Kicking it off: Do toddlers with disabilities activate leg muscles when driving with a joystick?
Madeleine E. McCreary1, Kimberly A. Ingraham1, Heather A. Feldner1, Katherine M. Steele1
1University of Washington
INTRODUCTION
While typically developing children take independent steps around 12-15 months of age, the onset of self- initiated mobility for children with motor disabilities is significantly delayed, typically between 3-5 years of age [1, 2]. Children who go on to become wheelchair users often do not gain access to powered mobility technology until 3-5 years [3, 4]. This delay can be detrimental, as self-initiated mobility leads to rapid development in social, language, cognitive, perceptual, and motor skills [5]. Introducing powered mobility at a younger age provides access to self-initiated mobility and exploration. However, device cost, size, portability, and negative perceptions of powered mobility hinder early access to this technology [3].
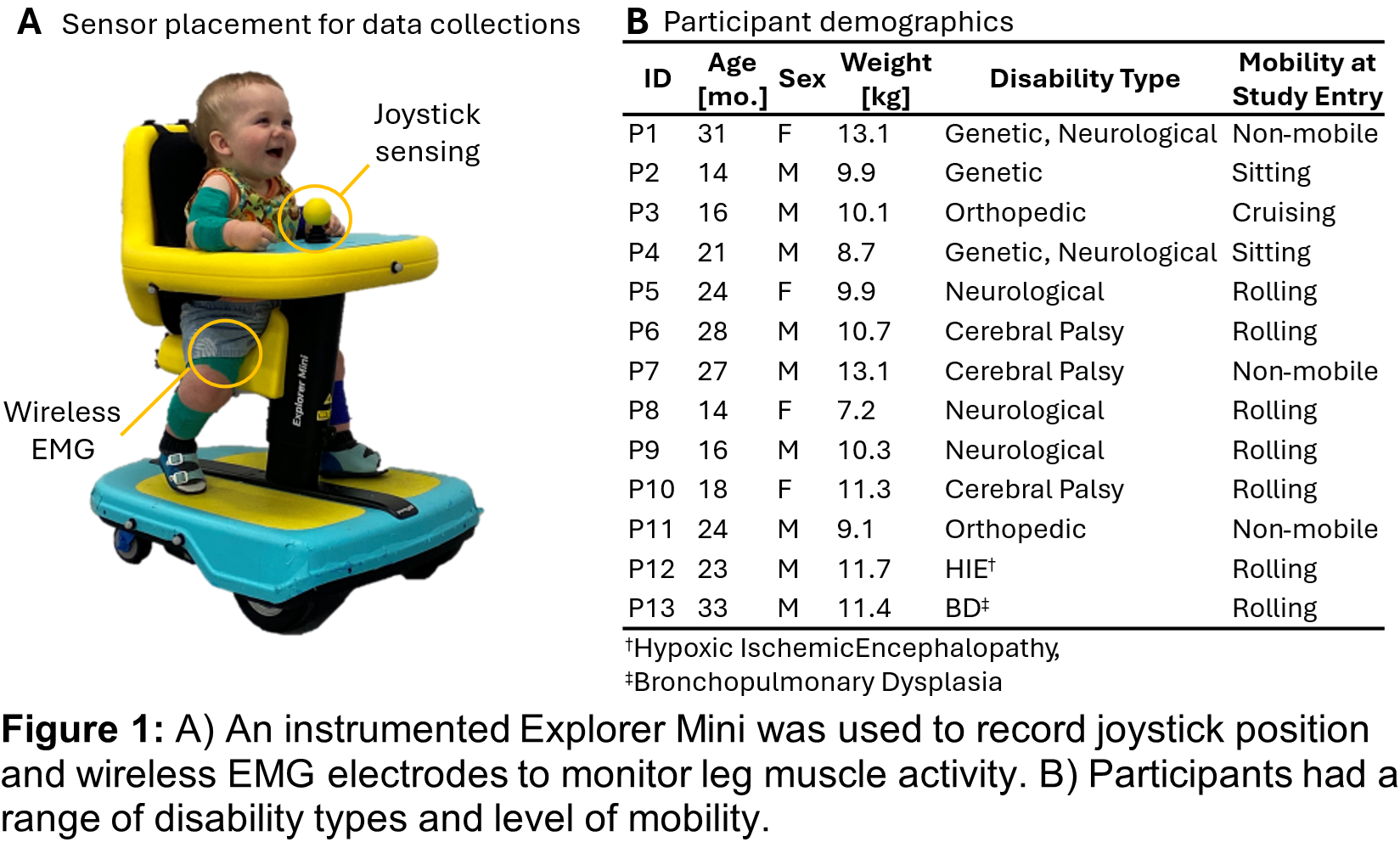
The Explorer Mini (Permobil AB, Kista, Sweden, Fig. 1A) is an FDA-cleared powered mobility device for children ages 12-36 months. It can be driven in seated, semi-standing, or standing positions and is steered with a joystick. Its introduction to the commercial market in 2020 has reduced many of the barriers to early powered mobility access as a lightweight (24 kg) and comparatively inexpensive (under $3000) device. As a new device, initial studies have assessed use patterns, developmental gains, and caregiver perceptions of the Explorer Mini [6–9]. There is a high success rate in exploratory behavior while driving the Explorer Mini, even if it’s a child’s first time using it [6, 7]. Children who regularly use the Explorer Mini show significantly greater changes in communication and gross motor development than those who do not [9]. Additionally, as children with disabilities use the Explorer Mini, the distance they travel and the complexity of their joystick movements increases with experience, displaying the benefits of regular use [8].
Reduced selective motor control is common for children with disabilities and coupled activity between the arms and leg muscle activity has been observed and related to functional deficits in adults with neurologic injury [10, 11]. Driving with a joystick is a complex motor task, requiring visual input, motor planning, and upper body coordination. Reduced selective motor control of children with motor disabilities may result in leg activation while using the joystick. Therefore, quantifying leg activation during Explorer Mini usage can provide insight into motor control strategies at use and measure selective motor control. The purpose of this study was to quantify leg muscle activity of toddlers with motor disabilities around joystick use while using the Explorer Mini and assess if leg muscle activation changes with experience.
METHODS
We enrolled 13 children with motor disabilities (age: 22.2 ± 6.4 months, Fig. 1B). Inclusion criteria were that children must be 1) between 12-36 months old, 2) have a disability or developmental delay that impacts their movement, and 3) be able to sit upright with support for up to 15 minutes.
Children attended 12 in-lab visits where they engaged with an instrumented Explorer Mini that recorded joystick position (Fig. 1A) in an enriched play environment tailored to child preferences. Each visit consisted of two 15-20 minute play sessions separated by a short 5-10 minute break. Seat and tray height of the Explorer Mini were adjusted at the beginning of each play session to ensure optimal positioning of the child. We placed wireless electromyography (EMG) electrodes (Delsys Inc, Natick, MA) on the right and left quadriceps femoris muscle group. During each play session, children engaged in child-led, exploratory play. The duration of each play session varied based on child engagement and mood.
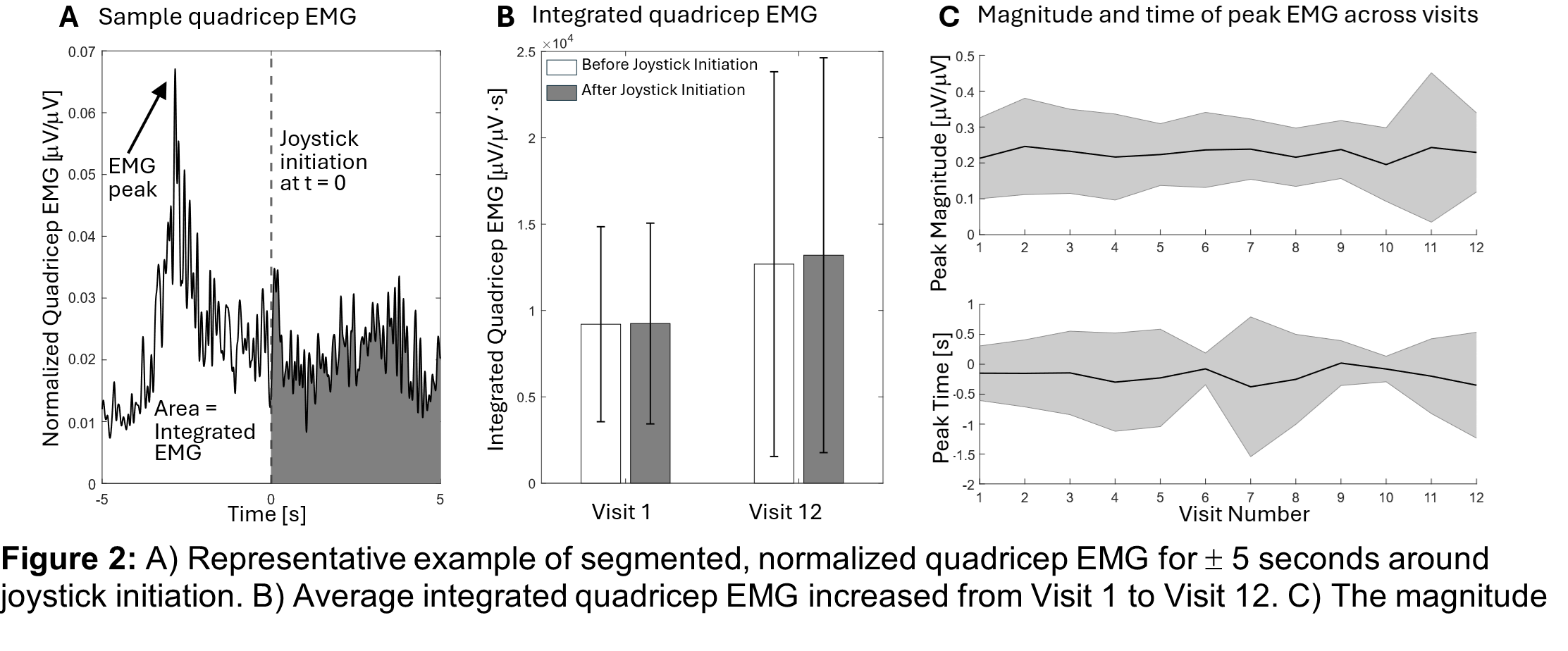
To quantify quadriceps activation around joystick use we first identified “j stic initiation” as the time point when the joystick was moved away from neutral. The window of EMG analysis was set to 5 seconds before and after each joystick initiation, yielding 10 second bouts. We chose ±5 seconds based on a sensitivity analysis of windows around the initiation of joystick movement. Joystick initiations with adult interference (e.g., clinician steering the Explorer Mini) were marked and excluded from analysis. All analyses were carried out using custom MATLAB scripts (MathWorks, Natick, MA). EMG data were high pass filtered at 20 Hz, demeaned, rectified, and low pass filtered at 10 Hz for analysis. EMG data were then normalized to the maximum EMG value of the visit. To compare EMG activity before versus after joystick initiation and across visits, we quantified integrated area via cumulative trapezoidal numerical integration. The peak EMG value and time of peak for each window was identified to assess changes in magnitude and timing across visits. To identify quadricep activation patterns, we performed dimensionality reduction of the bilateral EMG data through principal component analysis. K-means cluster analysis was performed to sort the EMG windows into distinct quadricep activation patterns using the first 3 principal components. Clustering was randomly initialized and then iterated upon for a maximum of 10,000 iterations.
RESULTS
Across all participants and all sessions, 21,551 bouts were identified (a representative bout is shown in Fig. 2a). The average integrated quadricep EMG was similar before and after joystick initiation but increased from Visit 1 to Visit 12 by approximately 38% on average (Fig. 2b). The peak magnitude of the quadriceps EMG did not display much change across visits, but on average the time of peak EMG occurred 0.47s earlier during Visit 12 than Visit 1 (Fig. 2c).
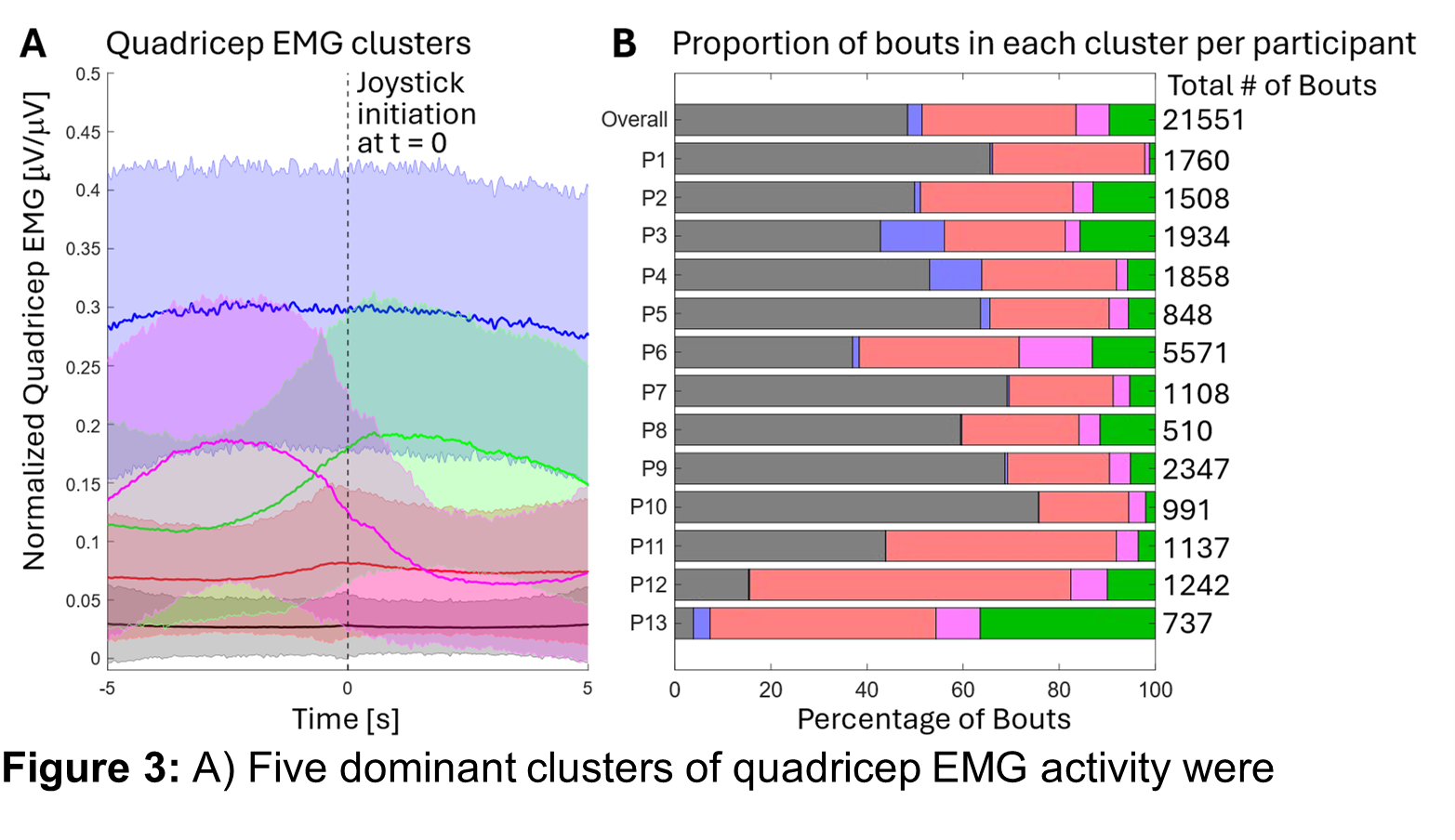
Five unique patterns of quadricep activation were identified through cluster analysis (Fig. 3a). The most common pattern was minimal activity (black) for 48% of bouts (range: 4-76%, Fig. 3b). Two clusters showed a peak before joystick initiation. The more prevalent of these clusters (red) had a lower peak and encompassed 32% of bouts (range: 19-67%, Fig. 3b). The other had a steeper magnitude increase and higher peak (pink) for 7% of bouts (range: 1-15%, Fig. 3b). There was also a cluster that peaked after joystick initiation (green) for 10% of bouts (range: 1-36%, Fig. 3b) For a small number of bouts, the quadriceps were active before and after joystick use (blue), representing only 3% of bouts (range: 0-13%, Fig. 3b). The proportion of bouts in each cluster was variable between participants (Fig. 3b).
DISCUSSION
We quantified quadriceps activation of toddlers with motor disabilities while using the Explorer Mini, specifically around joystick activation. Over 12 visits, integrated quadricep EMG in the 10 second window around joystick initiation increased, suggesting participants engaged their leg muscles more as they gained experience with the Explorer Mini. Because the peak quadricep magnitude demonstrated minimal changes across visits, we conclude that the legs were activated over a longer period around joystick initiation. The earlier occurrence of peak EMG suggests that as children gained experience, they were more likely to activate their legs in preparation of joystick initiation.
The quadriceps were activated for nearly half of the joystick initiation bouts, suggesting some coupling between arm and leg movement. When the quadriceps were activated, it was more common for the quadricep EMG peak to occur before joystick initiation (i.e., red and pink clusters). These clusters may reflect changes in selective motor control or inter-limb coordination when using a joystick [10].
The variability in cluster proportions between children indicates child-specific differences in leg activation patterns while using the Explorer Mini. Three children in this study were diagnosed with cerebral palsy (P6, P7, and P10). At this age, cerebral palsy is associated with the retention of immature motor strategies such as co-contraction and poor selective control of movements [12]. We expected to see more leg activation around joystick initiation in the children with cerebral palsy, but over 70% of P7 and P10’s uts had minimal leg activity (black). P6 had higher proportions of bouts in the high activity before (magenta) and after (green) joystick initiation clusters. Cerebral palsy is a very heterogeneous population, which often is not diagnosed until 2-3 years of age [12]. Evaluating these child-specific patterns of motor control during joystick use may provide insight into motor function and development.
There was one child whose disability was not neurological, genetic, or orthopedic. P13’s disability type was bronchopulmonary dysplasia, which is a condition that impairs lung development [13]. P13 had the lowest proportion of bouts in the minimal activity cluster (black) out of all participants and the highest proportion in the high activity after joystick initiation cluster (green). The differences in P13’s cluster proportions from the group average highlight the potential relationships between leg activation patterns and disability type. Performing this protocol with a larger group with diverse motor disabilities and tracking longitudinal changes will support future research to understand and optimize child-device interactions for powered mobility and other assistive technology.
Participant comfort, engagement, and fun were prioritized at each visit. Children were free to explore the play environment. We followed the guidance for instructing children’s use of powered mobility, based on their Assessment of Learning Powered Mobility (ALP) stage. While this can limit protocol repeatability and standardization (i.e., participants cannot be asked to execute a specific path or activity multiple times), this represents a common challenge in performing detailed neuromechanical studies in this population. Additionally, isolating specific muscles with EMG was difficult due to the small size of participants. Signals from the quadricep EMG sensors likely include cross-talk from several muscles located in the thighs, making the term “leg activation” more accurate.
When children with disabilities drive the Explorer Mini, arm movement and leg activation are often coupled. This relationship suggests reduced selective motor control, which can be quantified and tracked over time to provide insight into how self-initiated mobility impacts neuromuscular control. Collecting EMG data from the arms will enable a more comprehensive understanding of how motor control strategies change with experience. Additionally, characterization of leg activation during different seating positions will inform the development of clinical recommendations for Explorer Mini usage. Future research will enable better customization and evidence-based deployment of technology that supports self-initiated mobility and development for children with motor disabilities.
ACKNOWLEDGEMENTS
We thank the Center for Research & Education on Accessible Technology and Experiences (CREATE) and the Institute for Learning and Brain Sciences (I-LABS) for their support of this work, as well as LUCI for instrumenting the Explorer Mini and Mia Hoffman, Nicole Zaino, Liesbeth Gijbels and Alexis Sinclair for data collection assistance.
REFERENCES
-
Gerber RJ, Wilks T, Erdie-Lalena C. Developmental Milestones: Motor Development. Pediatrics In Review 2010; 31: 267–277.
-
Begnoche DM, Chiarello LA, Palisano RJ, et al. Predictors of Independent Walking in Young Children With Cerebral Palsy. Physical Therapy 2016; 96: 183–192.
-
Feldner HA, Logan SW, Galloway JC. Why the time is right for a radical paradigm shift in early powered mobility: the role of powered mobility technology devices, policy and stakeholders. Disability and Rehabilitation: Assistive Technology 2016; 11: 89–102.
-
Kenyon LK, Jones M, Livingstone R, et al. Power mobility for children: a survey study of American and
anadian thera ists’ ers ectives and ractices Developmental Medicine & Child Neurology 2018; 60: 1018–1025.
-
Campos JJ, Anderson DI, Barbu-Roth MA, et al. Travel Broadens the Mind. Infancy 2000; 1: 149–219.
-
lummer L gan rress l rer ini: nfants’ nitial erience with a vel ediatric
Powered Mobility Device. Physical & Occupational Therapy In Pediatrics 2020; 41: 192–208.
-
Zaino NL, Ingraham KA, Hoffman ME, et al. Quantifying toddler exploration in different postures with powered mobility. Assistive Technology; 0: 1–9.
-
Ingraham KA, Zaino NL, Feddema C, et al. Quantifying joystick interactions and movement patterns of toddlers with disabilities using powered mobility with an instrumented Explorer Mini. IEEE Transactions on Neural Systems and Rehabilitation Engineering; In Review.
-
Logan SW, Sloane BM, Kenyon LK, et al. Powered Mobility Device Use and Developmental Change of Young Children with Cerebral Palsy. Behavioral Sciences 2023; 13: 399.
-
Cahill-Rowley K, Rose J. Etiology of impaired selective motor control: emerging evidence and its implications for research and treatment in cerebral palsy. Developmental Medicine & Child Neurology 2014; 56: 522–528.
-
Sánchez N, Acosta AM, López-Rosado R, et al. Neural Constraints Affect the Ability to Generate Hip Abduction Torques When Combined With Hip Extension or Ankle Plantarflexion in Chronic Hemiparetic Stroke. Front Neurol 2018; 9: 564.
-
Graham HK, Rosenbaum P, Paneth N, et al. Cerebral palsy. Nat Rev Dis Primers 2016; 2: 1–25.
-
Thébaud B, Goss KN, Laughon M, et al. Bronchopulmonary dysplasia. Nat Rev Dis Primers 2019; 5: 1–23.