Lisa K. Simone, Ph.D.1, John A. Simone2, Roman Mitura3, Dean Klimchuk3, Maria T. Schultheis, Ph.D.1
1Kessler Medical Rehabilitation Research and Education Corporation, West Orange, NJ
2Virginia Tech, Blacksburg, VA
3Digital MediaWorks, Inc., Kanata, Ontario, Canada
ABSTRACT
Return to driving is one of the most sought after activities for individuals recovering from spinal cord injuries; without a car, employment and participation in community activities can be significantly compromised. Current driver retraining programs are limited by subjective measures, are costly and not readily available to all patients. The use of virtual reality (VR) technology for driver retraining has been identified as a possible supplement to address these needs. The goal of this research is need-driven; to develop a portable, clinician and user-friendly VR driving simulator that is cost effective and realistic. While several VR driving simulators exist, few employ adaptive equipment or have been validated using methodological studies. The focus of this paper is on the development of the custom driving hardware, including the integration of a real steering column and clinically recommended adaptive driving equipment (e.g., hand controls), interfaced to a custom driver retraining virtual environment.
KEYWORDS: driver retraining, virtual reality, spinal cord injury, hand controls
BACKGROUND/PURPOSE
This work has both research and development goals. The research focuses on using virtual reality as an intervention to improve driver retraining after spinal cord injury. Currently, driver retraining may require many one-on-one driving sessions behind the wheel with a trained evaluator. This training might not be available to all individuals, and the cost is often considered an out-of-pocket expense. The research aim of the study is to evaluate if the additional training using VR can reduce the number of evaluator-led training sessions. The protocol allows participants to practice driving, using clinically-recommended adaptive equipment, in different virtual environments of increasing difficulty over several sessions.
The development goal is to create the driving simulator hardware with adaptive equipment that is low cost, portable, and easily deployable to a wide range of sites including rehabilitation centers, doctor’s offices and outpatient facilities. Some driving simulators with hand controls have been reported. The most common configuration uses an actual car or the front half of a car containing the driver’s compartment, appropriate adaptive equipment, and a large projection screen. Peters et al. used the VTI driving simulator to evaluate driver adaptation to the special equipment by measuring performance and workload as compared to healthy controls (1). The simulator is a car body on a moving platform with a wide angle screen, and has been validated in previous studies. Ku et al. developed a simulator consisting of an actual car with appropriate adaptations, a beam projector and sound system (2). They report that fear of driving (due to the new challenge of hand controls) was significantly reduced, and that performance for individuals with SCI versus healthy controls (using normal foot pedals) was the same. Ahm et al. have also presented pilot data of a custom driving simulator using a remodeled automobile with real hand controls and a large screen (3). While these larger systems have been used successfully in research, they are not appropriate for low-cost deployment.
On the other extreme, two companies offer desktop driving simulators with hand controls. Both Simulator Systems International (Tulsa, OK) and Sim-Drive Canada (Cochrane, Alberta) offer similar systems. The hand controls option is a module mounted under the steering wheel that only mimics the mechanical control of the foot pedals, reducing the realism of the system. In addition, methodological clinical studies evaluating the usefulness of these systems in driver retraining has not been reported.
Although no standards yet exist to evaluate an individual’s ability to drive, there is some agreement that several physical parameters relating to functional performance in a dynamic interactive environment should be measured, such as steering and brake reaction time, and range of motion (4). The system developed as described below provides an interface to the software for these and other parameters.
APPROACH
In order to provide both realism, low cost and portability, the VR driving simulator is PC-based using one or three flat-screen displays, which can be large or small depending on cost and space issues. The hardware maintains the familiar steering wheel/foot pedal configuration for realism. In consultation with the Driving Program at Kessler Institute for Rehabilitation, which has participated in previous driving research projects with the investigators, an adaptive equipment configuration was defined which would meet the needs of most study candidates. This includes hand controls for acceleration and braking located to the left of the wheel, and a spinner or tri-pin knob located in one of four quadrants on the wheel (upper right, upper left, lower right, or lower left) for turning. In addition, the steering column requires a column shifter, ignition switch, turn signals, and tilt and telescope functions for realistic adjustability. For safety considerations, the steering wheel cannot contain an airbag. Other requirements include clearance for the participant in a wheelchair to access the steering wheel and hand controls.
 |
|---|
Simulators using real cars provide realism, but are not easily deployable or cost effective. Rather than using cars, the team decided to use real (production) car parts. Used and after market steering columns are inexpensive and functional; the steering column for this model is from a 1987 Cadillac DeVille and includes a working ignition switch, turn signals, column gear shifter, tilt and telescope features, and free-spinning steering wheel. Hand controls were acquired from Drive Master, Inc. (Fairfield, NJ), a company that provides automobile mobility solutions for individuals with disabilities. As depicted in Figure 1, the completed prototype shows the adaptive equipment mounted to the steering column. The hand controls function as they do in a car that has adaptive controls installed; the accelerator and brake pedals move appropriately in either push-pull or push-right angle modes.
 |
|---|
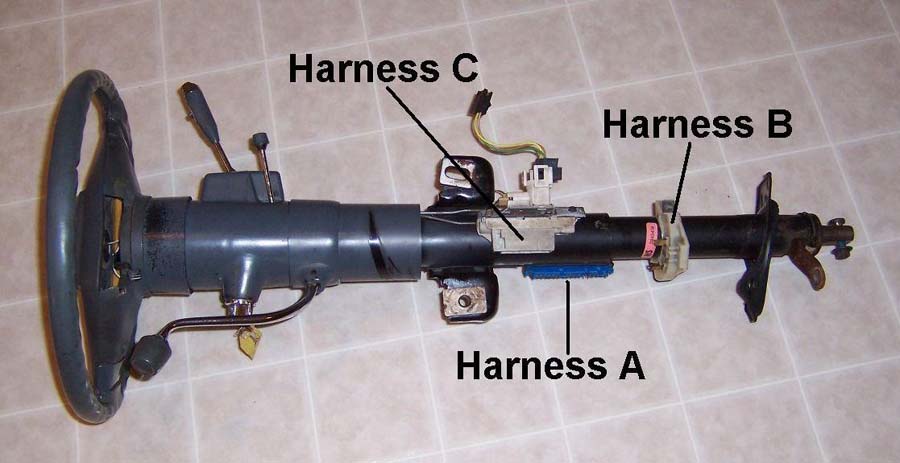
To interface with the simulation software (by Digital MediaWorks, Inc.) several physical parameters are measured. These include steering wheel angle, accelerator and brake depression, and the positions of the ignition switch, gear shifter, and turn signal stalk. Linear and rotary encoders are used for the continuous steering wheel (1 degree resolution) and foot pedal (500 counts per inch on depression) positions. The remaining parameters are captured from one of three wiring harnesses on the steering column (Figure 2) that make available various switch positions for the ignition switch, gear shift, and turn signal. High speed data acquisition provides real-time position and switch information to the virtual environment software up to once every millisecond, using a US Digital USB1 data acquisition interface.
OUTCOME/PERFORMANCE & COST
In conjunction with the virtual environment software, this hardware closes the feedback loop to provide a fully interactive environment for the participant. After depressing the brake pedal (using the hand controls), the participant turns the ignition to start the car and puts the car in gear. The software, which constantly monitors all the hardware parameters, “starts” the virtual car and places it in drive. When the participant accelerates, the virtual car accelerates and the virtual environment reacts to every action that the participant makes in a realistic manner.
The accessible driving hardware includes a real steering wheel and hand controls, and a flexible data acquisition interface to the virtual environment. The unit can be fitted under a table as shown here. The position of the steering wheel/hand control unit can be moved up and down, and tilted with respect to the table top to provide adjustability. The data acquisition interface is reconfigurable; additional analog and digital inputs can be easily plugged into the USB interface in order to capture additional physical or physiological parameters such as grip force and pedal force. Total cost (parts and labor) for the system shown here is under $2,500. Most importantly, the unit consists of an actual steering wheel and real adaptive driving equipment, which is only available currently in large expensive whole- or half-car simulators. This hardware interfaces to a PC-driving driving simulator making the entire system a more cost-effective acquisition for medical and clinical facilities.
IMPLICATIONS/FUTURE DIRECTIONS
The hardware described here allows the collection of important data for not only updating the virtual environment but for evaluating critical driving behaviors such as reaction time, appropriate use of hand controls, over-steering and attention. It will be validated and then used in future studies for driver evaluation and retraining. The current design allows a high degree of flexibility in placement of the steering wheel and hand controls with respect to the driver; it is likely that some of this flexibility is not needed and can be removed for simplicity. We intend to make manufacturing recommendations based on the results of this study to identify the critical hardware configurations that are needed in a final production system. Most importantly, the system allows collection in important driving data which can be used to evaluate driving behaviors in a cost-effective and realistic manner.
REFERENCES
- Peters, B. (2001). Driving performance and workload assessment of drivers with tetraplegia: an adaptation evaluation framework. J Rehabil Res Dev. 38(2): 215-24.
- Ku, J. H., Jang, D. P., et al. (2002). Development and validation of virtual driving simulator for the spinal injury patient. Cyberpsychol Behav 5(2): 151-6.
- Ahn, H. B., Ku, J. H., et al. (2001). The development of virtual reality driving simulator for rehabilitation. Proceedings of the 23rd annual International Conference of the IEEE Engineering in Medicine and Biology Society, Istanbul, Turkey.
- Beatson, C. and Gianutsos, R. (2000). Personal transportation: the vital link to independence, Chapter 43. Physical medicine and rehabilitation: The complete approach. M. Grabois, S. J. Garrison, K. A. Hart and L. D. Lehmkuhl, Blackwell Science, Inc: 777-802.
Author Contact Information:
Lisa K. Simone, Ph.D.
Kessler Medical Rehabilitation Research and Education Corporation
1199 Pleasant Valley Way
West Orange, NJ 07052
Phone (973) 324-3550
EMAIL: lsimone@kmrrec.org