Nicole L Zaino![]() 1
1![]() , Zahra McKee
, Zahra McKee![]() 1
1![]() , Charlotte D Caskey
, Charlotte D Caskey![]() 1
1![]() , Katherine M Steele
, Katherine M Steele![]() 1
1![]() , Heather A Feldner
, Heather A Feldner![]() 2
2![]()
![]() 1
1![]() Department of Mechanical Engineering, University of Washington,
Department of Mechanical Engineering, University of Washington, ![]() 2
2![]() Department of Rehabilitation Medicine, University of Washington
Department of Rehabilitation Medicine, University of Washington
INTRODUCTION
Cerebral palsy (CP) is a non-progressive neuromuscular disorder caused by an injury to the developing brain. CP is the most common pediatric motor disability in the United States, affecting over 2 per 1000 live births [1, 2]. CP affects gross motor function, often requiring individuals to use mobility aids such as orthoses and walkers. Introducing mobility aids early in a child's development is important to support self-initiated movement and development [3]. However, there is limited literature on early intervention and mobility aids for children under the age of 5. The timing, processes, and perceptions of mobility aid prescription and use are not well understood. The goal of this study was to understand the prescription process, expectations, initial use, and impacts of the first mobility aid for young children with CP from parent and clinician perspectives. This work will inform future prescription practices and the deployment of early mobility aids for young children with CP.
METHODS
We performed a mixed-methods study that consisted of surveys and semi-structured interviews. We completed this study virtually with individuals in the United States, recruited via convenience sampling through known clinical networks. All procedures in this study were approved by the authors' institutional review board, and written consent was obtained from everyone who participated in the interview portion of the study. Surveys were distributed via REDCap (Vanderbilt University, Nashville, TN). Two authors (NZ & CC) conducted the semi-structured interviews, which were audio recorded and transcribed verbatim. Surveys and interviews focused on the following most common mobility aids among children with CP: hinged or solid ankle foot orthoses (AFOs)supra-malleolar orthoses (SMOs), anterior or posterior walkers, and gait trainers [4].
Participants
Survey participants included 29 clinicians (21 physical therapists, 4 orthotists, 4 physicians) and 6 parents. A subset of seven clinicians (5 physical therapists and 2 orthotists) completed the optional semi-structured interview; these clinicians had 5 to 20+ years of experience working with children with CP. Parent participants had children across all Gross Motor Functional Classification Scale (GMFCS) levels (child's age: 5.7± 1.9 years) who received their first mobility aid under the age of 5 years old.
Procedure
The de-identified open-ended survey responses and transcribed interviews were analyzed and coded using constant comparison until themes emerged. Two authors (NZ & ZM) completed independent content analysis using inductive coding [5]. Differences in interpretation were resolved through discussion until a consensus was reached. The codes were consolidated into themes through discussion.
RESULTS
Three themes emerged from the data:
- obstacles to provision are frequent
- mobility aids have mixed impact on daily activities, and
- clinician education and training influences the prescription process.
Obstacles to provision are frequent
When considering AFO and SMO provision (n=29), 41% of clinicians said they are satisfied with the current prescription process, 17% were satisfied with the ability to try different types of orthoses, 34% were satisfied with the length of time for the family to receive the orthoses after prescription, 37% were satisfied with insurance coverage for orthoses, and 31% were satisfied with shoe options for orthoses. For walkers (n=27), 37% of clinicians were satisfied with the current prescription process, 44% were satisfied with the availability to trial walkers, 11% were satisfied with the length of time for the family to receive the walker after prescription, and 26% were satisfied with insurance coverage for walkers.
A significant factor affecting satisfaction with the process for receiving orthoses versus walkers is the length of time to receive the device after prescription (34% satisfaction for AFOs and 11% satisfaction for walkers). Three clinicians also reported that the timing of prescription for all mobility aids was a key part of their prescription decision process with a wait time ranging from 2 to 9 months before delivery. In one interview a physical therapist stated:
"The kids should be up on their feet three months earlier, and then it's six months to nine months before they get their walker."
The clinicians did highlight both parts of the provision process that work well and thoughts for improvement, as one orthotist said:
"Having more of an interdisciplinary collaborative opportunity or setting makes a lot of sense. I've seen that with amputee treatment with prosthetics and less so with orthotics, especially with children. But I think having an opportunity to have a clinic where you've got a physician, an orthotist, and a physical therapist would be a huge benefit and improvement to the process."
The largest obstacles to provision of mobility aids stated by clinicians included insurance (7), cost (5), family goals/acceptance (4), and access to trial devices (3). As one physical therapist shared:
"The process, the tediousness, and the time it takes for all the paperwork and the process. I'd say that's the biggest [challenge] because the others you can work around, but that one, you just have to slog through it."
Mobility aids have mixed impact on daily activities
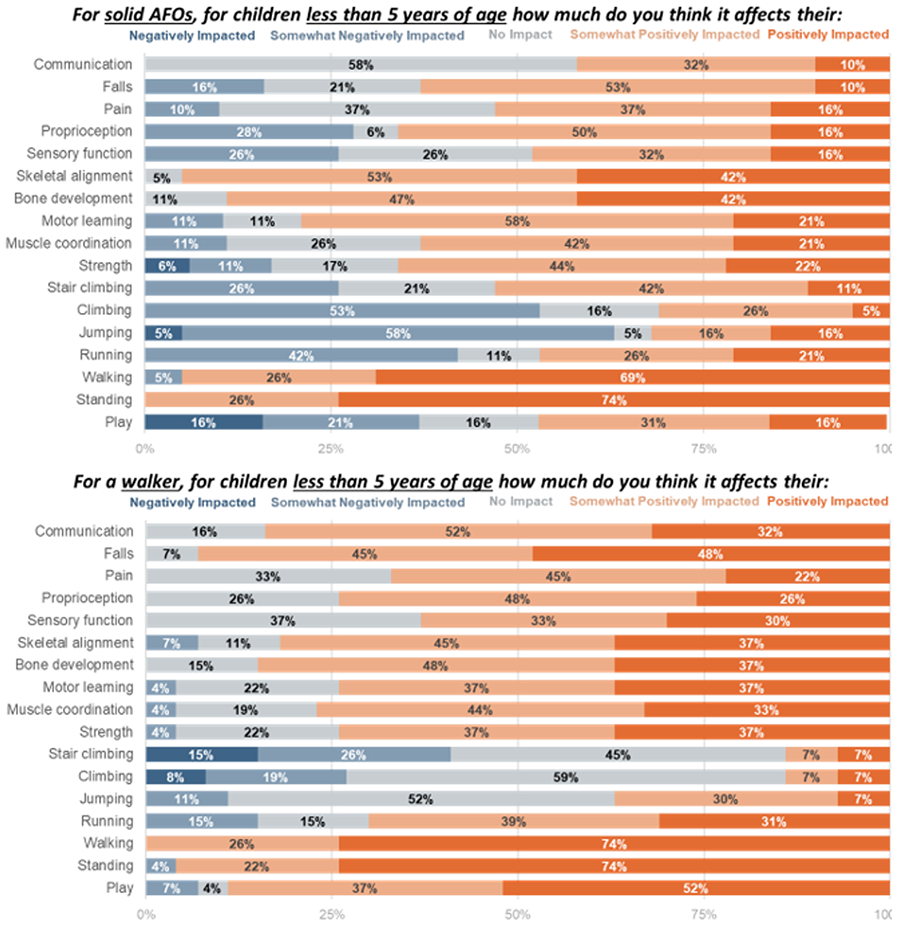
From the parent perspective, AFOs generally had a positive effect on walking and standing, with limited impact on jumping, climbing, stair climbing, and communication. While we were able to establish some trends across participants, it is important to note that this is a diverse population with diverse experiences. For example for pain where positive impact means a reduction in pain and a negative impact means an increase in pain; one parent noted that pain was very negatively impacted by AFOs, one stated that they were somewhat positively impacted pain, and the third parent said they saw no impact on pain from AFOs. The parent experiences were emphasized in open ended responses, for example:
"As my son has gotten older, we have seen greater benefit from his AFOs. We have finally seen the stretch in the hamstrings, and they provide stability when he stands."
Meanwhile, clinicians specifically highlighted that while AFOs were seen to positively impact walking, standing, skeletal alignment, and bone development they were seen as barriers to climbing, running, jumping, and play (Figure 1). While walkers were seen as positively impacting walking, standing, play, and falls they presented barriers to stair climbing and jumping. Only 4 and 6 clinicians respectively responded about the impacts of hinged AFOs and SMOs, so they are not included in Figure 1.
Clinician education and training influences the prescription process
Clinicians reported receiving a wide range of training on mobility aids. For some clinician participants, their training consisted of one survey course during their graduate studies. Other training included from a specific vendor or company, on-the-job experiences, and conference workshops. The amount of training may influence what clinicians consider when prescribing a specific device that has a large long-term impact for the patient.
Clinicians considered a large variety of factors during the prescription process, and these factors vary between clinicians. For a child's first orthoses, clinicians consider function level (10), family interest (7), musculoskeletal problems (7), and goals (6). For walkers clinicians consider the family's car (2), home environment (6), and support required (6). One physical therapist mentioned the nuances of their decision process:
"I think of like, sometimes it's like do we wait and see? Or do we be more proactive now? And I tend to be more proactive now thinking about future musculoskeletal issues that might come into play because of their alignment."
Our results suggest that there is inconsistency with who is driving decision-making in regard to device provision and type. In some scenarios it is a joint decision, driven by the parents, driven by one clinician, or driven by multiple clinicians working together.
"You know if the child that I'm working with is one of many children in the home and the parents are working and or really busy, and I feel like compliance is going to be a big problem, I might think twice before even broaching the conversation with the family [to recommend a child's first AFO]."
DISCUSSION AND CONCLUSIONS
Perceptions and experiences of the provision and use of first mobility aids such as AFOs and walkers are complex and multifactorial, with significant variation depending on family goals and motivation, clinician philosophy, and more straightforward variables such as the child's diagnosis and functional needs.
For example, one particularly notable result is how the power dynamic between clinicians and families varies between clinicians, having critical implications to if and what type of device is prescribed to the child. Additionally, who is making the final decision varied between clinicians and clinic settings. The philosophy varied such as family driven, where the clinicians provide all information and it is the families decision based on their goals if a device is prescribed and used, while other scenarios included the clinician driving the decision making while still educating the family on the options and why a specific device was chosen.
Limitations of this study included: a large majority of participants were from Washington state due to our recruitment methods and parent perspectives are only represented by survey data at this point. We have plans to conduct parent interviews in the future. Further, only limited perspectives were shared about hinged AFOs and SMOs as these were not employed as frequently as solid AFOs or walkers.
These results are important for understanding the process of how children with CP receive their first mobility aid and have important implications for provision process improvement. Examples of such improvements include better communication, "wraparound" care with the entire team of clinicians that must work together to get a child's mobility aid, smoothing the process with insurance companies, and timeliness of delivery of device after prescription. More research is needed to determine the best interdisciplinary solutions to address these highlighted areas in need of improvement.
REFERENCES
[1] Odding E, Roebroeck ME, Stam HJ. The epidemiology of cerebral palsy: Incidence, impairments and risk factors. Disabil Rehabil 2006; 28: 183–191.
[2] Colver A, Fairhurst C, Pharoah POD. Cerebral palsy. The Lancet 2014; 383: 1240–1249.
[3] Palisano RJ, Hanna SE, Rosenbaum PL, et al. Probability of walking, wheeled mobility, and assisted mobility in children and adolescents with cerebral palsy. Dev Med Child Neurol 2010; 52: 66–71.
[4] Østensjø S, Carlberg EB, Vøllestad NK. The use and impact of assistive devices and other environmental modifications on everyday activities and care in young children with cerebral palsy. Disabil Rehabil 2005; 27: 849–861.
[5] Thomas DR. A General Inductive Approach for Analyzing Qualitative Evaluation Data. Am J Eval 2006; 27: 237–246.