A Foldable Wheelchair Seat for Easier Restroom Access
Nick deGrasse![]() 1
1![]() , W. Jong Yoon
, W. Jong Yoon![]() 2
2![]()
![]() 1
1![]() University of Washington Seattle,
University of Washington Seattle, ![]() 2
2![]() University of Washington Bothell, Mechanical Engineering
University of Washington Bothell, Mechanical Engineering
INTRODUCTION

Today, wheelchair users face difficulties when accessing the restroom. The most common method of using a toilet with a foldable wheelchair is for the user to move out of their seat, and transfer themselves to the toilet using some common transfer techniques [1]. Attempting this requires dexterity that not all patients have, and involves a risk of falling or injuring oneself, in a setting where help may not be immediately available. Thus, many wheelchair users choose not to use a public toilet out of fear of embarrassment or injury.
There are mechanical lifting mechanisms which will transfer the user, however they require expensive and complicated infrastructure not present in most restrooms. Assistants sometimes are present to help transfer users from their seat to the toilet, which removes risk of injury, and allows users to use all toilets, however this requires dependency, removes privacy, and comes with a high cost. Toilet wheelchairs with a permanent opening (Fig. 1) [2] are another solution, which solves the issue of high cost, and lack of autonomy and privacy. These wheelchairs often require the users to sit on a permanent opening, which is placed high enough that the user can roll over the toilet when they want to use the restroom. This approach still has a risk of falling, as the users high seated position means that they are at risk of tipping while regularly using their chair. In addition, being forced to sit on a permanent opening means that the users comfort suffers, and they are left open to health risks associated with sitting on a permanent opening.
![Rollover wheelchair normal height (top) and raised to back over toilet (bottom) demonstrating another approach to a wheelchair with toilet access [3]](66_deGrasse/Fig2.png)
A foldable wheelchair (Fig. 2) designed to raise and lower the patient over the toilet, is a solution to the tipping issue, as the user can be lowered to a normal height while the chair is not in use [3]. This would allow the patient not to leave their seat, however this wheelchair under development is lacking a seat which opens and shuts, allowing the user to access the toilet below.
![The Reswick Rogers (1976) pressure-time curve [7], used to determine risk of injury given time and applied pressure to a persons skin. Does not hold up for very long (1) or short (2) periods of time](66_deGrasse/Fig3.png)
In order for this solution to work, it needs a seat which can be affixed to the wheelchair that allows access to the toilet below. The seat must be foldable like the wheelchair itself, it must support the user, to promote comfort and mitigate health risks, and it must be mechanical, to make the system cheap and simple to operate.
Preliminary Study
![Sitting behavior of full-time wheelchair users histogram [8]. Half of the days studied included at least a 2 hour period of time between wheelchair users shifting their weight](66_deGrasse/Fig4.png)
When considering health risks for the wheelchair seat design, our two main focuses were pressure sores and hemorrhoids. Pressure sores are caused by insufficient seat support, which can cause injuries to a person's skin tissue from prolonged applied pressure and are common in wheelchair patients and the elderly [4]. Hemorrhoids are caused by uneven support in seating, which can impede blood flow. This uneven support can be characterized by a large coefficient of variation (COV), which suggests pressure is focused on a few select areas, as opposed to evenly distributed across the users bottom. Devices such as hemorrhoid cushions have been shown to increase the severity of hemorrhoids [5], and increasing time spent seated on openings such as a toilet seat has been shown to increase the prevalence of hemorrhoids as well [6], as both impede even blood flow and offer uneven support. Because of this, it is expected that a permanent opening in a wheelchair seat will increase a patient's likelihood of hemorrhoids and pressure sores. In order to discover a safe limit for pressure the patient can experience while using the wheelchair seat design, the Reswick and Rogers pressure time curve was used (Fig. 3) [7]. The curve was the result of a 1976 study which evaluated the prevalence of pressure sores in 980 hospital patients, based on the severity and cause of their pressure sores. This study resulted in an equation (1) which related pressure, time, and danger of pressure sores.
(1)
Pressure sores are based on many factors such as age, patient physiology, and internal pressure, however this is considered a general guideline, though it is not used in clinical decision making due to high variability among patients and little control over loading conditions. The curve does fail at significantly short (Fig. 3, point 2) and long (Fig. 3, point 1) time periods. As time approaches zero, the tolerable pressure level approaches pressure levels capable of tearing tissue from blood vessels (600mmHg), and as time approaches 14+ hours, the calculated tolerable pressure becomes too low to cause pressure sores in most patients [7].
In order to find a tolerable pressure from the Reswick and Rogers pressure-time curve, a study evaluating the weight shifting behavior of 28 individuals across 192 days who were full-time manual wheelchair users was used [8]. The study evaluated the time between weight shifts (WS's, "defined as 30%-90% off-loading of at least one side of the buttocks for 15 s") and pressure reliefs (PR's, "90% off-loading of the entire buttocks for at least 15 s"), and gives data on how long users should expect to experience consistent loading. Fig. 4 compares the time between WS's or PR's in minutes, against how many days each time range was recorded during this 192 day study. The study resulted in a fair amount of variability between each patient; Fig. 4 shows that half the days studied included at least a 2 hour period between weight shifts, making 2 hours a good choice as it represents the median time, and occurs almost as frequently as the 80 minute time period.
Combining the Reswick and Rogers pressure-time curve (Fig. 3) and the study from Fig. 4, tolerable pressure is 150 mmHg, as calculated in equation (2). This pressure was used as a general guideline for resulting designs, and was considered an upper limit for measured pressures.
Prototype development
The two seating control setups were the normal seat, and the seat with an opening. Solutions which have support similar to the normal seat are to be considered adequate, whereas solutions with support similar to the seat with an opening are to be considered inadequate.
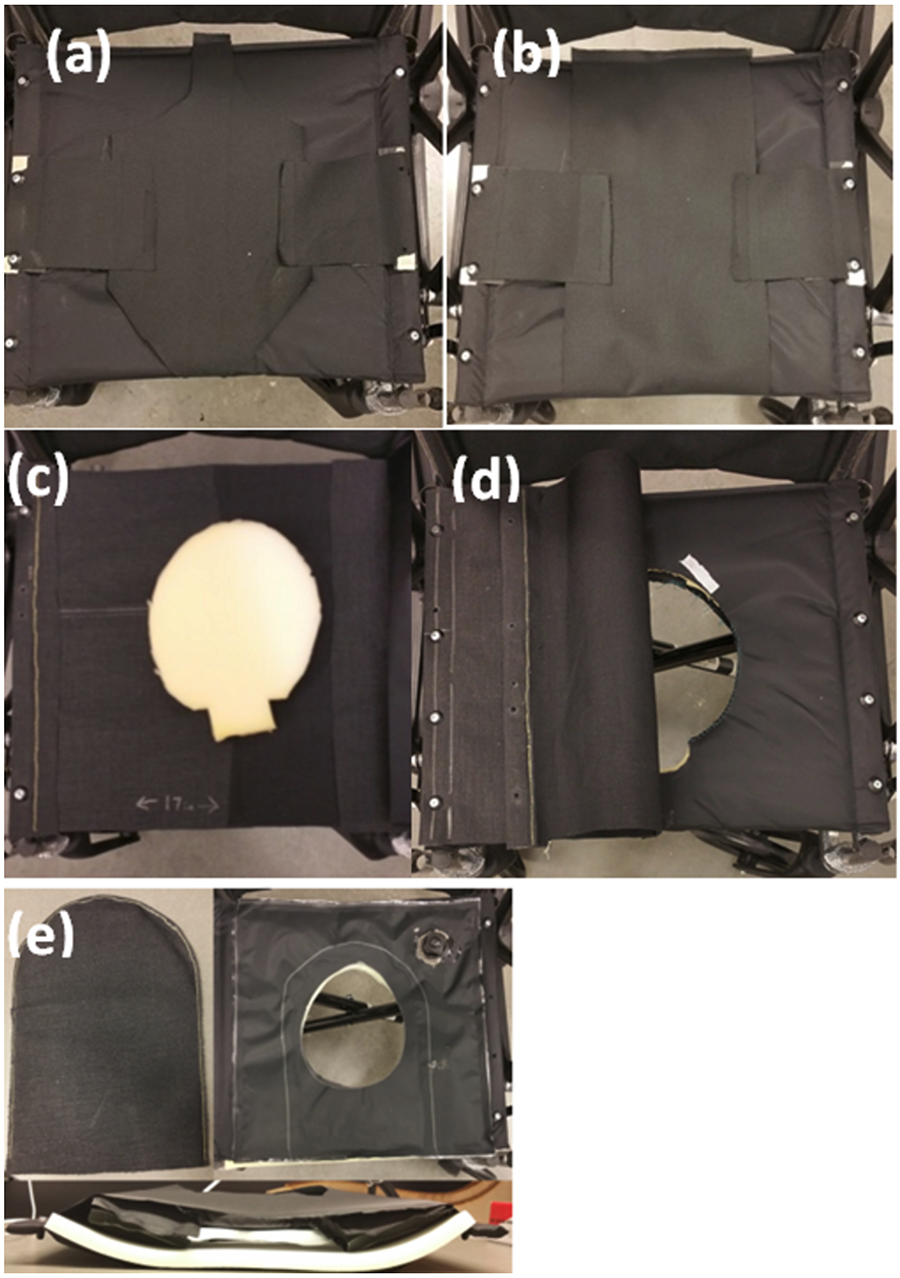
Five prototypes were created (Fig. 5) with different approaches to open and close an 8.5x7 in ovular opening in the wheelchair seat, which was made from about 2-inch thick polyurethane foam, between layers of flexible nylon fabric.
The first systems are layers which wrap around the seat to cover the opening, and can be moved aside to allow access to the opening (Fig. 5 a, b). The next design was the under-seat removable layer, which used a layer of nylon fabric wrapped underneath the seat, with polyurethane foam on top to fill the opening (Fig. 5 c). The layer can be attached and unattached in order to apply support, and to allow restroom use. This functionality requires a fastening system. The layer on top was a layer of fabric along the top of the seat, which users would have to move to the side to utilize the opening (Fig. 5 d). The pull tab, which used an acrylic fabric covered tab large enough to cover the opening, sandwiched between the fabric layers of the wheelchair seat, held in place by the user's weight. In order to remove the tab, and access the opening, the user will use an inflatable device to reduce pressure on the tab, allowing them to remove it from the seat (Fig. 5 e).
Measurements
Upon making prototypes of each design, a testing process was created to evaluate each designs support level. The testing process used the pressure mat (Boditrak, Winnipeg MB, Canada), and FSA 4.1.1, a program which creates visual maps of support, and will store information such as max pressure and COV for a trial.
The testing process used was to first set up each prototype in its 'closed' position, set the mat on the seat, and use FSA to record data. FSA was set to record at a rate of 2Hz. The tester then sits on the mat, waits 2-3 seconds for the initial spike in pressure from sitting down to stabilize, then records pressure data for 10 seconds which results in 20 data points. This measurement process is repeated seven times, and then data is exported to Excel, where the max pressure and COV for each of the 20 frames from each trial are averaged. The max pressure value, is simply the max pressure measured across all pressure sensor cells at a certain instance. COV, is the standard deviation divided by the mean of all pressure sensing cells on the mat. This averaged value across the 20 frames per each trial, results in a single max pressure and COV value for each trial. Each round of testing was conducted with just one user, for consistency. Max pressure and COV for these 7 measured trials were compared to the control setups using ANOVA testing to determine if solutions were statistically determinate from one and another, as well as comparing the max pressures from testing to our target value (150 mmHg). This will determine whether there is a location on the prototype where pressure exceeds our allowable value before pressure sores begin to occur.
RESULTS
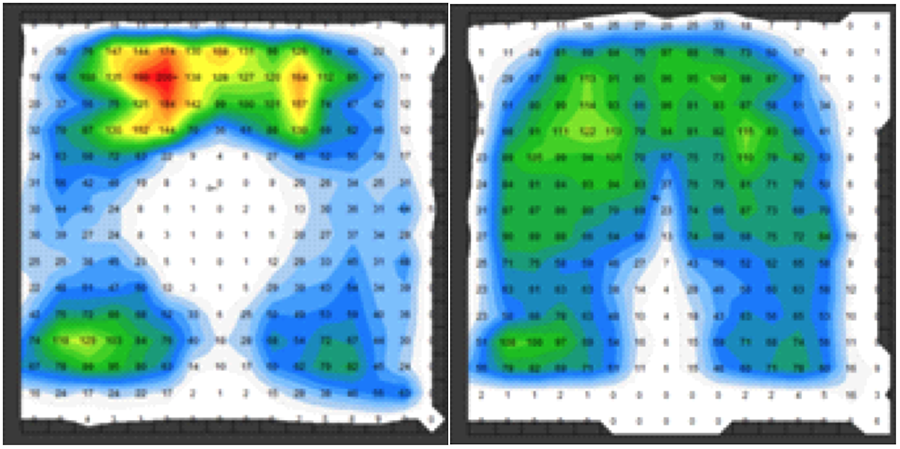
The seat with a permanent opening lacked support primarily in the midsection of the thighs, where pressure was generally around 40 mmHg (Fig. 6, left). The opening provided no support. Pressure was slightly focused near the front of the thighs (65-130 mmHg), but primarily in the tail bone and buttocks (120-200+ mmHg), where most of the weight is focused on, as there are bony protrusions. The normal seat (Fig. 6, right) provided the best support level, With 6 of 7 trials below the target pressure of 150 mmHg, a median pressure of 132.02 mmHg, and an average of 129.18 mmHg. The rest of the solutions, besides the layer under the seat, did not manage to yield a median max pressure below the target. The layer under the seat had only one trial above our target pressure, and had similar results to the normal seat in both max pressure (P = 0.384) and COV (P=0.30).
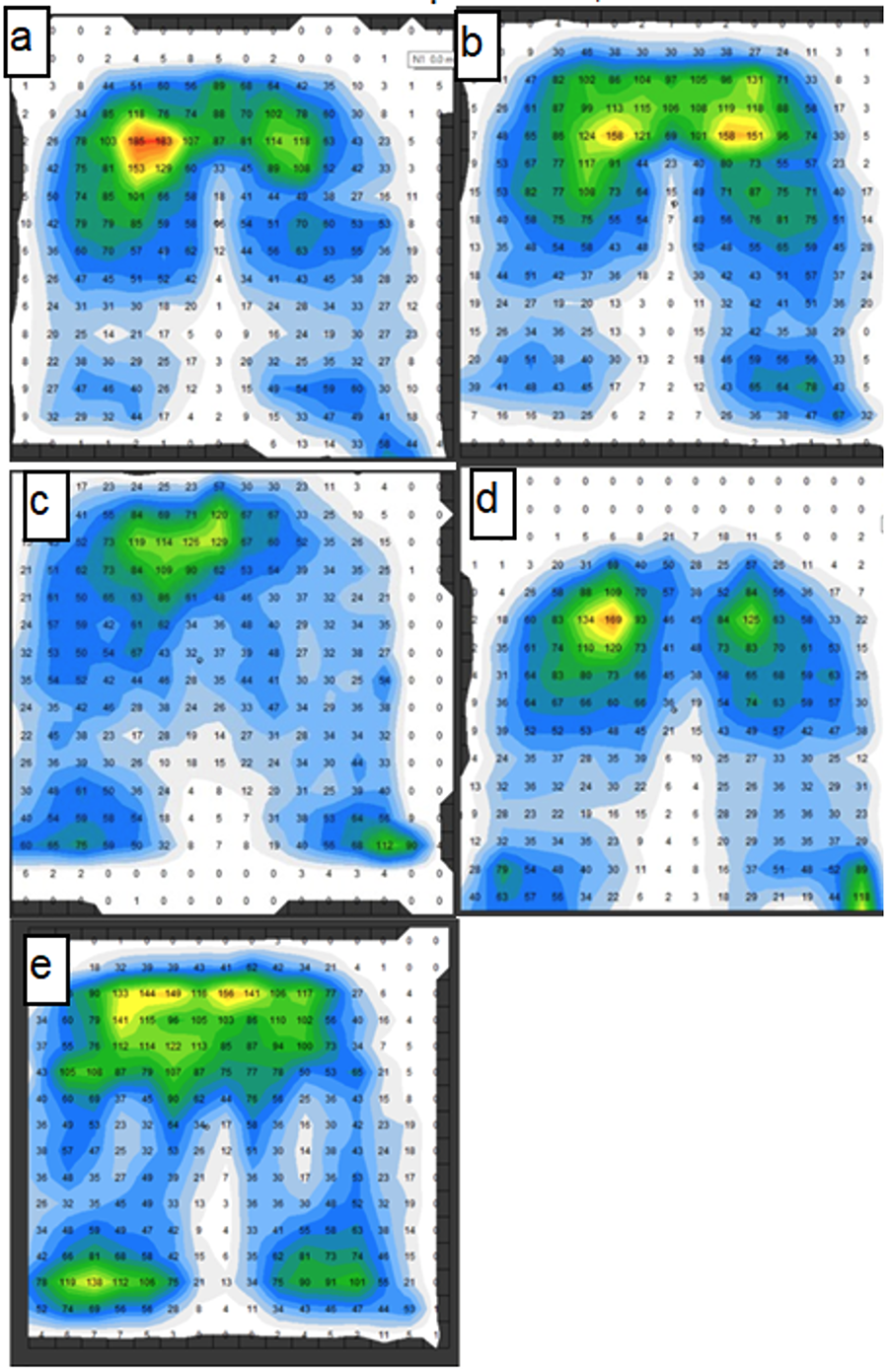
The slim and wide wrap around layers had a support pattern very similar to the seat with a permanent opening, meaning they lack the ability to provide support to the user in the space where the opening is present (Fig. 7 a, b). The max pressure for the slim wrap around layer ranged from 151.47 mmHg to 200 mmHg, and the max pressure for the wide layer ranged from 132.58 to 184.44 mmHg, showing that the wide wrap around layer did have some advantage over the slim layer; however its median max pressure (161.25 mmHg) suggests it's above our allowable pressure level. The slim and wide wrap around layers also had median COV values of 104.35% and 95.23%, which is similar to the seat with a hole (median COV 106.35%).
The layer under the seat provided a very similar support layout to the normal seat in max pressure (p = 0.384), as pressure was distributed well across the users' thighs and buttocks, which resulted in a median pressure of 138.99 mmHg, meaning this solution was within our allowable support level (Fig. 7 c). It also had a median COV of 83.25%, which is the lowest of all prototypes.
The layer on top of the seat also showed similar results to the permanent opening, with much of the pressure being focused on the buttocks of the user, and a lack of support in the area the hole is present (Fig. 7 d). This solution had a max pressure range of 105.85 to 184.65 mmHg, with a median of 173.21 mmHg, suggesting it also exceeds the allowable max pressure. It had a median COV of 93.09%.
The pull tab did provide more support than the seat with a permanent opening, as its pressure map shows more support focused on the thighs, and less at the buttocks. There is still an unsupported region across the middle of the thighs however (Fig. 7 e). The pull tab had a median max pressure of 151.7 mmHg, meaning that while it is close to our allowable pressure, it is still outside of the range. Its mean COV was 86.73%.
DISCUSSION
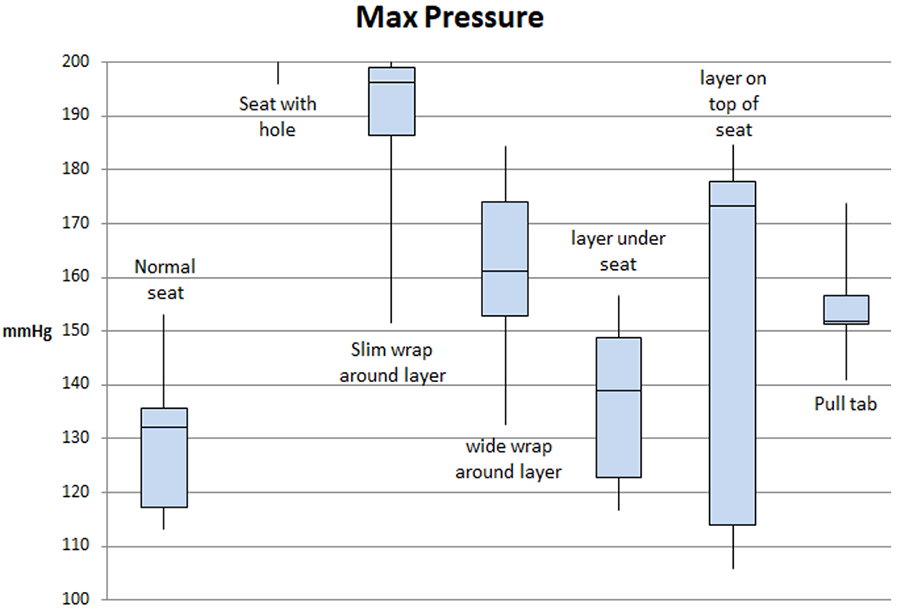
The Boditrak pressure mat used only had the capability to measure pressure up to 200 mmHg, meaning it's possible some of the prototypes gave off pressure levels above this which couldn't be recorded. The seat with a hole and the slim wrap around layer both had medians which were at or close to 200 mmHg, suggesting it's possible that both setups experienced pressures exceeding the devices capabilities (Fig. 8). It is also important to note that the hand rails present on the wheelchair had a tendency to push on the pressure map, and cause pressure spots to appear where the user was not seated. These spots did not create significant pressure as to affect the max pressure results, though it could bias COV low, as it gives the impression that pressure is being spread more evenly across the mat. The mat is also intended for longer testing periods (>1 hour), and in the case of a physician evaluating a patients seating safety this would be necessary, however as it is only being used as a tool to comparatively evaluate support, the short trial duration is of less importance.
It's also clear some prototypes had very large standard deviations, such as the layer on top of the seat, and the slim wrap around layer. For reference, the normal seat and layer under the seat had standard deviations in max pressure of 14.23 and 15.96 respectively. Some of this could have been accounted for by using longer trial times, but changes in sitting habits could have also had an effect. There was not a standard for posture, which was done to account for different sitting positions of different users. The high variability of some setups suggests longer testing or more consistent testing may be necessary. Testing for longer periods of time, and with standardized postures within the same time frame could yield more accurate results.
The methods are not accurate enough to evaluate clinical risk for each seating solution, nor are they meant to. They are however viable methods to compare the support levels of each seating solution prototype, and have shown that the removable layer under the user's seat provides similar levels of support to a standard foldable wheelchair seat.
CONCLUSION
The roll-over-toilet wheelchair is a solution which mitigates these problems, however still requires an adequate opening and closing mechanism to allow access to the toilet below. The testing methods mentioned above evaluated 7 different seating situations, and found that the seat with a permanent opening was not a viable solution, as it exceeded what was considered a safe pressure for the user. Of the 7, only two had a median max pressure which was within an acceptable range, the normal wheelchair seat, and the layer beneath the seat. Although a suitable seating solution was created, and has been evaluated to provide similar support levels to the normal folding wheelchair seat, the seat still requires feedback from likely wheelchair users. Creating a usability feedback survey and conducting subject experiments to guide the future iterations of this solution is necessary.
REFERENCES:
- "Toilet Transfer Techniques." Access Board, United States Access Board, www.access-board.gov/guidelines-and-standards/buildings-and-sites/about-the-aba-standards/ufas.
- Mariner Rehab Shower Commode Chair. Invacare. Catalog listing for Invacare commode wheelchair
- W. Jong Yoon, Mohamed Shakir, Yasir Salih Osman, Design and Development of a Smart Multifunction Toilet Wheelchair (SMTW), 15th International Conference on Ubiquitous Robots (UR), June 27-30, 2018, Hawaii, USA
- Mayo Clinic Staff, "Bedsores (pressure ulcers)," The Mayo Clinic, 09-Mar-2018. [Online]. Available: https://www.mayoclinic.org/diseases-conditions/bed-sores/symptoms-causes/syc-20355893. [Accessed: 28-May-2019].
- "Will sitting on a doughnut help or hurt hemorrhoids?," Beverly Hills Hemorrhoid Surgeons and Proctologists, 17-Apr-2019. [Online]. Available: https://lacolon.com/article/will-sitting-doughnut-help-hurt-hemorrhoids. [Accessed: 29-May-2019].
- T. C. B. Dehn and M. G. Kettlewell, "Haemorrhoids And Defaecatory Habits," The Lancet, vol. 333, no. 8628, pp. 54–55, Jan. 1989
- Gefen A (2009) Reswick and Rogers pressure-time curve for pressure ulcer risk. Part 1. Nursing Standard. 23, 45, 64-74. Date of acceptance: February 13 2009
- Sonenblum, Sharon E., et al. "Everyday Sitting Behavior of Full-Time Wheelchair Users." Journal of Rehabilitation Research & Development, vol. 53, no. 5, June 2016, pp. 585–597. EBSCOhost, doi:10.1682/JRRD.2015.07.0130.