Cardiovascular load of using a walker-based exoskeleton in children with cerebral palsy
Katie M. Landwehr-Prakel1, Anna M. Fragomeni2, Kristie F. Bjornson3, Chet T. Moritz2,4, Heather A. Feldner2, Katherine M. Steele1
1Department of Mechanical Engineering, University of Washington, 2Department of Rehabilitation Medicine, University of Washington 3Seattle Children’s Research Institute, 4Department of Electrical and Computer Engineering, University of Washington
Introduction
Cardiovascular fitness is critical for all children and adults to support health and participation. For a multitude of reasons, children with cerebral palsy (CP) experience reduced physical activity levels, which ultimately affects their health and function [1]. To address this gap in physical activity, mobility aids, such as orthoses, gait trainers, or walkers can be used. These aids are especially important for children with CP in Gross Motor Functional Classification Systems (GMFCS) Levels III-V who often use these devices for daily activities.
Over the past decade, there has been increased use of exoskeletons in adult rehabilitation. However, their development, access, and associated clinical experience for pediatric populations remains largely unexplored [2]. The Trexo exoskeleton (Trexo Robotics, Mississauga ON) is one example of a mobility aid that has been recently developed to support training and activities of daily living for children with CP. The Trexo is a battery-powered exoskeleton mounted to the frame of a commonly used Rifton gait trainer that generates a stepping pattern using hip and knee actuation. The Trexo supports walking at rates of 10-70 steps/minute and can be set in two different modes: endurance and strength. The Trexo has been evaluated for in-home use and shown to improve sleep and bowel function within the first month of use [3, 4]. Currently, there have been only two studies [5, 6] examining feasibility and effects of Trexo use across a broad set of outcome measures.
Whether and how exoskeletons like the Trexo may support cardiovascular function and fitness remains unknown. Depending on the rehabilitation goal, mobility aids may be used to increase or decrease cardiovascular load. Understanding the cardiovascular load during exoskeleton use is important for optimizing utility and outcomes. Evaluating how cardiovascular loads vary with speed, mode, or other settings can be used to optimize device settings, such as to decrease load to support community participation and longer walking bouts or increase load for an intensive training session. However, the impact of mobility aids on cardiovascular load is rarely assessed, especially in children with CP. Prior studies have examined cardiovascular demands with other exoskeletons but have been limited to adults with spinal cord injuries [7].
One way to measure cardiovascular load is through heart rate (HR). HR can be measured over time as an indirect indicator of physical activity, providing a measure of the relative stress placed on the cardiopulmonary system due to physical exertion [8]. Prior research has used the heart rate reserve (HRR) based on heart rate to evaluate exercise intensity. HRR has been shown to reflect the rate of energy expenditure during physical activity [9] and has been recommended for use in estimating intensity of activities of daily living.
The purpose of this study was to quantify how heart rate changes during Trexo use in children with CP. We hypothesized that HR would: 1) increase during Trexo use, 2) be higher in Strength versus Endurance mode, and 3) increase with higher Trexo Percent Initiation, an estimate from the exoskeleton of a user’s contribution.
Methods
Participants: Four children with CP (1M/3F, age: 32 ± 8.0 months) who were GMFCS Levels III-V participated in this study. This study was approved by the University of Washington Institutional Review Board (STUDY00014877) and registered at ClinicalTrials.gov (#NCT05520359). Exclusion criteria included contraindications for weight bearing activities, orthopedic surgery of the lower extremities or neurosurgery within the last 12 months, or botulinum toxin injections of the lower extremities within the last 6 months.
Data Collection: Participants completed up to 6 visits of walking with the Trexo (Figure 1). Each visit consisted of multiple sessions at varying speeds (steps/min), and modes (Strength or Endurance). Each session was at a fixed speed. Speed, mode, and the length of each session were determined by the researcher, physical therapist, and caregiver by monitoring the child’s comfort and engagement.
For each participant, Trexo parameters were determined at an initial enrollment visit. The Trexo leg lengths were determined by taking measurements from the participant’s hip-to-knee and knee-to-floor, respectively. The range of motion of the hip and knee joints were determined by moving each leg through its full passive range in the device. Trexo Support Force, dictating the torque applied by the hip and knee actuators, was determined by starting at the lowest level of support, and if needed, increasing until a successful stepping pattern was achieved. In Endurance mode, the Trexo provided full assistance to the user, moving the user’s legs through a defined hip-knee kinematic pattern without requiring contribution from the user. In Strength mode, the Trexo provides greater delay to await initiation of a step from the user.
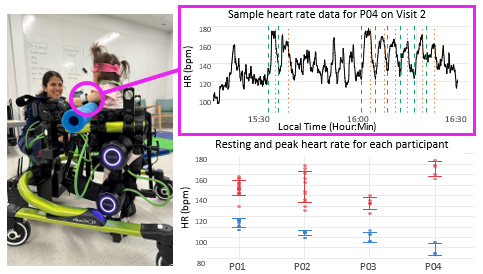
Outcome Measures: Heart rate (HR) was collected throughout each visit using a Polar OH1 Optical Heart Rate Sensor (Polar Electro Oy, Kempele, Finland) at a frequency of 1 Hz. Resting Heart Rate (HRRest) was determined at the beginning of each visit as the lowest HR averaged over a period of 10 seconds prior to walking with the Trexo. Peak Heart Rate (HRPeak) was the highest HR averaged over a 10 second period during each session. Age predicted Maximum Heart Rate (HRMax) was quantified as [10].
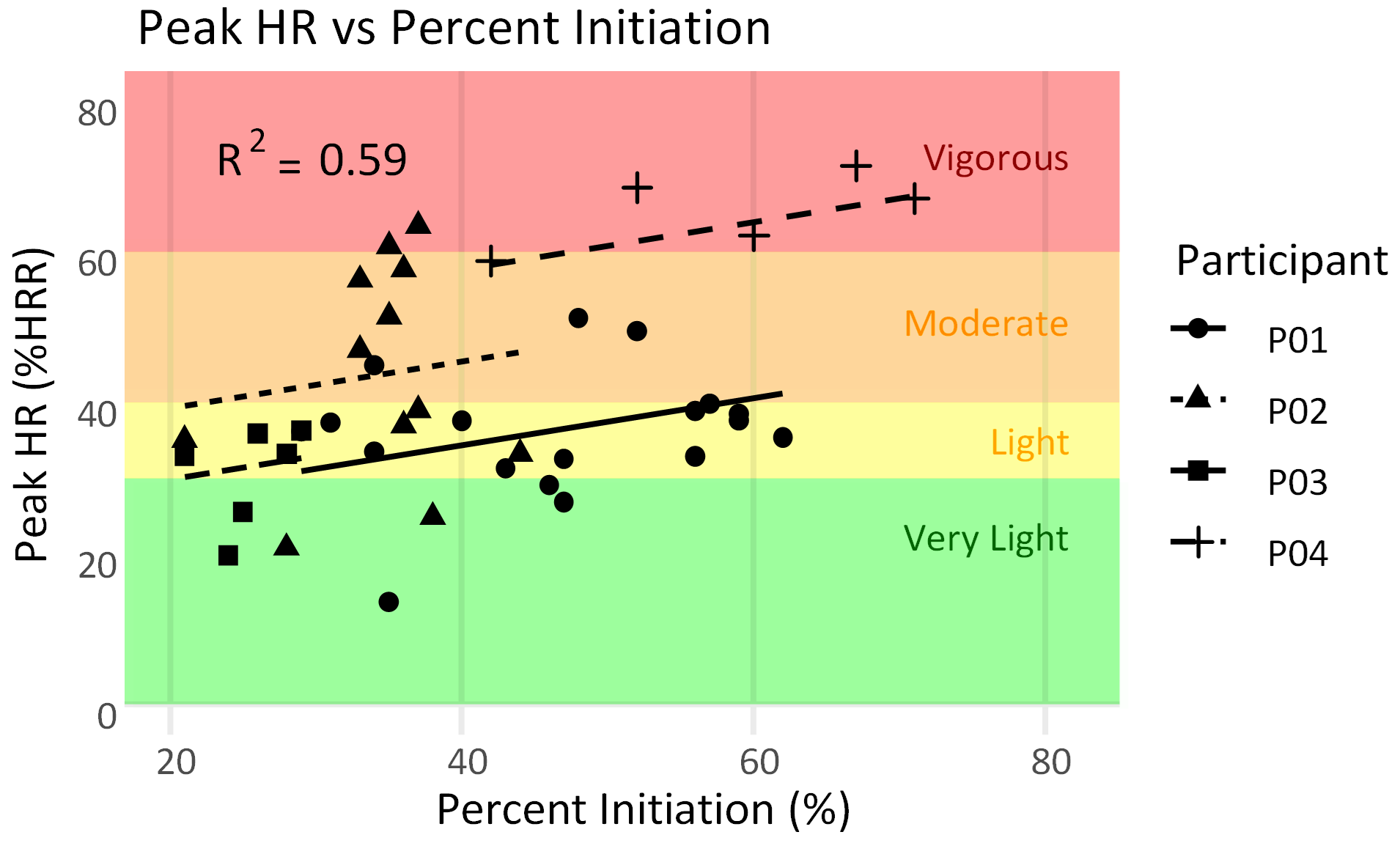
Heart Rate Reserve (HRR) was used to normalize HR across participants and visits. HRR is a measure derived as the difference between HRMax and HRRest and is used to gauge exercise intensity [9]. Percentage of HRR (%HRR) was calculated as (HRPeak-HRRest)/(HRMax-HRRest)×100.
To quantify user contribution, we evaluated the Percent Initiation for each session. Percent Initiation is a metric quantified by Trexo that uses the motor hip torques to estimate the user’s contribution. Since this measure is reported for each limb, we analyzed Percent Initiation for the more-affected side, determined as the side with more muscle spasticity measured from the Modified Ashworth Scale (MAS) from the hamstrings, quadriceps, gastrocnemius, and soleus muscles.
Analysis: All analyses were conducted using R version 4.1.1 [11]. Descriptive statistics were used to summarize participant characteristics and HRPeak with varying Trexo mode. A linear mixed effects model was used to evaluate whether HRPeak varied with Percent Initiation. For this model, we used the lme4 package [12] with random effects for participants. Conditional R2 values were calculated using the MuMIn package [13] to report the variance explained by the entire model, including fixed and random effects.
|
Heart Rate Summary |
|||||||
|
ID |
Age (mo) |
Sex |
Visits |
Resting |
Peak |
HRR |
|
|
P01 |
23 |
F |
6 |
112.3 ± 3.9 |
147.4 ± 6.7 |
94.4 ± 3.9 |
|
|
P02 |
42 |
M |
2 |
102.2 ± 3.9 |
148.5 ± 14.8 |
103.3 ± 3.9 |
|
|
P03 |
29 |
F |
3 |
101.9 ± 5.4 |
132.8 ± 5.6 |
104.4 ± 5.4 |
|
|
P04 |
34 |
F |
2 |
89.7 ± 7.5 |
165.5 ± 7.4 |
116.3 ± 7.5 |
|
Results
All participants completed 2-6 visits of walking in the Trexo (Table 1) with sessions of varying speeds (steps/min) and modes (Strength or Endurance). HRRest of all participants across all visits ranged from 74-115.5 bpm (97.6 ± 5.9).
Heart rate increased from baseline with Trexo use for all participants and all sessions. HRPeak across all sessions ranged from 123.1-174.3 bpm (148.6 ± 5.7), which equated to an %HRR of 19.8-71.4%. HRPeak was generally higher in Strength versus Endurance mode. The average HRPeak in Strength mode ranged from 146.5-163.3 bpm (154.6 ± 8.4) versus 132.5-174.3 bpm (147.53 ± 19.7) in Endurance mode. HRPeak was positively correlated with sessions with higher user contribution as measured by Percent Initiation (R2 = 0.59, Figure 2).
Discussion
We sought to investigate whether toddlers with CP increased heart rate while using the Trexo to potentially support fitness and cardiovascular health. Three of four participants had significant increases in HR to moderate or vigorous levels of activity relative to their resting heart rate. This increase in HR was greater than other studies that have assessed the effect of mobility activities on cardiovascular load in CP. Aurich-Schuler et al. (2017) assessed HR during Lokomat use in children with neurological disorders and reported a trend of increasing HR with less Lokomat assistance, but did not report HR relative to resting rates [14]. To mimic activities of daily living, Israeli-Mendlovic et al. (2014) measured HR among children with CP GMFCS IV-V (6 to 12 years) while performing Gross Motor Functional Measure (GMFM) assessments. Participants performed their most challenging skill achieved from the GMFM for 2 minutes with an average heart rate of 127.3 ± 21.9 [15].
The resting heart rates of the children in this study (97.6 ± 5.9) were similar to those prior literature for children with CP, which report resting rates of 93.9 ± 17.1 (GMFCS I and II) and 100.7 ± 10.2 bpm (GMFCS IV and V) [15, 16]. Limited research has investigated heart rates for children or adults with CP in GMFCS Levels IV and V. Given the prevalence of cardiovascular disorders in this population, understanding whether or how daily activities and assistive technology can support fitness and cardiovascular health are important areas for future research.
We found that HRPeak generally increased in Strength versus Endurance mode. Endurance mode was designed to support walking practice by moving the limbs through a defined kinematic pattern. Strength mode was designed to increase difficulty by encouraging the user to produce torque at the hip to initiate a step. This is similar to the findings of Aurich-Schuler et al. (2017) using the Lokomat, where they observed a trend that heart rate increased with increased difficulty across modes, although these results were not statistically significant [14].
We did not find significant associations in HRPeak with speed. This could be attributed to the fixed range of speeds available on the Trexo (10-70 steps/min) and our small number of participants who could complete sessions at multiple speeds in both modes.
This preliminary study demonstrated that the Trexo may support elevated HR for fitness or cardiovascular training among young children with CP in GMFCS Levels IV-V. Limitations of this study include the limited sample size and number of trials at each speed and mode. Further, the estimates of age-adjusted maximum HR for calculating HRR may overestimate HRR for young children, suggesting exercise intensity may be even higher for these children. Future research that evaluates the generalizability of these findings and compares HR of young children with CP across activities of daily living and different rehabilitation protocols are critical to understand and support long-term cardiovascular health and fitness in this population.
Acknowledgements
This work was supported by the Seattle Children’s Hospital CP Research Fund. We would like to thank the participants and their families for their time and participation, as well as Kevin Doherty-Regalia, Avni Sisodiya, and Grace O’Connor for their assistance with data collection.
References
[1] Fowler EG et al. Promotion of Physical Fitness and Prevention of Secondary Conditions for Children with Cerebral Palsy: Section on Pediatrics Research Summit Proceedings. Phys Ther 2007;87:1495–510.
[2] Fosch-Villaronga E et al. Promoting inclusiveness in exoskeleton robotics: Addressing challenges for pediatric access. Paladyn J Behav Robot 2020;11:327–39.
[3] Diot CM et al. Robot-Assisted Gait Training with Trexo Home: Users, Usage and Initial Impacts. Children 2023;10:437.
[4] Diot CM et al. Robotic lower extremity exoskeleton use in a non-ambulatory child with cerebral palsy: A case study. Disabil Rehabil Assist Technol 2021;18:497–501.
[5] McCormick AM et al. A randomized, cross-over trial comparing the effect of innovative robotic gait training and functional clinical therapy in children with cerebral palsy; a protocol to test feasibility. Contemp Clin Trials 2023;127:107086.
[6] Bradley SS et al. Physiotherapy-assisted overground exoskeleton use: Mixed methods feasibility study protocol quantifying the user experience, as well as functional, neural, and muscular outcomes in children with mobility impairments. Front Neurosci 2024;18:1398459.
[7] Shackleton C et al. Effectiveness of over-ground robotic locomotor training in improving walking performance, cardiovascular demands, secondary complications and user-satisfaction in individuals with spinal cord injuries: A systematic review. J Rehabil Med 2019;51:723–33.
[8] Rowlands AV et al. Measurement of Physical Activity in Children with Particular Reference to the Use of Heart Rate and Pedometry. Sports Med 1997;24:258–72.
[9] Swain DP, Leutholtz BC. Heart rate reserve is equivalent to VO2 Reserve, not to VO2 max. Med Sci Sports Exerc 1997;29:410.
[10] Gellish RL et al. Longitudinal Modeling of the Relationship between Age and Maximal Heart Rate. Med Sci Sports Exerc 2007;39:822.
[11] R Core Team. R: A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing; 2024.
[12] Bates D et al. Fitting Linear Mixed-Effects Models Using lme4. J Stat Softw 2015;67:1–48.
[13] Bartoń K. MuMIn: Multi-model inference. R package version 1.48.4. 2024.
[14] Aurich-Schuler T et al. Can Lokomat therapy with children and adolescents be improved? An adaptive clinical pilot trial comparing Guidance force, Path control, and FreeD. J NeuroEng Rehabil 2017;14:76.
[15] Israeli-Mendlovic H et al. Heart rate and heart rate variability parameters at rest, during activity and passive standing among children with cerebral palsy GMFCS IV–V. Dev Neurorehabil 2014;17:398–402.
[16] Amichai T et al. Cardiac Autonomic System Response to Submaximal Test in Children with Cerebral Palsy. Pediatr Phys Ther 2017;29:125.