One aspect of the wheelchair-provision process that can enhance the benefits and minimize the problems of wheelchair use is the training of wheelchair skills.[1-3] Caregivers of individuals who are wheelchair users are at risk of injury.[4,5] Roberts et al.[6] reported that 77% of 195 caregivers who pushed wheelchairs had received no wheelchair training but the caregivers who did receive training reported less shoulder, back, wrist and elbow pain. In an uncontrolled pilot study looking at the effectiveness of the WSTP in improving the manual wheelchair skills of untrained caregivers, Kirby et al. [7] found an increase from a pre-training total WST score of 77.8% to a post-training score of 94.7% (p < 0.001), a 22% relative increase that was retained at 6 months follow-up.
However, only 55% of 42 wheelchair users at discharge from a rehabilitation center reported having received wheelchair skills training and only 22% of them reported that a caregiver was present during training.[8] In an online survey [9] to document the extent and nature of wheelchair user and caregiver wheelchair-skills training by occupational therapists in Nova Scotia, of the respondents to the question "…do you typically provide wheelchair-skills training…?", only 40 (46.0%) answered "Yes, usually" for caregivers. The median duration of training sessions for caregivers was only 20 minutes and the median number of sessions was 1. Clearly more work is needed on wheelchair skills training for caregivers.
Although caregivers experience difficulties with a variety of skills, the "gets over soft surface" skill is the one for which the research evidence is least clear. Rolling resistance is inversely proportional to wheel diameter and the smaller diameter and narrow width of most caster tires in comparison to rear-wheel tires allow them to sink into further into a soft surface. Anecdotal evidence suggests that a caregivers have less difficulty on soft surfaces if they pull the wheelchair backward rather than push it forward.
OBJECTIVE
To test the hypothesis that forward forces ("pushes") horizontally applied to the push-handles tend to push the casters into the surface and backward forces ("pulls") tend to lift the casters from the surface.
METHODS
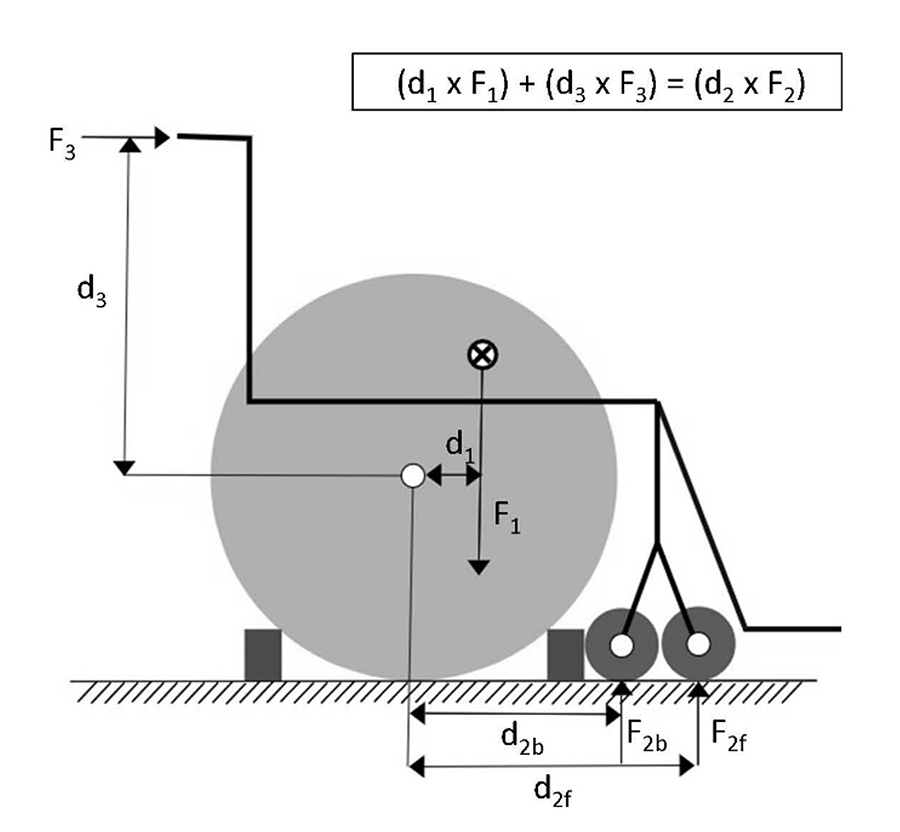
We developed a biomechanical model to compare forward forces with backward forces from the perspective of the vertical forces between the casters and the surface. The forces induce moments of force (torque) about the rear wheel axles. In Figure 1, F1 is due to gravitational forces acting on the combined center of mass of the wheelchair occupant and the wheelchair (minus the rear wheels), F2 is the reactive force under the casters trailing either forward (Ff) or backward (Fb) and F3 is the horizontal force applied to the push-handles. d1 is the horizontal distance from the rear-wheel axle to the F1 force vector, d2b is the horizontal distance from the rear-wheel axle to the F2b force vector, d2f is the horizontal distance from the rear-wheel axle to the F2f force vector and d3 is the vertical distance from the rear-wheel axle to the F3 force vector. The rear wheels are unlocked but prevented from rolling forward or backward by chocks to simulate a high-rolling-resistance setting (e.g., a soft surface). The Figure illustrates the equilibrium condition of balanced clockwise and counterclockwise moments of force. If F3 is in the backward direction, F2 will be lessened in comparison with F3 in the forward direction that will increase F2. Additionally, in the backward direction, the casters trail forward, providing a longer moment arm for F2.
To empirically validate the model, we used a Quickie 2 manual wheelchair with a cross-brace folding frame. The rear wheels were 61 cm in diameter with smooth polyurethane tires and axle positions in the mid-range vertically and fore-aft. The casters were 15 cm in diameter with smooth solid poyurethane tires and a caster trail of 5.24 cm. The wheelbase with the casters trailing backward was 46.5 cm and 57.0 cm with the casters trailing forward. The sling seat was covered by a contoured foam cushion 10 cm thick. The upholstered sling backrest is 40.5 cm above the midpoint of the seat. The horizontal cylindrical push-handles at the top of the backrest canes were straight, 10 cm long, 3 cm in diameter and rubber-coated. Swinging removable footrests with a hanger angle of 70 degrees, flip-up footplates and heel loops were used on both sides. The lowest point on the footrests was 8 cm above the surface. Padded, removable, elevating desk-length armrests were present on both sides.
The caregiver and wheelchair occupant were both investigators so that no informed consent was necessary. The wheelchair occupant was an able-bodied woman (weight 70 kg, height of 170 cm). She was seated in the wheelchair with her hands folded in her lap and her position on the seat maintained with a pelvic belt. The casters were positioned on a force platform embedded in the floor with the rear wheels off the platform. The wheel locks were unlocked. The rear wheels were prevented from moving by chocks in front of and behind them (bricks on a carpet underlay to minimize slippage). In this high-rolling-resistance setting, the wheelchair frame was free to rotate about the axles of the rear wheels but the rear wheels were not free to roll.
Horizontal forces were applied by a single caregiver (weight 73 kg, height 173 cm) to a load cell that was rigidly attached to the wheelchair push-handles. The wheelchair weighed 20.1 kg including the weight of the load cell and its connector to the push-handles. The forces applied by the caregiver were gradually increased over a 15-second period from zero until maximum or an event (e.g., caster lift-off) occurred. Forces from the load cell and force platform were continuously recorded at 200 Hz under four test conditions – forward and backward forces, each with the casters trailing forward and backward.
RESULTS
Forward forces caused the force under the casters to gradually increase until the wheelchair shifted. Backward forces caused the force under the casters to gradually decrease until they lifted off the surface.
The conditions, endpoints and qualitative results are shown in Table 1. Further quantitative analysis is in progress.
| # | Direction of applied force | Caster position | Endpoint | Force under casters |
| Forward | Forward | Wheelchair shifted | Gradually rose | |
| Backward | Caster lift-off | Gradually fell | ||
| Backward | Forward | Wheelchair shifted | Gradually rose | |
| Backward | Caster lift-off | Gradually fell |
DISCUSSION AND CONCLUSION
These findings empirically validate the biomechanical model and corroborate our hypothesis. These findings suggest that caregivers should pull rather than push occupied wheelchairs when high rolling resistance is encountered. However, further testing is needed while caregivers push or pull occupied wheelchairs on soft surfaces.
REFERENCES
[1] World Health Organization. Guidelines on the provision of wheelchairs in less resourced settings. 2008. http://www.who.int/disabilities/publications/technology/wheelchairguidelines/en/. Accessed February 11, 2019.
[2] Tu C-J, Liu L, Wang W, Du H-P, Wang Y-M, Xu Y-B, Li P. Effectiveness and safety of wheelchair skills training program in improving the wheelchair skills capacity: a systematic review. Clin Rehabil. 2017;31:1573-82.
[3] Keeler L, Kirby RL, Parker K, McLean KD, Hayden J. Effectiveness of the Wheelchair Skills Training Program: a systematic review and meta-analysis. Disabil Rehabil Assist Technol. 2018:https://doi.org/10.17483107.2018.1456566 (Epub ahead of print).