Upper Extremity Biomechanical Differences Between Wheelchair Lacrosse Athletes With Spinal Cord Injury and Able-Bodied Lacrosse Athletes During Overhead Throwing
Matthew M. Hanks![]() 1
1![]() , Alyssa J. Schnorenberg
, Alyssa J. Schnorenberg![]() 1
1![]() , Kenneth K. Lee
, Kenneth K. Lee![]() 2
2![]() , Brooke A. Slavens
, Brooke A. Slavens![]() 1,2
1,2![]()
![]() 1
1![]() University of Wisconsin-Milwaukee,
University of Wisconsin-Milwaukee, ![]() 2
2![]() Clement J. Zablocki Veterans Affairs Medical Center (Milwaukee)
Clement J. Zablocki Veterans Affairs Medical Center (Milwaukee)
INTRODUCTION
An estimated 294,000 individuals in the United States live with spinal cord injuries (SCI) [1], and many use manual wheelchairs for daily mobility and physical activity. Adaptive sports are enjoyed by manual wheelchair users with SCI to improve physical fitness, mental and social health, and employment opportunities [2,3]. As manual wheelchair users who participate in overhead adaptive sports greatly rely on their upper extremities for mobility, activities of daily life, and sport, they are at roughly twice the risk of developing shoulder pain and pathology [4]. Wheelchair lacrosse is a novel adaptive sport that has grown drastically in the last decade and combines overhead throwing with manual sport wheelchair propulsion. The shoulder may be susceptible to injury in wheelchair lacrosse as research has found that 43% of upper extremity injuries in able-bodied lacrosse occur at the shoulder [5] and rotator cuff tears are prevalent in 76% of overhead adaptive sport athletes [4]. The purpose of this study was to quantify and compare thorax, glenohumeral, elbow, and wrist joint kinematics of wheelchair lacrosse athletes with SCI and able-bodied lacrosse athletes during overhead throwing. A quantitative comparison between wheelchair athletes with SCI and able-bodied athletes is warranted to understand the biomechanical demands of the thorax and upper extremity during overhead throwing in wheelchair lacrosse.
METHODS

Five wheelchair lacrosse athletes with SCI (46±16 years, 71±3 in., 195±35 lbs.) and three able-bodied lacrosse athletes (24±4 years, 71±2 in., 203±46 lbs.) participated and were recruited from local university- and community-affiliated wheelchair and able-bodied lacrosse teams. Level of SCI (incomplete or complete) ranged from the 4th cervical vertebra (C4) to the 2nd lumbar vertebra (L2). All participants were right-hand dominant.
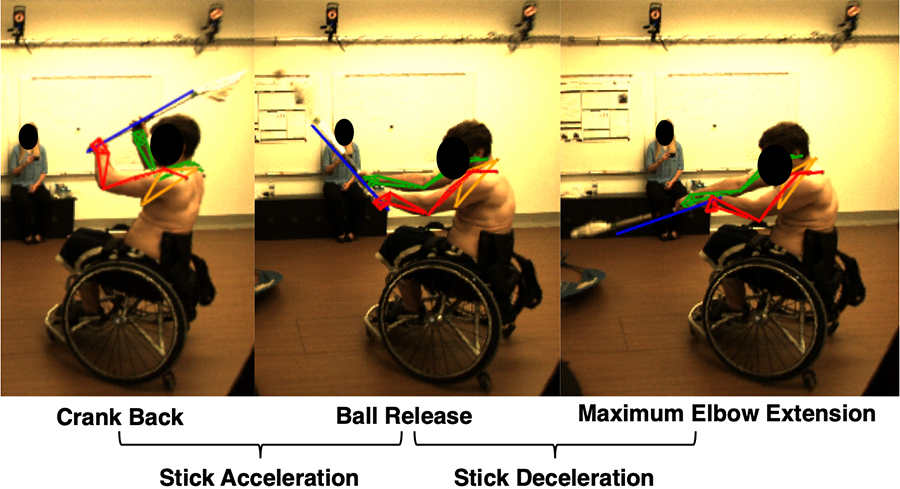
University Institutional Review Board approved the study and written consent was obtained prior to participation. Participants were affixed with 27 retro-reflective markers on select bony anatomical landmarks [6] and three additional markers were placed on the lacrosse stick and ball (Figure 1). Participants were instructed to perform multiple overhead throws using their preferred overhead throwing motion from a stationary position and a standardized men's lacrosse stick and ball into a net located in front of them. Participants with SCI performed overhead throwing while seated in their personal sports wheelchair and setup (SCI).
Able-bodied participants performed overhead throwing while seated in a standardized sport wheelchair with their hips and feet secured with a standard ratchet strap (AB-WC) and also while standing (AB-Standing). A 15-camera Vicon T-Series motion capture system with Vicon Nexus software (Vicon Motion Systems, Oxford, UK) was used to collect three-dimensional (3-D) kinematic data (240 Hz). Data were cleaned using Vicon Nexus software and the resulting marker trajectories were filtered using a Woltring filter. A custom inverse kinematics model was implemented using MATLAB (The MathWorks Inc., Natick, MA) [6]. Left-right axial rotation of the thorax, 3-D motion of the glenohumeral joint, flexion-extension of the elbow, and ulnar-radial deviation of the wrist were the focus of the analyses as these motions have been previously reported as key metrics in the overhead lacrosse throw [7]. Segment coordinate systems were aligned with recommendations from the International Society of Biomechanics [8], and a Z–X–Y Euler sequence was used to determine the joint angles of the distal segment relative to the proximal segment for all joints. For between-group analyses, mean joint angles were calculated at three events during the overhead throw identified by Mercer & Nielson [9]: (1) crank back: maximum elbow flexion of the dominant (top) arm, (2) ball release: the instant the ball left the pocket of the lacrosse stick head, and (3) maximum elbow extension of the dominant arm (Figure 2). Joint range of motion was assessed from crank back to maximum elbow extension. Peak joint angular velocity was assessed in two phases of the overhead throw: (1) stick acceleration and (2) stick deceleration [9].
Due to the non-normal distribution of the data, nonparametric independent samples Mann-Whitney U tests were conducted to assess differences between groups with statistical significance set at p<0.05. Group differences were analyzed for the thorax, dominant glenohumeral, elbow, and wrist joint angles at the overhead throw events, ranges of motion during the throw, and angular velocities during the stick acceleration and deceleration phases of the throw.
RESULTS
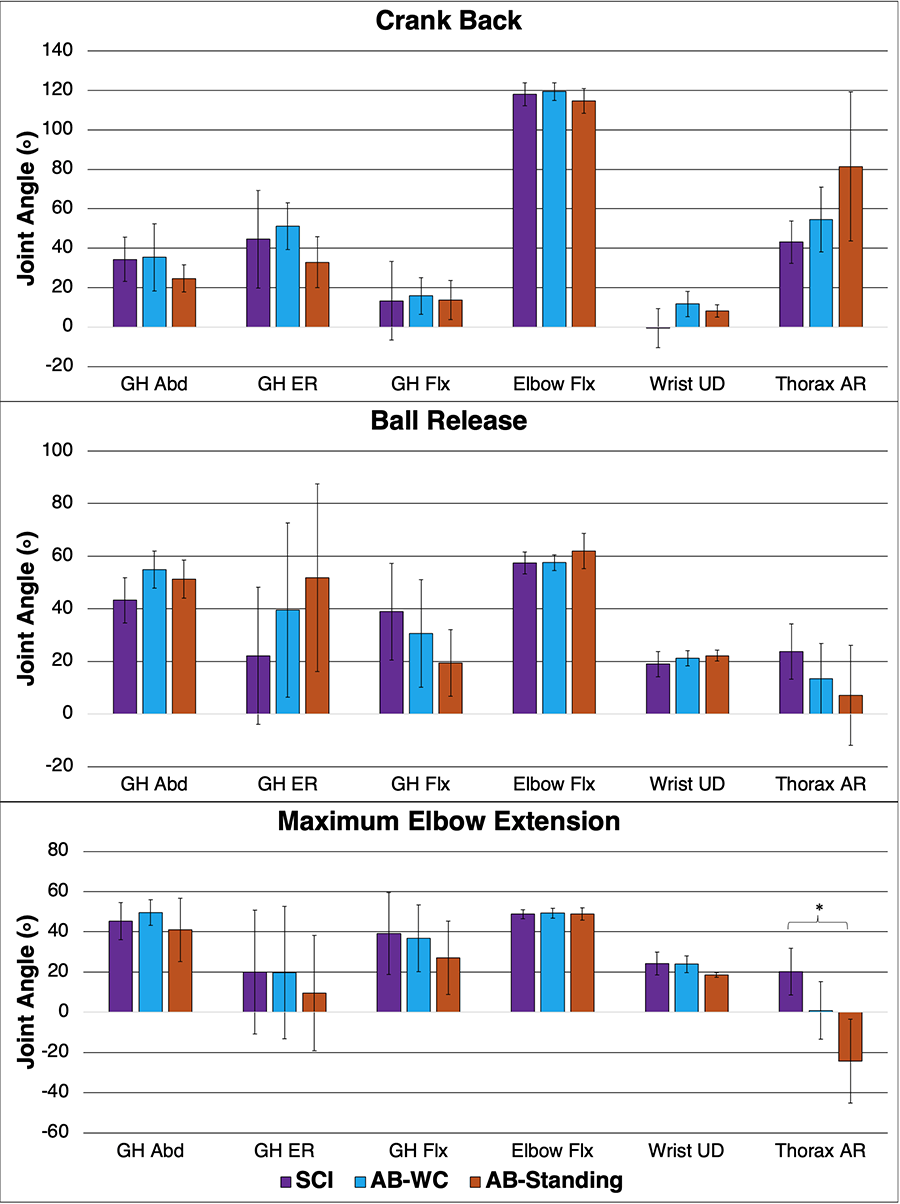
A significant difference between the SCI and AB-Standing groups was observed for thorax axial rotation at maximum elbow extension (20±12º right axial rotation vs. 24± 21º left axial rotation; p=0.036), respectively. No other significant differences were observed between the SCI and AB-Standing groups. No significant differences were found between the SCI and AB-WC groups (Figure 3).
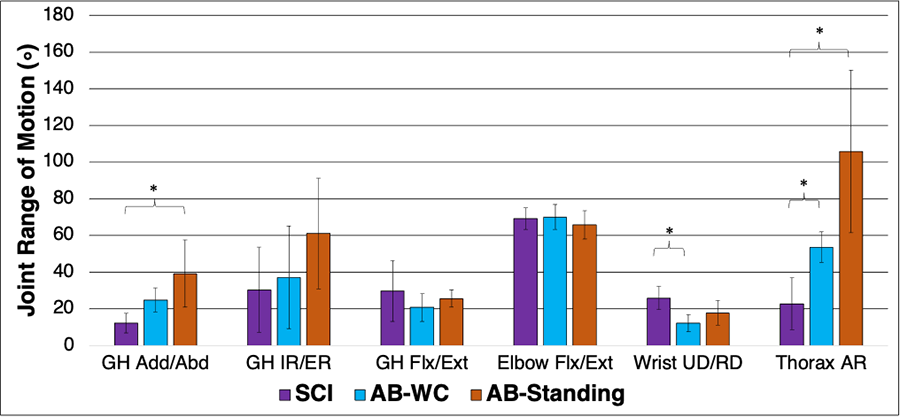
Significant differences between the SCI and AB-Standing groups were found for thorax axial rotation range of motion (23±14º vs. 106±44º; p=0.036) and glenohumeral joint adduction-abduction range of motion (12±5º vs. 39±18º; p=0.036), respectively. Significant differences between the SCI and AB-WC groups were found for the thorax axial rotation ranges of motion (23±14º vs. 54±8º; p=0.036) and wrist ulnar-radial deviation ranges of motion (26±6º vs. 12±5º; p=0.036), respectively (Figure 4).
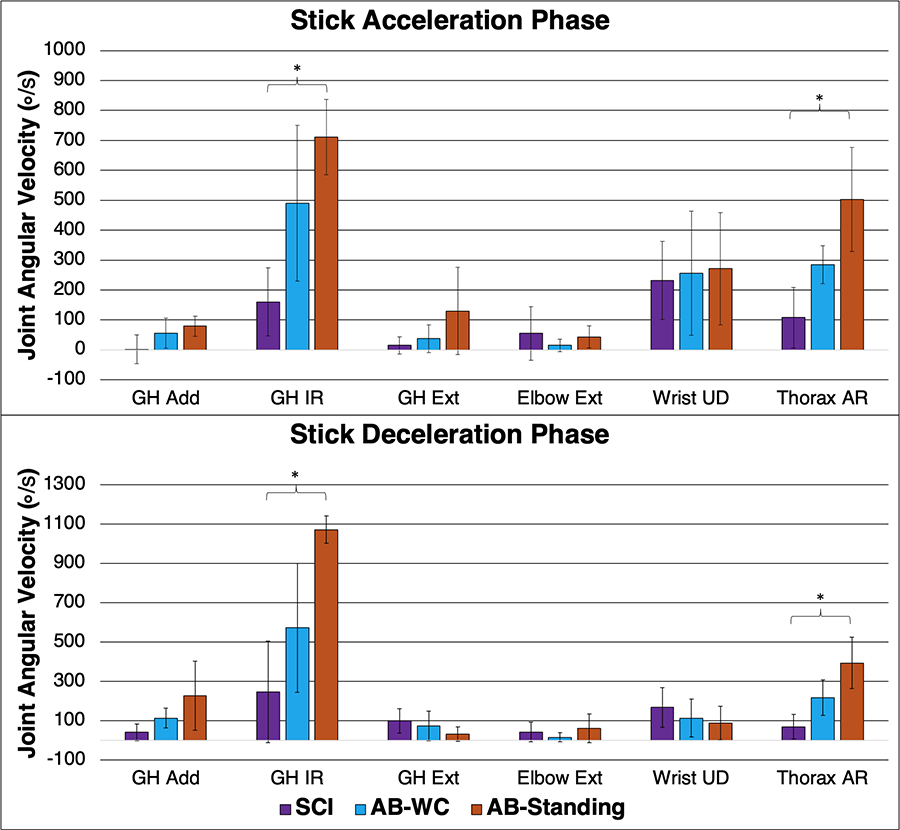
The SCI group exhibited significantly smaller peak thorax left axial rotation angular velocity (108±101º/s vs. 502±174º/s; p=0.036) and peak glenohumeral joint internal rotation angular velocity (160±114º/s vs. 711±125º/s; p=0.036) than the AB-Standing group during the stick acceleration phase, respectively. The SCI exhibited significantly smaller peak thorax left axial rotation angular velocity (69±63º/s vs. 394±131º/s; p=0.036) and peak glenohumeral joint internal rotation angular velocity (247±259º/s vs. 1072±69º/s; p=0.036) during the stick deceleration phase, respectively (Figure 5).
DISCUSSION
This study found that wheelchair lacrosse players with SCI (SCI) exhibited significantly different upper extremity biomechanics that able-bodied lacrosse players seated in a wheelchair (AB-WC) and standing (AB-Standing). Thorax axial rotation angle at maximum elbow extension was significantly smaller in the SCI group than the AB-Standing group. Deficits in thorax axial rotation during overhead throwing in able-bodied lacrosse are related to decreased shoulder range of motion and angular velocity, which are associated with pain and pathology [10]. Participants in the AB-Standing group transitioned from thorax axial rotation toward the dominant arm at crank back to axial rotation toward the non-dominant arm at maximum elbow extension. However, when the same participants performed the throw in a wheelchair, they exhibited less thorax rotation toward the dominant arm at crank back and did not rotate as far toward the non-dominant arm at maximum elbow extension. The SCI group exhibited the least thorax axial rotation toward the dominant arm at crank back and did not transition toward the non-dominant arm at maximum elbow extension. The differences in thorax rotation between the AB-WC and AB-Standing groups suggest that the wheelchair acts as an extrinsic factor to limit thorax axial rotation during the throw. Further deficits in thorax axial rotation in the SCI group indicates decreased thorax control due to SCI and even more so limits the amount of thorax axial rotation during the overhead throw, which can alter upper extremity joint kinematics. Although not statistically significant, glenohumeral joint abduction and external rotation were greater in the SCI group than the AB-Standing group during crank back (Figure 3). Glenohumeral joint abduction and external rotation are considered high-risk joint orientations for injury in overhead sports, such as baseball and tennis. These joint positions place the shoulder in a compromised and unstable situation that predisposes an athlete to significant stress placed on the soft tissues of the anterior glenohumeral joint, which can result in pain and injury [11]. Decreased upper extremity range of motion is also associated with pain and pathology in overhead sport athletes [10]. We found the SCI group exhibited significantly smaller ranges of motion in thorax axial rotation compared to the AB-WC and AB-Standing groups and glenohumeral joint adduction-abduction compared to the AB-Standing group. Although not statistically significant, glenohumeral joint internal-external rotation range of motion in the SCI group was half of that of the AB-Standing group, respectively (30±23º vs. 61±30º). However, the SCI group did exhibit greater wrist ulnar-radial deviation range of motion than the AB-WC group (p=0.036) and the AB-Standing group (Figure 4). Greater wrist range of motion may be a compensatory strategy to overcome deficits in thorax and glenohumeral joint range of motion; however, further research is needed to support this. Similar to joint ranges of motion, thorax and glenohumeral joint angular velocities were significantly smaller in the SCI group than the AB-Standing group during the stick acceleration and deceleration phases (Figure 5). These findings align with previous research that found wheelchair tennis athletes exhibited smaller angular velocities than able-bodied tennis athletes [12].
CONCLUSIONS
This study successfully quantified upper extremity joint kinematics in wheelchair lacrosse athletes with SCI and compared them to able-bodied lacrosse athletes. We found that wheelchair lacrosse athletes with SCI exhibit decreased thorax and glenohumeral joint ranges of motion and angular velocities and increased glenohumeral joint abduction and external rotation, which are associated with injury in overhead athletes. The results of this study provide foundational knowledge regarding potential safety concerns or areas to improve training in wheelchair lacrosse. Future research is warranted to further investigate the relationships among upper extremity joint kinematics, pain, and injury risk in wheelchair lacrosse.
REFERENCES
- National Spinal Cord Injury Statistical Center. (2020). Spinal Cord Injury Facts and Figures at a Glance Birmingham. AL: National Spinal Cord injury Statistical Center.
- Sisto, S. A., & Evans, N. (2014). Activity and fitness in spinal cord injury: review and update. Curr Phys Med and Rehabil Rep, 2(3), 147-157.
- Kim, W., Lee, L., Lans, D., Tostenrude, D., & Lee, K. (2018). Perception of employment by the veterans participating in the national veterans wheelchair games: a survey study. PM&R, 10(3), 263-268.
- Akbar, M., Brunner, M., Ewerbeck, V., Wiedenhöfer, B., Grieser, T., Bruckner, T., ... & Raiss, P. (2015). Do overhead sports increase risk for rotator cuff tears in wheelchair users?. APM&R, 96(3), 484-488.
- Webb, M., Davis, C., Westacott, D., Webb, R., & Price, J. (2014). Injuries in elite men's lacrosse: an observational study during the 2010 world championships. Ortho J Sport Med, 2(7).
- Schnorenberg, A. J., Slavens, B. A., Wang, M., Vogel, L. C., Smith, P. A., & Harris, G. F. (2014). Biomechanical model for evaluation of pediatric upper extremity joint dynamics during wheelchair mobility. J Biomech, 47(1), 269-276.
- Hanks M.M., Brewer L.E., Gilmer G.G., & Oliver G.D. (2018). The Influence of Self-Selected Protective Equipment on Kinematics in Youth Lacrosse Players. Sport Med Rehabil J, 3(2).
- Wu, G., Van der Helm, F. C., Veeger, H. D., Makhsous, M., Van Roy, P., Anglin, C., ... & Buchholz, B. (2005). ISB recommendation on definitions of joint coordinate systems of various joints for the reporting of human joint motion—Part II: shoulder, elbow, wrist and hand. J Biomech, 38(5), 981-992.
- Mercer, J. A., & Nielson, J. H. (2013). Description of Phases and Discrete Events of the Lacrosse Shot. Sport J, 16(1).
- Wasser, J. G., Chen, C., & Vincent, H. K. (2016). Kinematics of shooting in high school and collegiate lacrosse players with and without low back pain. Ortho J Sport Med, 4(7).
- Kuhn, J. E., Huston, L. J., Soslowsky, L. J., Shyr, Y., & Blasier, R. B. (2005). External rotation of the glenohumeral joint: ligament restraints and muscle effects in the neutral and abducted positions. J Shoulder and Elbow Surg, 14(1), S39-S48.
- Reid, M., Elliott, B., & Alderson, J. (2007). Shoulder joint kinetics of the elite wheelchair tennis serve. British J Sport Med, 41(11), 739-744.
ACKOWLEDGEMENTS
This research was supported by the Medical College of Wisconsin, Department of Physical Medicine and Rehabilitation, Research Grant. We would like to thank members of Milwaukee Eagles Wheelchair Lacrosse and the UWM Mobility Lab for participating in the study.