Fani N. Lee![]() 1
1![]() , Heather A. Feldner
, Heather A. Feldner![]() 2
2![]() , Kelly Hsieh
, Kelly Hsieh![]() 1
1![]() , Fabricio Balcazar
, Fabricio Balcazar![]() 1
1![]() , Brenda Sposato Bonfiglio
, Brenda Sposato Bonfiglio![]() 1
1![]() , Sarah Parker Harris
, Sarah Parker Harris![]() 1
1![]()
![]() 1
1![]() Department of Disability and Human Development, University of Illinois Chicago;
Department of Disability and Human Development, University of Illinois Chicago; ![]() 2
2![]() Department of Rehabilitation Medicine, University of Washington
Department of Rehabilitation Medicine, University of Washington
INTRODUCTION
Rehabilitation scholarship has demonstrated that theoretical frameworks are necessary in establishing experimentation structure, as they not only set the tone of the research but also serve as a foundation for interpreting results and disseminating knowledge.[1] The use of theory is especially important in research involving people with disabilities (PWD) because of their historical objectification and marginalization in society, which includes assistive technology (AT) processes.[2] Despite increased citation of social theory in evidence-based AT research, there continues to be a gap in integrating AT conceptual models in research design, data analysis, and results interpretation.[1] Meaningful integration of theory into practice is the essential next step in generating socially-responsive research that addresses AT consumer needs and moves the field forward. This paper proposes that AT research must merge biophysical and social theory in a way that conveys the interconnection of factors impacting AT users' experiences, values, participation, and quality of life. To accomplish this task, two pre-existing AT models, the Human Activity Assistive Technology model (HAAT) [3] and the interdependence frame for AT [4] have been merged into a novel model, the interdependence-HAAT model (i-HAAT), to provide a contemporary approach for constructing, interpreting, and translating AT outcomes research.
OBJECTIVE
The purpose of this paper is to demonstrate the utility of the i-HAAT as a theoretical framework in AT outcomes research. First, this article will explain the importance of theory in AT research. Then, each conceptual framework will be discussed, both individually and as a merged unit. Finally, the application of the merged framework to the authors' study population of former long-term nursing home residents using AT in the community will serve as an example for how this framework can guide AT research design and result interpretation.
BACKGROUND
Current evidence-based practice (EBP) mandates have contributed to a dissonance between theory and practice, where evidence is applied without contemplation of its theoretical foundation.[1] The underutilization of theory in AT research has diminished the ability to "…identify and refine conceptual relationships among interventions and between populations, and to develop a systematized knowledge base."[1, p. 131] Additionally, the scarcity of theoretically-framed research leaves a gap in the AT field that allows for the predominant medicalized view of disability to guide EBP without regard to its underlying effects on PWD [2] or consideration of the trajectory of the field. This paper argues that AT research must be framed by a theoretical model that emphasizes the personal and contextual factors contributing to societal exclusion, acting as a springboard for reform.
The Human Activity Assistive Technology model
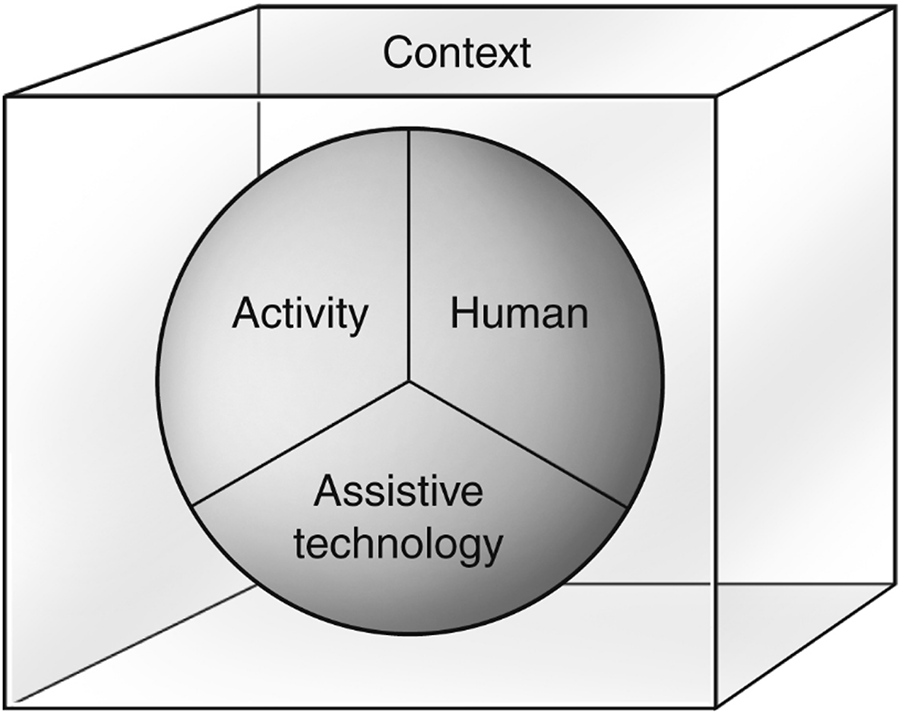
The Human Activity Assistive Technology (HAAT) model [3] is recognized as the founding theoretical model of AT. It is visually represented as a three-dimensional sphere consisting of equal parts human, activity, and AT housed within a contextual cube (Figure 1). Although seemingly simplistic in its structure, each HAAT factor bears significant weight and consideration as a system. The 'human' represents an individual's physical, emotional, cognitive, and sensory skills used in activity participation, as well as their life roles, technology experience, motivation, and lifespan considerations.[3] 'Activity' in the HAAT model considers the task(s), task demands, and the contextual influencers of participation in life situations.[3] 'Assistive technology' is described as a device that enables activity performance, which includes the continuum of technology complexities as well as the consideration of the human/technology interface impacting AT selection and use.[3] 'Context' includes the physical, social, cultural, and institutional landscapes that shape AT use.[3] Conceptualizing AT use as an interrelated system takes into consideration the complex relationships contributing to participation, integration, and well-being.
An interdependence frame for assistive technology
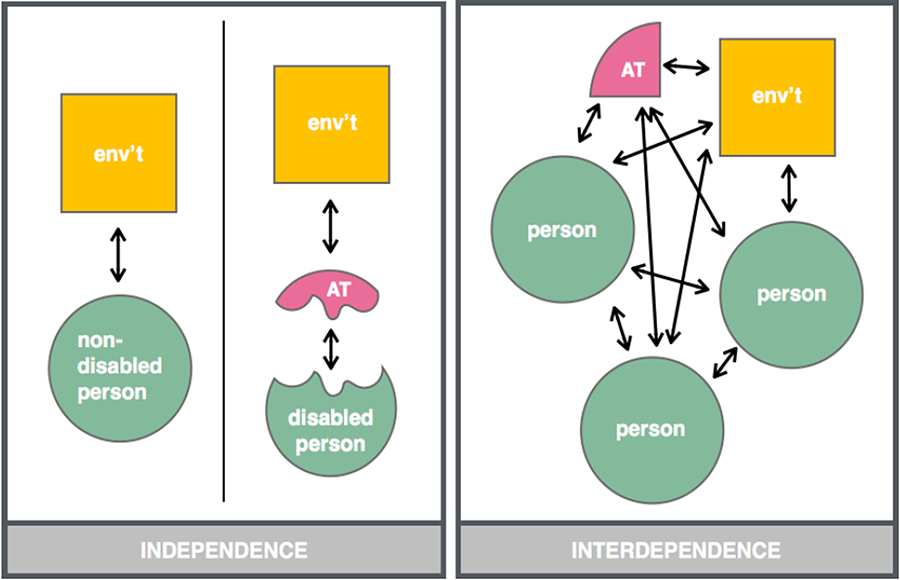
The interdependence frame for AT [4] illustrates the multiple interactions between people, AT, and the environment without specific identification of a single AT user (Figure 2). This contrasts to the independence frame commonly utilized in rehabilitation research examining the effectiveness of AT in improving functional independence and participation in specific daily activities. [5] The interdependence frame reasons that although AT is prescribed for an individual, it is utilized by many people within the original user's social group to facilitate participation.[4] This view stems from literature examining the interactional nature of community living for many PWD that has demonstrated both the value of independence in decision-making and self-directed activity engagement, as well as the importance of interdependence in the form of support from family/friends, personal care assistant(s), and community services.[5] Community living scholars have recognized that for PWD to live well in their communities, interdependence should be recognized as an integral component of well-being that is incorporated within infrastructural supports.[5]
APPROACH
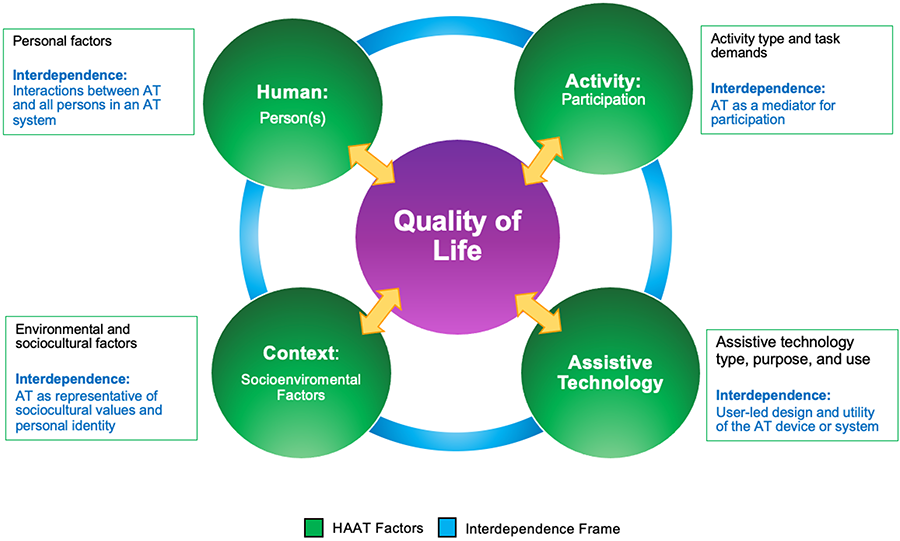
The i-HAAT, a framework constructed by merging the HAAT model and the interdependence frame for AT, incorporates factors impacting AT outcomes and examines the interactional aspects of those factors through an interdependence lens (Figure 3). It is worth noting that quality of life (QoL) has been added to the framework because of its identification as a critical variable in AT outcomes research.[6] However, research using the i-HAAT model is not required to report on QoL outcomes. When applying this model to AT outcomes inquiry, the researcher selects the outcome factor(s) to be measured (e.g., AT use/abandonment, AT satisfaction, AT efficacy/impact, functional performance, cost analysis, psychosocial impact, etc.), and the framework serves as a guide for considering domain factors that may impact the outcome factor(s). In this way, the model can be adapted and applied to various AT outcome inquiry projects.
The human domain denotes the individual person issued the AT and any other person(s) within their environment utilizing or interacting with the AT. The shared interaction surrounding AT within the human domain is an important consideration in AT outcomes research, especially as related to the impact this interdependence has on the successful use and overall satisfaction with the AT. The activity domain represents participation factors as they are perceived by the primary AT user, including the aspects of activity that yield internal outcomes such as feelings of independence, role fulfillment, and productivity. Interdependence in the activity domain emphasizes autonomy rather than completing tasks without assistance.[4] In the AT domain, interdependence emphasizes AT consumer involvement in all aspects of AT design, delivery, and use to counter traditionally disempowering AT systems.[7] The context domain acknowledges that AT holds meaning and purpose in one's life, helping to negotiate participation and societal inclusion, and contributing to personal conceptualizations of identity.[7]
Application of the i-HAAT Model to community re-integration outcomes research
To demonstrate the customizability of the i-HAAT Model, an example of its application in a research study investigating the outcomes of former long-term nursing home residents using AT in the community is illustrated (Figure 4). The process begins with quantitative variable identification and categorization and is followed by establishing interconnectivity between domain variables. Finally, the model is used to frame examination of infrastructural supports for deinstitutionalized AT users.
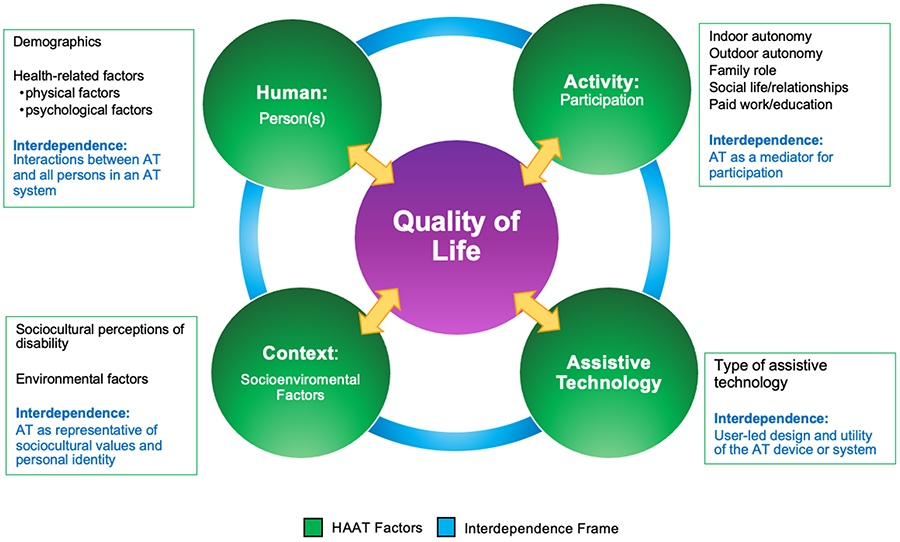
This study employed an explanatory sequential mixed methods approach, where quantitative survey data was explained using subsequent qualitative interview data.[8] Variables theorized as contributing to participation and QoL outcomes were identified using a mix of researcher-generated surveys and standardized measures. Researcher-created surveys identified demographic variables within the human domain and AT factors within the AT domain (Figure 4). The World Health Organization (WHO) Quality of Life-Brief Form [9] captured health-related factors in the human domain, environmental factors in the context domain, and QoL in the central domain. The WHO Disabilities Module [10] measured the sociocultural perceptions of disability in the context domain. The Impact on Participation and Autonomy questionnaire [11] measured participants' indoor and outdoor autonomy, family roles, social relationships, and work/education in the activity domain.
Study findings demonstrated a positive correlation between participation and QoL. When visualizing the results within the i-HAAT diagram, it became evident that at least one factor from each domain impacted participation and QoL outcomes for the study participants, exemplifying the meaning of an interactional AT system. Therefore, it was concluded that the state-funded program overseeing community transition could more effectively contribute to successful individual outcomes by using the i-HAAT model domains as a guide. Specifically, a person's wants, needs, and lived experiences which were outlined in the human domain were more likely to be identified and supported during transition planning when each i-HAAT domain was addressed. Transition care planning that incorporated consideration of contextual elements (i.e., environment, resources, and positive relationships), activities with meaningful outcomes, and AT supporting activity engagement had the potential to positively impact a person's autonomy, self-efficacy, health, values/purpose, participation, and quality of life.[12]
CONCLUSION
This paper argues that to move the field forward towards socially-responsive research, theoretical framing of inquiry must take precedence in AT outcomes inquiry. The use of the i-HAAT model as a conceptual foundation and pragmatic structural frame for AT outcome research processes from design to result interpretation may help this endeavor. As applied to research investigating the role of AT in the lives of former long-term nursing home residents, the i-HAAT model assisted in categorizing quantitative variables, visualizing the interactional elements influencing participation and QoL outcomes, and identifying areas of program-level change that may impact successful community living. The i-HAAT model demonstrates potential value in today's scholarship and practice because it presents a field-forward approach to AT outcomes research. Additional research using this model is necessary across methodologies and populations to hone its application and significance.
References
[1] Lenker, J. A., Fuhrer, M. J., Jutai, J. W., Demers, L., Scherer, M. J., & DeRuyter, F. (2010). Treatment theory, intervention specification, and treatment fidelity in assistive technology outcomes research. Assistive Technology, 22(3), 129-138.
[2] Ripat, J. D., & Woodgate, R. L. (2011). Locating assistive technology within an emancipatory disability research framework. Technology and Disability, 23(2), 87-92.
[3] Cook, A.M., Polgar, J.M., & Encarnação, P. (2020). Assistive technologies: Principles and practice. St. Louis, Mo.: Mosby Elsevier
[4] Bennett, C. L., Brady, E., & Branham, S. M. (2018). Interdependence as a frame for assistive technology research and design. Proceedings of the 20th International ACM SIGACCESS Conference on Computers and Accessibility, 161–173.
[5] White, G. W., Lloyd Simpson, J., Gonda, C., Ravesloot, C., & Coble, Z. (2010). Moving from Independence to interdependence: A conceptual model for better understanding community participation of centers for independent living consumers. Journal of disability policy studies, 20(4), 233–240.
[6] De Jonge, D., & Stevens, W. (2016). Capturing the true value of assistive technologies to consumers in routine outcome measurement. Technologies, 4(4), 35.
[7] Ravneberg, B., & Söderström, S. (2017). Disability, society and assistive technology. Taylor & Francis.
[8] Creswell, J.W., & Plano Clark, V.L. (2018). Designing and conducting mixed methods research (3rd ed.). Los Angeles: SAGE.
[9] Harper, A., Power, M., & The WHOQOL Group. (1998). Development of the World Health Organization WHOQOL-BREF Quality of Life Assessment. Psychological medicine, 28(3), 551–558.
[10] Power, M. J., Green, A. M., & THE WHOQOL-DIS Group. (2010). Development of the WHOQOL disabilities module. Quality of life research, 19(4), 571–584.
[11] Cardol, M., de Haan, R. J., van den Bos, G. A. M., de Jong, B. A., & de Groot, I. J. M. (1999). The development of a handicap assessment questionnaire: The Impact on Participation and Autonomy (IPA). Clinical rehabilitation, 13(5), 411–419.
[12] Mills, W. L., Snow, A. L., Wilson, N. L., Naik, A. D., & Kunik, M. E. (2013). Conceptualization of a toolkit to evaluate everyday competence in planning transitions from nursing homes to the community. Journal of the American medical directors association, 14(8), 626.e1-626.e7.