INTRODUCTION
Children with visual impairments may face challenges in their education and daily life. These areas become intertwined as learning motions for daily activities are a central aspect of the education of children with visual impairments. The Western Pennsylvania School for Blind Children (WPSBC) educates approximately 200 students and provides vital early intervention and outreach services to visually impaired students, who may have additional physical, cognitive, and emotional challenges [1]. Therapists and teachers work with students using FOCUS (Functional Outcomes-based Curriculum for Unique Students) to address core subjects and the skills necessary to enhance independence and quality of life [1].
Students from the WPSBC often experience limitations during feeding and painting exercises, specifically the lack of independence due to the hand-over-hand style used by therapists to guide activities. Since assistive technology impacts the target group positively, can a universal attachment device separate the hands of students and therapists while improving their learning experience and assessment abilities? Our team designed a universal attachment device to enhance client independence and improve therapist's guidance for a comfortable feeding and painting experience.
METHODS
The framework for the design methodology was based on human-centered design and incorporated observation, development of an experience map, needs generation, concept generation and selection, benchmarking, and specification development. In lieu of in-person observations, the group received demonstration videos from the team of therapists that were our main points of contact at the WPSBC. The videos presented how the universal attachment would be used with the children and avoid hand-over-hand motion exercises and detailed the actual hand-over-hand use of a utensil by a student to help the team identify the key issues to address. These student and therapist observations led us to identify what needs were required to solve these issues related to grip strength, comfortability, adaptability, and washability. These needs are listed as follows:
- The universal attachment device separates the therapists' and users' hands.
- The universal attachment device allows students to learn feeding and painting motions comfortably.
- The universal attachment device provides a better assessment of the user's progress.
- The universal attachment device accommodates a range of items for feeding and painting.
- The universal attachment device is washable for sanitation and reuse.
- The universal attachment device is hypoallergenic.
Concept Generation and Selection
After identifying specific needs, the team generated various design concepts for the universal attachment device. The common components of each concept comprised of handles for both the therapists and users connected by a ball and socket joint. The ranking matrix in Appendix Figure 4 was used to gauge the success of other design elements. This led us to incorporate a silicone grip for the user as well as consider both a clamping mechanism and inserts for the utensil attachment. This final concept can be seen in Appendix Figure 5.
Benchmarking
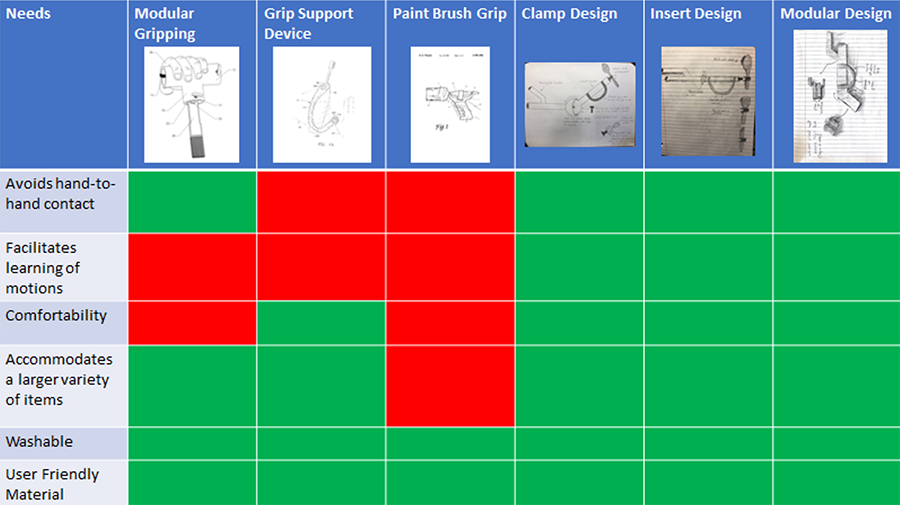
Three benchmarking products were identified and compared to our designs by how well each design conceptually fulfilled the client's needs. A modular gripping handle, grip support device, and a paint brush handle were great for attaching various utensils and providing assisted grips, but lacked any components that promoted the guidance and instruction of motion exercises in the design. Only the concepts designed by our team incorporate these instructional capabilities into the function of the device, adding more significance to its fabrication. Appendix Figure 6 shows our benchmarking matrix.
Specifications
Device specifications were defined in order to give the needs and design concepts specific metrics and testing methods. This builds the framework for analyzing how acceptable the functional prototypes are for the users, both the students (clients) and therapists (providers). Our specifications are outlined in Appendix Figure 7. In order to make the Universal Attachment more functional for both users, the team decided to use the following metrics; making the protype safe and washable, measuring the time it takes to clean the device, allow the Universal Attachment to have different positions for the user handle, the clamp to be able to hold at least 3 items and measure the different parts of the Universal Attachment to figure out the correct size of the product for both users.
Usability Scale
Using the identified device requirements, the team developed a usability scale that consists of 17 questions to address both provider and client responses, as well as specific features of the device. Examples of questions include overall satisfaction with the device, ease of learning how to operate the device, support and comfortability of the handles, student enjoyment and initiation of use, and the ability of the device to meet individual student and therapist goals. Data was also collected on how ease of cleaning the device and device durability, which were important needs identified early on in the design process. A Likert scale was used to obtain data, with 1 representing strongly disagree and 5 representing strongly agree, as well as a "not applicable" option. The survey also asked for reports on how long it took to clean the device after each use, what percentage of the therapy time the client was able to use the device, and approximately how long the client was able to grip the device before it needed to be readjusted by the provider. A comments section was also included to obtain feedback from therapists and teachers that used the universal attachment. Due to the nature of the student population at WPSBC, most of the students are non-verbal and the provider interpreted the student's feelings about the device when reporting feedback. This combination of objective and subjective information guided prototype designs and provided a means to compare data between prototype iterations.
DESIGN & OUTCOMES
1st Prototype

After determining the proper design elements of the device, it was time to assemble the materials and fabricate the first prototype. The therapist handle was created by cutting PVC rod stock to 6" on a bandsaw, then using the lathe to bring it down to 1.5" diameter and creating a notched insert on the end to secure the ball & socket element. The ball & socket joint was tightened over the handle, and the aluminum client handle with the silicone grip was secured to the joint and the clamp mechanism using ¼"-20 screws. The device weighed 1.86 lbs. The fully assembled prototype can be seen in Figure 2.
The research team received usability feedback from four surveys for Prototype 1. Average scores from the surveys are depicted in Figure 4 and Table 1 in the appendix. The highest average scores were ease of cleaning and durability of the device, both with an average of 4.25. The lowest average scores were facilitator satisfaction with the device, client improvement toward individual goals, and client initiating grasp of the device (all three had average = 2). The average amount of time it took to clean the device was 53 seconds, and the average percentage of time the students used the device within each feeding session was 37.5%. Throughout the survey, some questions were left unanswered because they did not apply to the student (i.e., client enjoyment or initiation of use). Due to the small sample size, it is unclear whether this was dependent on client temperament, or if the survey needed to be adjusted for more accurate data collection. Common themes from the written feedback section of the questionnaire included the heavy weight and large profile of the device which was distracting and tiring to the students.
2nd Prototype

Feedback from the first prototype provided us with design changes to focus on for the next iteration of the product. Making the device lighter weight, compact, and designing a new client handle and clamping mechanism to facilitate accurate hand placement were our primary objectives. We achieved this by acquiring new joint and clamp elements used in microphone setups to provide more range of motion and attaching a ¾"x 6" PVC pipe to the clamp for the client handle. The pipe was packed tightly with plastic brush bristles so that the utensil would displace the bristles and create a tight hold on the handle of the utensil. This updated version of the device weighed 1.02 lbs. The fully assembled prototype can be seen in Figure 4.
Final Prototype
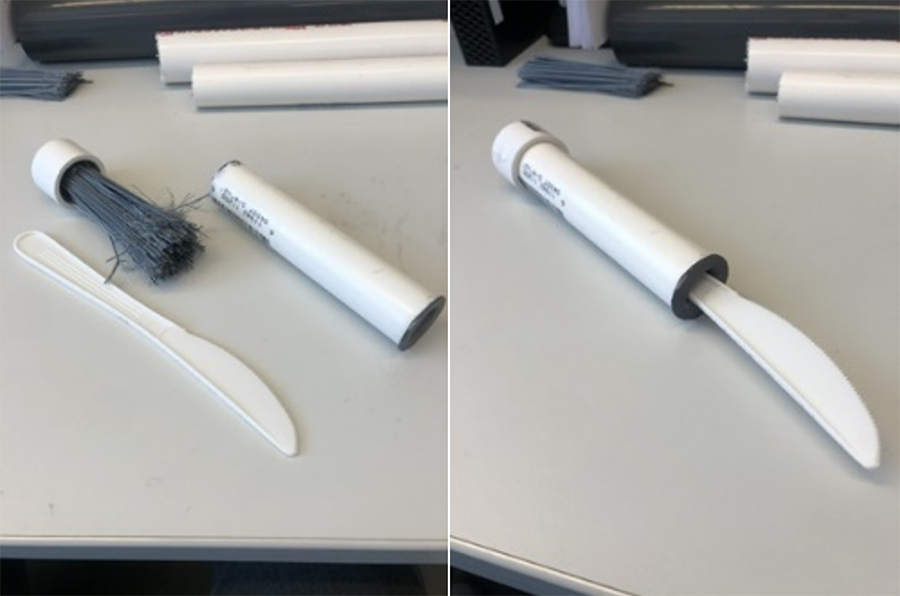
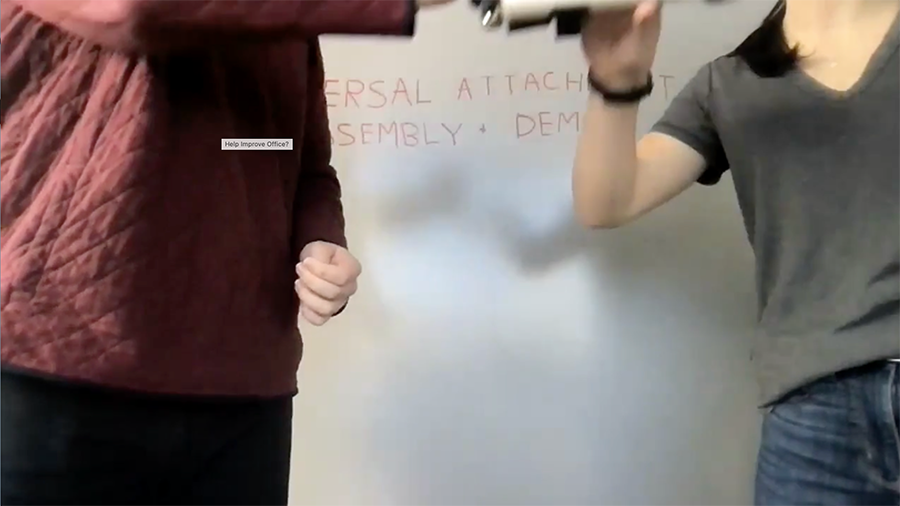
Based on feedback received virtually by our stakeholders, the team worked to optimize the client handle of the device. This was accomplished by gluing the plastic brush bristles to the inside of a ¾" PVC cap and creating a rubber guard with a slit on the other end for utensil insertion. The result was a cleaner looking handle that also increased its functionality and washability as seen in Figure 3. Functional use of the prototype can be seen in Appendix Figure 9 and Figure 10.
The cost of the fabrication for a single universal attachment device is listed below in Table 2, which comes out to an estimated total of $39.76.
| Material | Cost ($) |
|---|---|
| 1" x 6" PVC Pipe | .60 |
| ¾" x 6" PVC Pipe | .41 |
| 1 ½" Dia. x 6" PVC Rod | 3.26 |
| ¾" Dia, PVC Cap, Unthreaded | .83 |
| Plastic Bristle Broom Head | 8.97 |
| Clothespin-Style Plastic Mic Clip | 5.95 |
| Locking Ball Socket Adapter | 12.75 |
| Silicone Adaptive Grip | $6.99 |
| TOTAL | $39.76 |
DISCUSSION
The team created a functional universal attachment prototype that was delivered to the client, and further improvements will be continually added following this April 2021 submission. The initial prototypes were only used for feeding exercises; however, the research team hopes that the "universal" part of the device can be expanded to accommodate other utensils to facilitate instrumental activities of daily living including brushing teeth, brushing hair, baking, and gardening, and a variety of other activities. This device is significant to the user and therapist in many ways. The device will allow patients to have a sense of independence when learning tasks using various utensils, while the therapist will still be able to aid and assess these activities.
Several challenges were encountered during this process, primarily due to COVID-19 restrictions. In-person observations were not feasible, and all conversations between the design team, design course professors, and WPSBC therapists were completed over Zoom conferencing to gather the appropriate information. Considering the nature of the student population, most of whom are non-verbal and lack the cognition to fill out a paper questionnaire, in-person or even video observations of the device being used by students and witnessing their disposition towards the device would have been beneficial. While face-to-face observations would have provided a more in-depth understanding of the client's diverse set of needs, virtual conversations and survey feedback allowed us to gauge the needs of the students and therapists. COVID-19 also limited the amount of time the therapists were able to trial the universal attachment with their students as they often had to go remote. The team anticipated collecting more data on Prototype 2 and the final prototype in order to compare scores between the three device updates, but the reduced amount of in-person time at the school limited this opportunity. Additionally, no data was collected for painting activities in addition to feeding exercises. Future work should focus on the comfortability of the device and the incorporation of other utensil exercises.
CONCLUSION
Students from the WPSBC experience limitations with their feeding and painting exercises being accurately guided and lack independence due to the hand-over-hand style used by therapists. Based on various discussions in regard to prototype function, the team designed a concept that attempted to accommodate the identified user needs. Throughout this process, many of the specific parts of the device were altered to accommodate changes in client needs, availability of building materials, and feasibility of construction. Virtual collaboration with WPSBC provided various roadblocks due to the challenges of navigating life in a pandemic, but the adaptability of University of Pittsburgh design students, faculty, and the therapist team is greatly appreciated. Regarding the future of the universal attachment device, the research team aims to continue collaborating with the therapists and clients and improving on previous design concepts. Our goal is to create a design that can be easily replicated with low-cost materials by families, teachers, and therapists to support people with disabilities in achieving a level of independence in their daily activities.
APPENDIX
| Ranking Matrix |
|
Concept 1 | Concept 2 | Concept 3 | Concept 4 | Concept 5 |
|---|---|---|---|---|---|---|
| User Needs | Weight | Silicon Grip | Utensil Inserts | Clamp | Ball & Socket | Modular |
| Avoids hand-to-hand contact | 25 | 1 | 3 | 3 | 3 | 3 |
| Facilitates learning of motions | 20 | 1 | 3 | 3 | 4 | 3 |
| Comfortability | 10 | 5 | 2 | 3 | 5 | 3 |
| Accomodates a larger variety of items | 5 | 1 | 5 | 5 | 4 | 3 |
| Washable | 10 | 5 | 4 | 3 | 4 | 5 |
| User-friendly material | 10 | 5 | 5 | 4 | 3 | 3 |
| Easy assessment of user progress | 20 | 5 | 5 | 3 | 4 | 3 |
| Total | 100 | |||||
| Average | 3 | 3.7 | 3.2 | 3.75 | 3.2 | |
| Rank | 5 | 2 | 4 | 1 | 3 | |
| Continue? | Combine | Yes | Yes | Combine | Yes |
Figure 4. Ranking Matrix used for concept generation.
Figure 5. Initial concept sketch of universal attachment device.
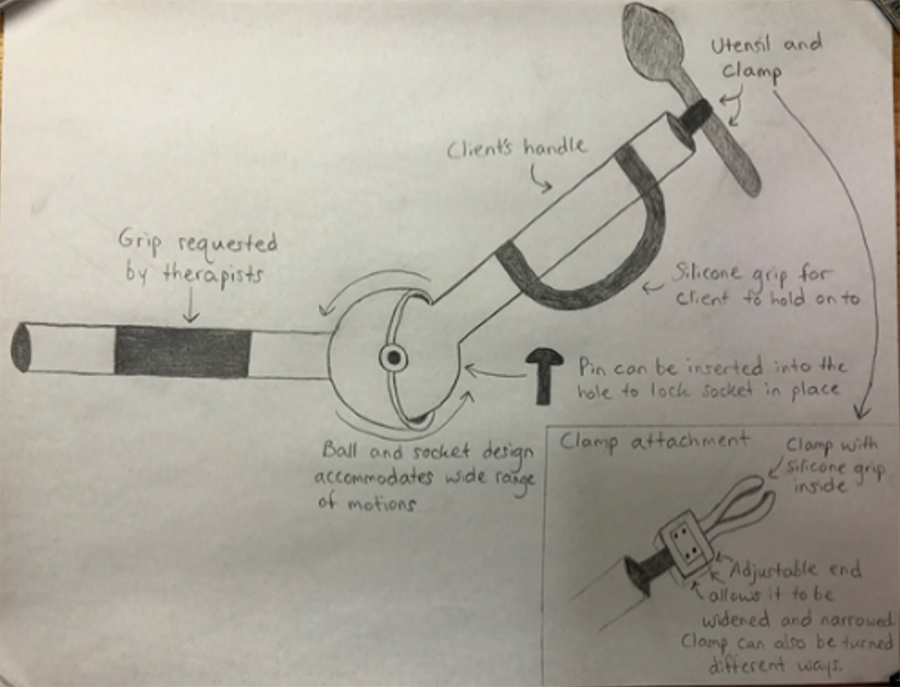
Figure 6. Benchmarking matrix used to determine their fulfillment of the user needs.
| Metric # | Need # | Metric | Importance | Units | Marginal Value | Ideal Value | Testing Methods | Lab or User Test |
|---|---|---|---|---|---|---|---|---|
| 1 | 5, 6 | Safe and washable | 1 | Y/N | Y | Y | User interaction for one week | User |
| 2 | 5 | Time to clean | 1 | Min | 3-6 min | 2-5 min | 10 washing trials | User |
| 3 | 2, 3 | Three degrees of freedom | 1 | Y/N | Y | Y | Can be locked in three different positions | Lab |
| 4 | 2, 4 | Attachment Variety | 1 | N/A | 3 | 5 | Item insertion and testing | Lab |
| 5 | 1 | Diameter of therapist handle | 2 | Inch | ± .25 in | 2.25 in | Measurement | Lab |
| 6 | 1 | Length of therapist handle | 2 | Inch | ± 1.00 in | 4.75 in | Measurement | Lab |
| 7 | 1, 2 | Diameter of user handle | 1 | Inch | ± .25 in | 2.00 in | Measurement | Lab |
| 8 | 1, 2 | Length of user handle | 1 | Inch | ± 1.00 in | 2.25 in | Measurement | Lab |
| 9 | 2, 3 | Diameter of ball & socket | 2 | Inch | ± .25 in | 2.25 in | Measurement | Lab |
| 10 | 2, 3 | Clamp length | 1 | Inch | ± .25 in | 2.25 in | Measurement | Lab |
Figure 7. Specifications for metric evaluation and testing.
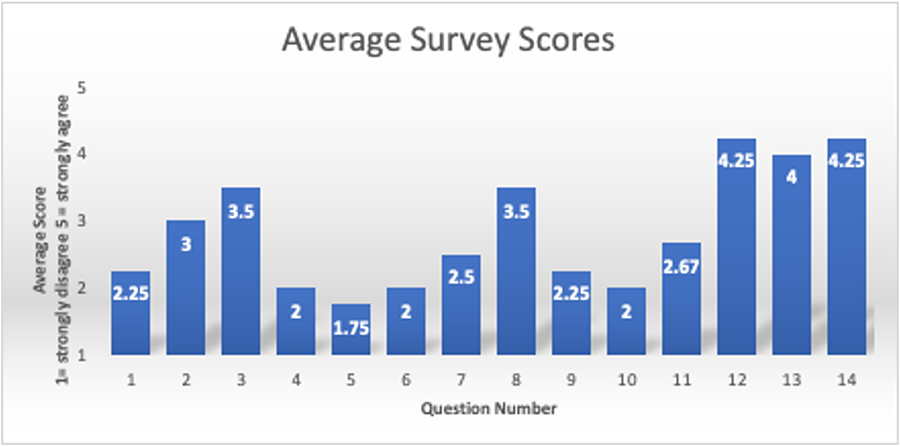
Figure 8: Average Likert scale scores for each question from the usability scale.
Survey Section |
Average Result |
Provider Score |
2.5 (out of 5) |
Client Score |
2.49 (out of 5) |
Device Score |
4.12 (out of 5) |
Device Cleaning Time |
53 seconds |
% of time used |
37.5% |
Figure 9. How to use the Universal Attachment Part 1.
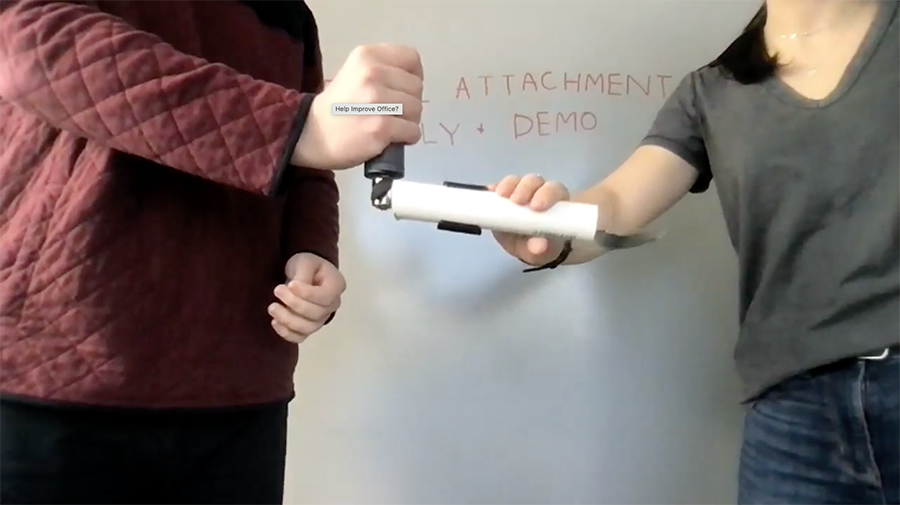
Figure 10. How to use the Universal Attachment Part 2.
REFERENCES
- Western Pennsylvania School for Blind Children Home. (n.d.). Retrieved November 19, 2020, from https://www.wpsbc.org/
ACKNOWLEDGMENTS
We would first like to express our gratitude to our professors Dr. Mhatre, Dr. Goldberg, and Dr. Pearlman for giving us the opportunity to develop rehabilitation technology that benefits both the user and therapist. They provided us with the knowledge, guidance, and feedback throughout the design process that we needed to succeed. We would also like to thank our design lab instructor, Stephanie Vasquez, for sharing her knowledge about the design process and 3D printing, as well as the feedback she provided us throughout our project development.
We would also like to extend our gratitude to the therapists at the Western Pennsylvania School for Blind Children; Stacey Resavage, Cortney Divito, and Becky Eckenrod. Their continued guidance, support, and feedback served an integral role in the development of our project design. Finally, we would like to express our gratitude and appreciation to other members of the Western Pennsylvania School for Blind Children, Mark Kislan and Molly Eads, for providing us with the opportunity to collaborate with them.