Stowable Passive Supernumerary Dorsal Grasping
Derrick Ma*1,2, Jungyo Lee*1, Andrew I.W. McPherson*1, Hannah S. Stuart1
1Embodied Dexterity Group, University of California, Berkeley
2California Institute of Technology
INTRODUCTION
Neuromuscular injuries and disorders can severely impair one's ability to move or perform daily tasks. Spinal cord injury (SCI) at the cervical level is the most common category of SCI, often resulting in tetraplegia [1]. This condition significantly impairs motor and sensory functions in the upper limbs, leading to a diminished quality of life due to the loss of critical abilities required for activities of daily living (ADLs), such as grasping and manipulating objects. Regaining hand and arm function is a top priority for individuals with cervical SCI, as consistently highlighted in surveys [2,3].
One approach to mitigate this lost function is through the use of assistive devices. Despite the variety of available assistive technologies, there is a high rate of abandonment among users, particularly with active devices [4] due to several factors such as expectation mismatches between users' needs and device capabilities, the device's weight making it cumbersome to use, unintuitive control schemes that are difficult to learn, aesthetic concerns, challenges associated with independently donning and doffing devices, and the psychological burden of using a highly mechanized device [5,6]. Therefore, devices with simple designs and intuitive usages can help fill this gap.
In this paper, we introduce the Passive Dorsal Grasper, a lightweight and seamless assistive wearable device that leverages the residual active wrist extension of individuals with C5–C7 spinal cord injuries to facilitate grasping tasks. Unlike previous active devices [7,8], this electronics-free device harnesses existing wrist movements without the need for external power, addressing common issues related to active assistive technologies. The Passive Dorsal Grasper allows users to independently don and doff the device, stow the fingers out of the way when unused, and is not sensitive to hand morphology or finger contractures, potentially reducing abandonment rates.
METHODS
The Passive Dorsal Grasper
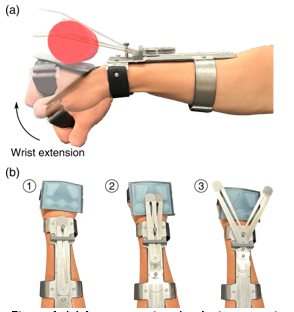
The Passive Dorsal Grasper is an unpowered assistive device designed to allow individuals with C5-C7 spinal cord injuries who retain some voluntary wrist extension to grasp objects with the back of their hand. The device features two deployable aluminum fingers that rest at a 20-degree angle above the dorsal plane of the hand when aligned with the forearm and are bent at the tips. These fingers provide a grasping surface against which objects can be secured, as shown in Figure 1(a). The overall weight of the device is 148.36 g. The base of the fingers is mounted on a deployment carriage and linear rail system integrated into a forearm baseplate for ease of deployment/retraction (Figure 1(b)). The device is attached to the forearm of the user by two combination metal and Velcro cuffs. Additionally, an artificial palm component made of silicone protects the thinner skin on the back of the hand and provides increased contact friction for grasping. This artificial palm is separate from the rest of the device being held in place with a Velcro strap between thumb and forefinger and across the palm.
Grip Strength Measurement
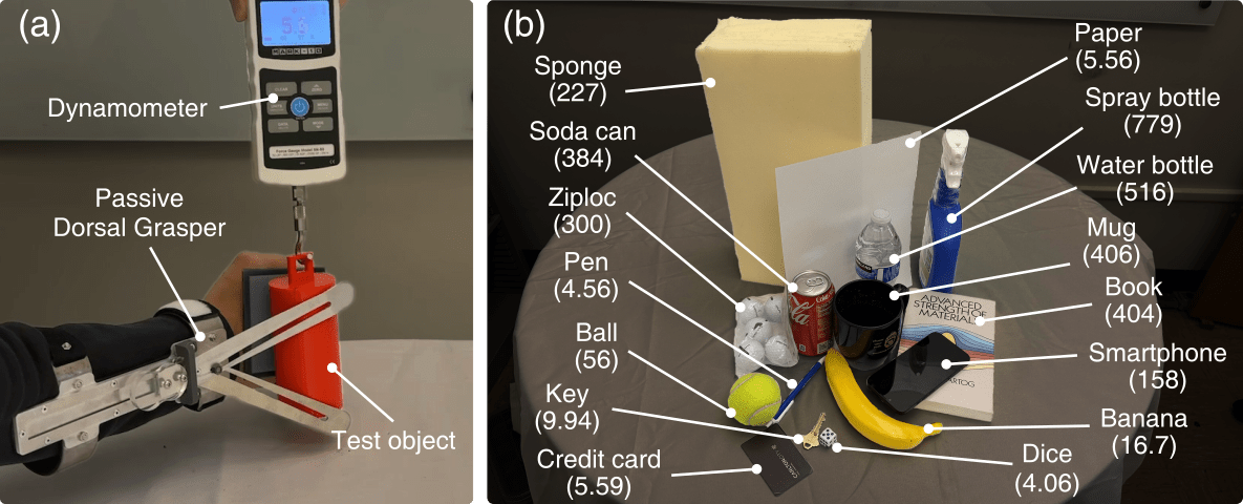
To measure maximum palmar grip strength, 3D printed cylinders with diameters varying from 40 mm to 70 mm were prepared. Additionally, a plastic key card to simulate a credit card was added as a test object. We used the device to secure each object in an opisthenar grasp with the flat sides of the baseplate perpendicular to the ground, after which a force gauge was used to pull the objects vertically upwards as shown in Figure 2(a). Each trial ended when the object began to slip against the artificial palm or the fingers, recording the peak force experienced during the trial. The test was performed for 8 trials with each object for three different finger design variants, with the author exerting the maximum possible wrist extension force.
ADL Grasp and Manipulation Test
In order to evaluate the range in geometry of objects encountered in ADL that the Passive Dorsal Grasper can successfully manipulate, a modified Grasp and Release Test (GRT) was performed by an author. Fifteen objects were chosen for this test, shown in Figure 2(b). As with the grip strength testing, each of the three sets of fingers were tested across the range of objects, with at least 10 trials being conducted for each one. Each trial began with the object being placed in a starting area on a table in front of the shoulder of the arm wearing the Passive Dorsal Grasper. A 30 second timer was started, during which the researcher performing the task attempted to pick up the object using the device. If successful during the time-period, the researcher then attempted to supinate and pronate the hand while maintaining a firm grasp on the object. The success or failure of the two subtasks, denoted “grasp” and “manipulation," respectively, were recorded for each trial.
RESULTS
Grip Strength Measurement
The grasp force measurements across the four cylindrical objects and the flat key card using the Passive Dorsal Grasper are shown in Figure 3(a). The results reveal a decreasing trend in grasp forces as the cylinder diameter increases. Specifically, the grasp forces recorded are 35.8 ± 3.39 N, 33.2 ± 2.05 N, 29.9 ± 1.67 N, and 23.1 ± 2.48 N for the 40 mm, 50 mm, 60 mm, and 70 mm cylindrical objects, respectively. For the flat credit card, the grasp force is significantly lower, measuring 9.71 ± 1.93 N - less than half the grasp force achieved with the 70 mm cylindrical object. This reduction in grasp force for the credit card is likely due to the minimal contact area with the single fingertip and the limited ability of the passive grasper to stabilize such a thin, flat object.
ADL Grasp and Manipulation Test
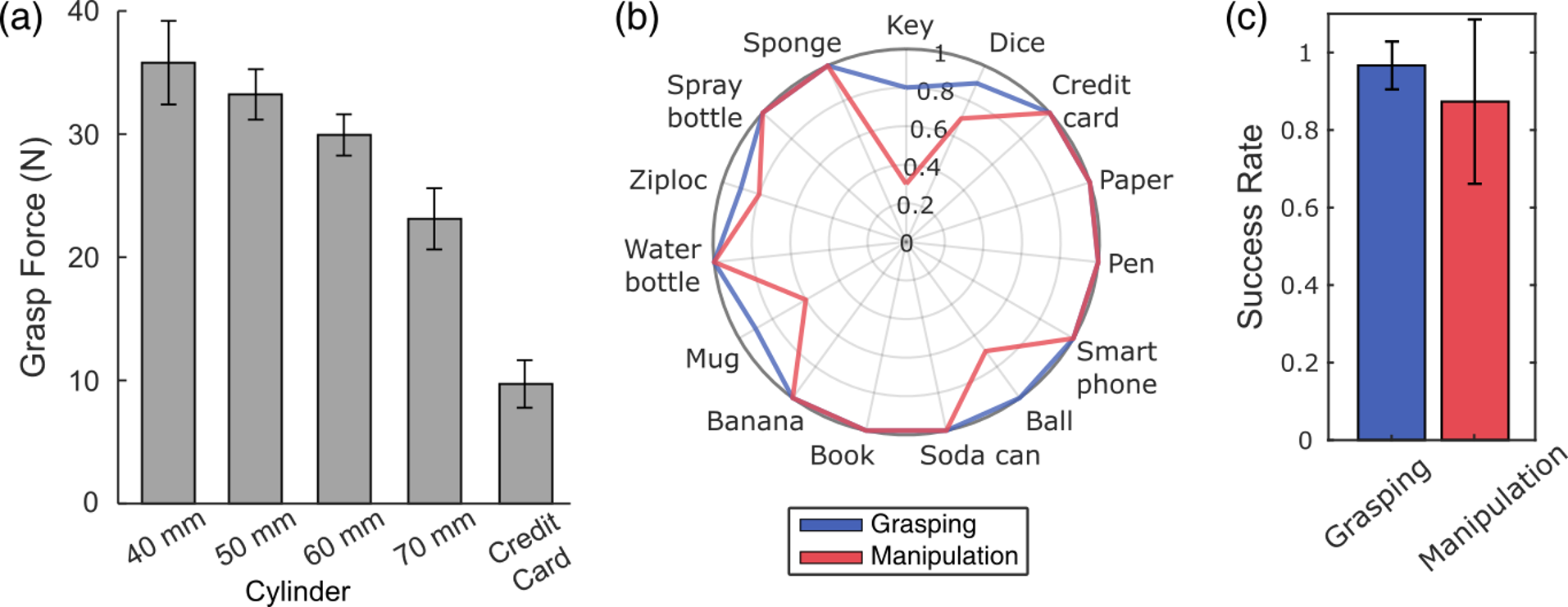
The results of the ADL Grasp and Manipulation Test are depicted in Figure 3(b). Eleven objects achieved a 100% success rate for grasping tasks: credit card, paper, pen, smartphone, ball, soda can, book, banana, water bottle, spray bottle, and sponge. However, during manipulation tasks, one object experienced failures. The ball exhibited a lower success rate during manipulation due to its spherical shape, which required it to be held between only one finger and the artificial palm, and often resulted in the object falling during the task due to instability.
The key object demonstrated the lowest success rates, achieving only an 80% success rate for grasping and 30% for manipulation. This discrepancy highlights the challenge of stabilizing the irregular and small geometry of the key during manipulation tasks with single point contact. The Ziploc bag has 5 golf balls inside it that make irregularity of the shape resulting in several failure cases during the task. In the case of the mug, which is heavy with a slippery surface and larger diameter made it difficult to perform the grasp and manipulation task.
The average success rate for the ADL grasp and manipulation test across all tested objects are presented in Figure 3(c). The Passive Dorsal Grasper achieved an average success rate of 96.7 ± 5.96% in grasping and 87.3 ± 20.5% in manipulation. The higher average success rates indicate that the Passive Dorsal Grasper is promising as a wearable assistive device at establishing grasping and stability with a wide variety of object shapes.
DISCUSSION
The results of the grip strength testing and ADL grasp and manipulation task show promise for the Passive Dorsal Grasper as an alternative method for grasping for individuals with SCI, who are otherwise unable to perform prehensile grasping. These results show that the passive grasper can successfully resist sufficient force to grasp many objects with grasp forces near 30 N for object diameters of 40-60 mm. This is sufficient for many common objects but suggests limitation in its ability to grasp objects that cannot be held in both fingers, are too large or require extensive wrist extension to secure. Additionally, after the conclusion of the ADL grasp and manipulation task the researcher was able to return to some of the objects that the Passive Dorsal Grasper struggled the most on, such as the key, and perform 10 successful grasp and manipulation trials in a row. This suggests the device may perform better than the results suggest when accounting for this learning effect.
It seems that modifying the geometry and mechanical properties of the aluminum fingers may allow for more successful grasping of certain objects, perhaps by decreasing the angle between the fingers and the back of the hand for smaller objects. Alternatively, increasing the stiffness of the fingers may allow for the application of more grip force without as much deflection. Such considerations are important to analyze in future work in order to create an assistive device that can be effective for a wide range of ADL tasks while still remaining easy to use and low-profile/lightweight enough to stay out of the way when stowed.
CONCLUSIONS
The Passive Dorsal Grasper introduced in this work demonstrates the potential usefulness of a simple, stow-able device to extend the range of objects users with cervical SCI can grasp and manipulate with remaining wrist extension regardless of hand morphology or contractures. By designing the device to be lightweight, low profile and deployable as needed, the device can be worn for long durations without getting in the way, reducing the need to don and doff it which is one commony noted reason for under use or abandonment of assistive devices.
Future work is needed to test the device with persons with SCI to determine if the usability translates. Additional testing in the home, performing ADLs with and without the device for comparison in individuals with SCI will also be essential to evaluate the impact on ADL ease and independence. The device can also be left with the participants in the home to allow unsupervised exploration of other tasks the device can be useful for. Also, in order to quantify the embodiment of the device, we can perform widely used survey methods such as the System Usability Score [9] which provides a comprehensive understanding of the usability of the device to the targeted population.
REFERENCES
[1] National Spinal Cord Injury Statistical Center. (2022). Traumatic spinal cord injury facts and figures at a glance. Birmingham, AL: University of Alabama at Birmingham.
[2] Anderson, K. D. (2004). Targeting recovery: priorities of the spinal cord-injured population. Journal of neurotrauma, 21(10), 1371-1383.
[3] A. Bryden, A. Peljovich, H. Hoyen, G. Nemunaitis, K. Kilgore, and M. Keith, “Surgical restoration of arm and hand function in people with tetraplegia,” Topics in Spinal Cord Injury Rehabilitation, vol. 18, no. 1, pp. 43–49, 2012.
[4] Bryden, A., Peljovich, A., Hoyen, H., Nemunaitis, G., Kilgore, K., & Keith, M. (2012). Surgical restoration of arm and hand function in people with tetraplegia. Topics in Spinal Cord Injury Rehabilitation, 18(1), 43-49.
[5] Wessels, R., Dijcks, B., Soede, M., Gelderblom, G. J., & De Witte, L. (2003). Non-use of provided assistive technology devices, a literature overview. Technology and disability, 15(4), 231-238.
[6] Sugawara, A. T., Ramos, V. D., Alfieri, F. M., & Battistella, L. R. (2018). Abandonment of assistive products: assessing abandonment levels and factors that impact on it. Disability and Rehabilitation: Assistive Technology, 13(7), 716-723.
[7] Lee, J., Yu, L., Derbier, L., & Stuart, H. S. (2021, May). Assistive supernumerary grasping with the back of the hand. In 2021 IEEE International Conference on Robotics and Automation (ICRA) (pp. 6154-6160). IEEE.
[8] Lee, J., Mcpherson, A. I., Huang, H., Yu, L., Gloumakov, Y., & Stuart, H. S. (2024). The Supernumerary Dorsal Grasper for people with C5-C7 spinal cord injury. Authorea Preprints.
[9] Brooke, J. (1996). SUS: A quick and dirty usability scale. Usability Evaluation in Industry.