Solveig Millett![]() 1
1![]() , Corinne Jean-Louis
, Corinne Jean-Louis![]() 1
1![]() , Delilah Hsu
, Delilah Hsu![]() 1
1![]() , Olivia Dungan
, Olivia Dungan![]() 1
1![]() , Sara Benham
, Sara Benham![]() 1
1![]()
![]() 1
1![]() Department of Rehabilitation Sciences, Moravian College, Bethlehem, PA
Department of Rehabilitation Sciences, Moravian College, Bethlehem, PA
INTRODUCTION
There are more than one billion individuals globally with disabilities who need one or more assistive technology (AT) devices, and it is estimated that two billion people will need at least one assistive device by 2030. [1] However, at present only one in 10 people who need AT have access to it due to documented barriers such as cost, availability, lack of research and awareness, and availability of personnel trained in the provision of AT. [2,3] These needs prompt the exploration of novel AT service delivery methods that are accessible, affordable, and customizable to promote the wellbeing and increased independence of individuals with disabilities. In more recent years, technological advancements have unfolded new prospects for assistive device provision, particularly through the use of three-dimensional (3D) printing technology. 3D printing offers the possibility of designing individualized and reproducible products at relatively low costs. As this technology has become more affordable and accessible, it has been increasingly implemented in healthcare and rehabilitation settings. The benefits of 3D printing are particularly relevant for occupational therapy practitioners (OTPs), who regularly fabricate and implement AT to enhance client performance. 3D printing specific to occupational therapy service delivery includes the exploratory reports of the fabrication of customized pillboxes and assistive hand tools to open beverage bottles, to unlock/lock doors, and to write. [4-6] Despite the benefits, 3D printing is not yet mainstream in occupational therapy settings with noted barriers including the lack of awareness, experience, and training, as well as the time required to learn to operate computer aided design (CAD) software and 3D printers. [7]
In order to address the barriers and to prepare for the anticipated mainstreaming of 3D printing technology in clinics and hospitals, OTP perceptions of 3D printing must be examined to project technology adoption. The guiding framework of this study is the Technology Acceptance Model (TAM), which considers the importance of user perceptions to predict future use of new technologies in workplace settings. [8] For example, among rehabilitation professionals, the perception that the technology will benefit their work and patients is the most important factor determining the adoption of new technologies. [9] According to the TAM, more exposure to and experiences with the technology increase the likelihood that one will use it, with reports that more experience with 3D printing contributes to more positive perceptions of the technology. [10] However, research has not yet focused on the OTP perceptions of 3D printing in inpatient settings, where AT is routinely fabricated and trialed but also where OTPs often have limited time and resources to do so in a patient-centered manner. With the understanding that experience influences the use of technology, the purpose of this case study was to determine whether and how an experience implementing a 3D printed device with a patient impacts the OTP's perceived acceptance of 3D printing technology in regard to Usefulness, Ease of Use, and Intention to Use. We also explored the OTP's perceived benefits and barriers of using 3D printing in an inpatient rehabilitation setting in order to inform future implementation of 3D printing in this setting.
DESIGN & METHODS
This study was a single case pretest-posttest design with additional qualitative measures. The study protocol was approved by the Human Subjects Institutional Review Board at Moravian College. The OTP participant was recruited through an email to the inpatient occupational therapy email listserv of a local inpatient rehabilitation center. To be included in the study, the OTP was required to have a license to practice, be employed full-time or part-time in an inpatient rehabilitation setting, have at least six months of experience, and consider themselves a novice in 3D printing. All data collection was electronic. After signing an informed consent, the OTP answered demographic questions and completed the pretest questionnaire. At that time, the participant was provided links to two short, educational videos describing the 3D printing process and its potential application to clinical settings, as well as a list of 3D printed devices available to implement with a patient.
The primary outcome measure was a pretest and posttest questionnaire based on the TAM scale and modified to relate to 3D printing technology. [8] This measure was selected based on established reliability and validity and its extensive use to predict user acceptance and future use of new technologies. The modified TAM scale consisted of nine items based on the following TAM scale categories: perceived Usefulness (items 1-3), Ease of Use (items 4-6), and Intention to Use (items 7-9). The posttest included four additional questions on the perceived effectiveness of the chosen device and six open-ended questions regarding the patient, the OTP's experience, and the anticipated benefits and challenges of integrating 3D printing in the inpatient rehabilitation setting. All items, except open-ended questions, were rated on a 7-point Likert scale ranging from 1 (totally disagree) to 7 (totally agree). An outcome analysis was completed by totaling the OTP's modified TAM responses by category and comparing the pretest and posttest responses. Responses to items regarding device effectiveness and open-ended questions were then analyzed for themes.
RESULTS
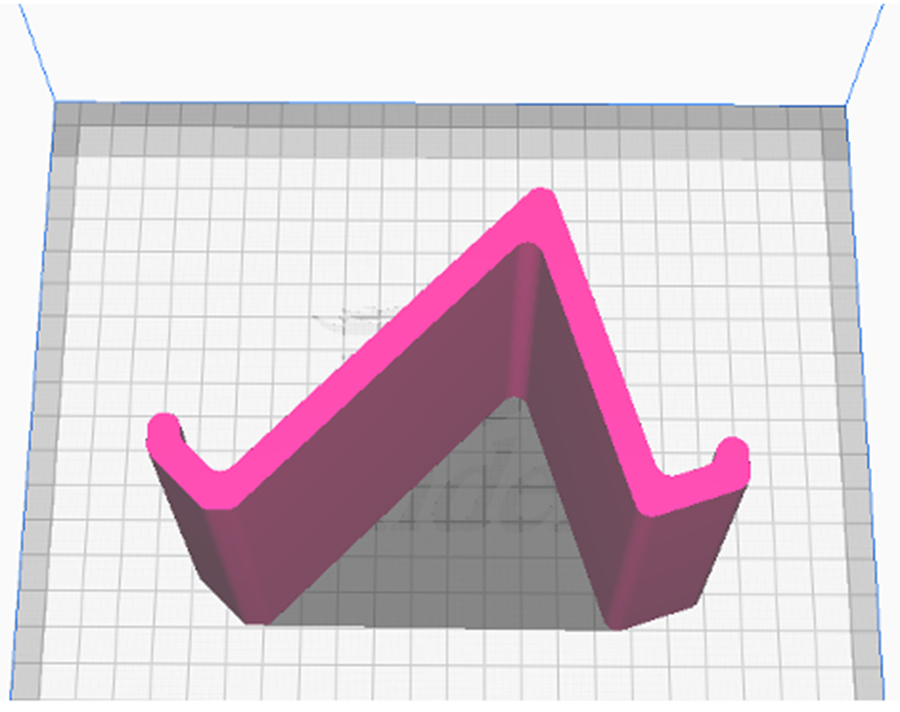
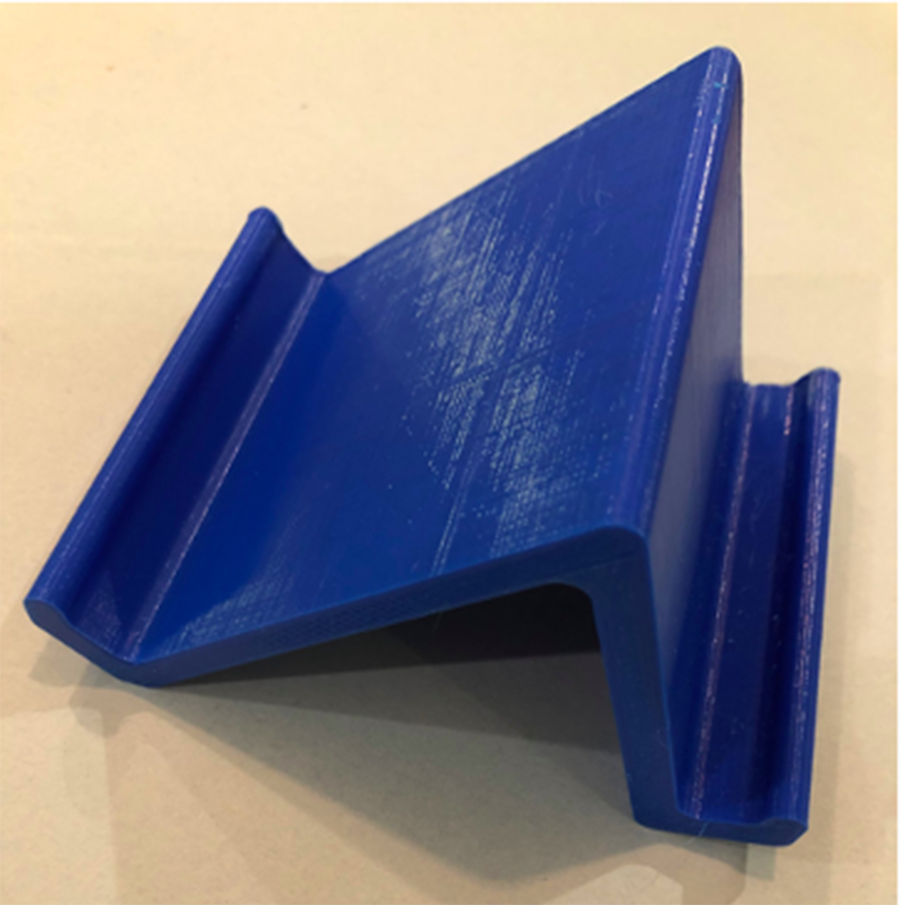
The OTP of this case study was a 32 year-old, white, male, licensed occupational therapist with nine years of experience. He requested a phone stand to implement with a patient with a spinal cord injury. The research team then selected a design and modified its dimensions (Figure 1) and printed the device (Figure 2). [11] Two copies of the device were then delivered directly to the OTP for application, training, and education with his patient. The OTP was also provided information regarding the time (10 hours) and cost ($1.89) of device production. Following implementation of the 3D printed phone stand, the OTP completed the posttest questionnaire.
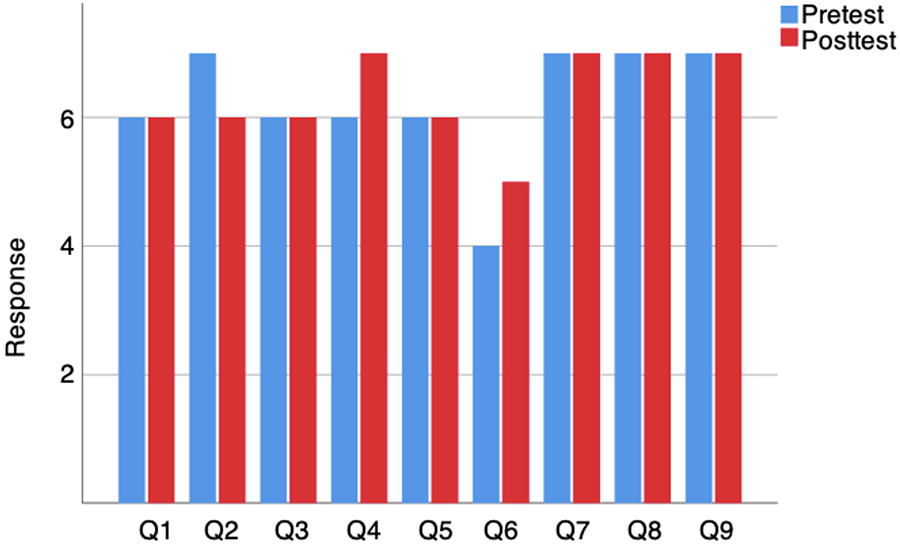
Table 1 outlines the questionnaire items and responses, and Figure 3 is a visualization of the pretest to posttest responses. From pretest to posttest, the OTP's responses indicated a slight decrease in Usefulness (pre = 19/21, post = 18/21), a modest increase in Ease of Use (pre = 16/21, post = 18/21), and no change for Intention to Use (pre = 21/21, post = 21/21). At posttest, the participant rated 6/7 for all items relating to device effectiveness. As reported by the OTP, the phone stand was implemented with a patient with a spinal cord injury who experienced difficulties stabilizing their cell phone. The OTP indicated that further modifications to the 3D printed phone stand were necessary to prevent slippage of the phone and of the stand on the bedside table. The participant reported several perceived benefits of 3D printing technology: greater customizability to meet the needs of more patients as compared to off-the-shelf devices, increased availability of devices, cost-effectiveness, and the ability to fabricate 3D printed orthoses. Anticipated challenges of using 3D printing in OTP practice included necessary training on 3D printing technology and access to appropriate software.
DISCUSSION
This study examines perceptions of 3D printing technology of an OTP before and after implementing a 3D printed device with a patient and explores perceived benefits and barriers of integrating this technology in an inpatient rehabilitation setting. The results of this study suggest that implementing a 3D printed device with a patient combined with indirect exposure to the 3D printing process through brief educational videos influenced the OTP's perceived acceptance of 3D printing technology. His responses indicated overall favorable perceptions of 3D printing despite having no prior experience using this technology. Pretest results indicated that the participant's intention to use 3D printing technology was high, possibly from previous knowledge of the benefits, and this did not diminish following education and hands-on experience. Over this same period, a small increase was evident in Ease of Use, as consistent with previous reports after exposure. [10] The posttest suggests that the OTP would be more comfortable using 3D printing technology with an expert, but it is notable that his confidence to use 3D printing without expert help improved. Although improvement was evident in this category, the OTP's perceptions of Ease of Use was relatively lower than Intention to Use. This was further explained by his open-ended responses regarding anticipated challenges of access to appropriate training and software. Meanwhile, the OTP's perceived Usefulness of this technology was high, though decreased slightly. However, he appears to perceive 3D printing as beneficial, reporting customizability, cost-effectiveness, time-efficiency, and use for custom orthoses, as reported in the responses to the open-ended questions, and supported by previous literature. [7]
|
Questionnaire Items |
Response |
|
Pre |
Post |
||
TAM Perceived Usefulness |
|
6 |
6 (=) |
|
7 |
6 (↓) |
|
|
6 |
6 (=) |
|
Total Perceived Usefulness (/21) |
19 |
18 (↓) |
|
TAM Perceived Ease of Use |
|
6 |
7 (↑) |
|
6 |
6 (=) |
|
|
4 |
5 (↑) |
|
Total Perceived Ease of Use (/21) |
16 |
18 (↑) |
|
TAM Intention to Use |
|
7 |
7 (=) |
|
7 |
7 (=) |
|
|
7 |
7 (=) |
|
Total Intention to Use (/21) |
21 |
21 (=) |
|
Device Effectiveness (Posttest) |
|
-- |
6 |
|
-- |
6 |
|
|
-- |
6 |
|
|
-- |
6 |
|
There were several limitations in this study. Firstly, as a case study, it is difficult to generalize results to other OTPs in inpatient settings. Additionally, self-selection bias may have contributed to a ceiling effect in survey responses. The recruitment and inclusion of more OTPs with a greater variety of initial perceptions of 3D printing technology would improve the generalizability of results. This study did not include direct comparison to off-the-shelf AT or measurement of patient reported outcomes, though this was partially mitigated with the addition of questionnaire items regarding perceptions of these topics. Lastly, the OTP in this study did not engage directly with 3D printing software and equipment, which may limit realistic perceptions.
Future studies might address these study limitations by conducting similar research fully within an inpatient setting with more qualitative data collection as well as greater integration of and engagement with the 3D printers at the inpatient site. This may improve both recruitment of OTPs and data collection of the barriers and strategies for successful integration of the 3D printing process within the setting.
Low cost, customizability, and timely provision of devices make 3D printing an appealing technology in clinical practice. However, the OTP participating in this study reported relatively lower confidence in using 3D printing technology without an expert and additional concerns regarding training and software. It will be important to provide a structure in which OTPs of various experience levels feel supported to learn and use 3D printing technology, including opportunities for online and hands-on training, practice, and mentorship. It may be helpful to designate one "expert" in the department who can serve as a mentor and resource for practitioners less experienced in 3D printing. [12]
CONCLUSION
3D printing is an emerging and potentially important tool in the timely provision of effective, affordable, and patient-specific customized AT. As fabricators and providers of AT, OTPs have an opportunity to utilize 3D printing technology to improve patient outcomes. This study indicates that perceptions of 3D printing may shift with hands-on experiences using 3D printed devices in clinical practice. This highlights the importance of providing opportunities for OTPs to engage with 3D printing technology and printed devices while developing a service delivery plan to train OTPs and further integrate the technology into clinical practice.
REFERENCES
- Gupta, N., Castillo-Laborde, C., & Landry, M. D. (2011). Health-related rehabilitation services: Assessing the global supply of and need for human resources. BMC Health Services Research, 11(1), 276. doi:10.1186/1472-6963-11-276
- Kaye, H. S., Yeager, P. & Reed, M. (2008). Disparities in usage of assistive technology among people with disabilities. Assistive Technology, 20(4), 194-203. doi. 10.1080/10400435.2008.10131946
- Tangcharoensathien, V., Witthayapipopsakul, W., Viriyathorn, S., & Patcharanarumol, W. (2018). Improving access to assistive technologies: Challenges and solutions in low- and middle-income countries. WHO South-East Asia Journal of Public Health, 7(2), 84-89. doi: 10.4103/2224-3151.239419
- Schwartz, J. K., Caceres, Y., Centeno, A., Cruz, V., Gutierrez, J., & Orozco, N. (2020). Impact of pillbox customization on device satisfaction and medication adherence. American Journal of Occupational Therapy, 74(Suppl. 1).
- Janson, R., Burkhart, K., Firchau, C., Hicks, K., Pittman, M., Yopps, M., Hatfield, S., & Garabrant, A. (2020). Three-dimensional printed assistive devices for addressing occupational performance issues of the hand: A case report. Journal of Hand Therapy, 33(2), 164-169. https://doi.org/10.1016/j.jht.2020.03.025
- Buehler, E., Comrie, N., Hoffman, M., McDonald, S., & Hurst, A. (2016). Investigating the implications of 3D printing in special education. ACM Transactions on Accessible Computing, (8)3. doi: 10.1145/2870640
- Patterson, R. M., Salatin, B., Janson, R., Salinas, S. P., & Mullins, M. J. (2020). A current snapshot of the state of 3D printing in hand rehabilitation. Journal of Hand Therapy, 1-7. doi: 10.1016/j.jht.2019.12.018
- Venkatesh, V. & Davis, F. D. (2000). A theoretical extension of the technology acceptance model: Four longitudinal field studies. Management Science, 46(2), 169-332. https://doi.org/10.1287/mnsc.46.2.186.11926
- Liu, L., Cruz, A. M., Rincon, A. R., Buttar, V., Ranson, Q., & Goertzen, D. (2014). What factors determine therapists' acceptance of new technologies for rehabilitation: A study using the Unified Theory of Acceptance and Use of Technology (UTAUT). Disability & Rehabilitation, 37(5), 447–455. https://doi.org/10.3109/09638288.2014.923529
- Benham, S. & San, S. (2020). Student technology acceptance of 3D printing in occupational therapy education. American Journal of Occupational Therapy, (74)3. https://doi.org/10.5014/ajot.2020.035402
- Haberberger, C. (2017). Dual angle phone and tablet stand. Retrieved September 15th, 2020, from https://www.thingiverse.com/thing:2188695/files
- McGrath, C., Ellis, M., Harney-Levine, S., Wright, D., Williams, E. A., Hwang, F., & Astell, A. (2017). Investigating the enabling factors influencing occupational therapists' adoption of assisted living technology. British Journal of Occupational Therapy, 80(11), 668–675. https://doi.org/10.1177/0308022617711669