Sharon Eve Sonenblum, MS; Stephen Sprigle, PhD, MPT; Leslie VanHeil, MSPT; Chris Maurer, MPT
ABSTRACT
People with spinal cord injuries (SCI) must transfer many times daily. Despite the importance of proper transfers, researchers have not completely described the kinematics of lateral transfers. In this study, 19 male adults with SCI who transfer independently or with minimal assistance were recruited to perform three lateral transfers to and from a therapy mat. On average, subjects elevated their sacroiliac joints (buttocks) 11 inches above the therapy mat and lowered the tempromandibular joint (head) to 21 inches above the mat. Subjects used a variety of strategies to complete the transfer that differed by their timing, the number of lifts performed, and their body positioning during transfers. Transfers from the wheelchair to the mat were more consistent within subjects.
KEYWORDS: transfer, biomechanics, wheelchair, SCI
BACKGROUND
Persons with spinal cord injuries (SCI) must learn to transfer to and from the wheelchair, bed, toilet, bathtub, car, and any other surface on which he or she wants to be. Given the high number of transfers made on any given day, acquiring the proper technique is paramount to shoulder joint integrity and personal independence. In fact, the ability to transfer has been correlated with independence in spinal cord injured persons (1). Subbarao et al reported that 72.7% of persons polled with SCI suffered from upper extremity (UE) pain (2). After a comprehensive literature review, Nyland et al identified transfer technique as a risk-factor for UE degeneration and cited the need for quantitative measures of transfers and additional transfer research (3). Currently, research on the kinematics of lateral transfers has been limited to the upper extremity.
The purpose of this pilot study was to collect kinematic data on lateral transfers and identify different transfer strategies. Additionally, this study aimed to identify quantitative measures which describe transfers.
METHODOLOGY
Subjects:
A convenience sample of 19 male adults was recruited from Shepherd Center (an acute SCI rehabilitation center) with IRB approval. Subjects had to be able to perform lateral transfers independently or with minimal assistance and could not have pressure sores or upper extremity orthopaedic conditions. The average age of our subjects was 32.1 years (Range: 18-61, Stdev: 11.7), weighed 176 pounds (Range 125-280, Std: 41) and were 71.9 inches tall (Range: 63-77 inches, Std: 3.7). The subject pool encompassed 14 Complete injuries (10 T-level, 3 C-level, and 1 T/C level, 3 incomplete T-levels, 1 incomplete C-level, and an incomplete post-polio subject. SCI levels ranged from C5 to T12. All of our subjects except one were more than 6 months post injury. Three subjects were excluded from analysis because they used sliding boards to perform transfers.
Instrumentation:
The motion capture system used was developed by Motion Reality Inc. (Marietta, GA). Eight 60Hz cameras were located around the perimeter of the ceiling. 37 permanent and four temporary markers were applied to the subject and 8 markers were applied to their wheelchair. Rather than direct application to the participant, the markers were attached to a vest, belt, gloves, hat, and booties. The proprietary motion capture software used a single capture frame of the subject in an approximate T-pose while seated in their own wheelchair, as well as height, weight, shoe size and body-type to create a model of the subject. After the model was created and temporary markers removed, each capture began in the modified T-pose. The body was tracked according to the model previously created.
Protocol:
After providing written consent, subjects donned markered apparel and researchers collected demographic, wheelchair and medical history information. We captured a single frame to create a model and then asked subjects to perform three lateral transfers to their stronger side between their own wheelchairs and a 20” high therapy mat. They were provided as much assistance as they generally used. . The second transfer was video taped.
Analysis:
A mid-transfer point was defined for each transfer such that time zero was set to be the point where the waist reached its maximum height between the final lift-off from the chair (or mat) and the initial contact with the mat (or chair). Many kinematic variables were calculated and analyzed but only a subset of these variables will be discussed here.
For each subject, two average values (transfer to the mat and transfer to the chair) were calculated for the following descriptors of transfers: buttock height, head height, wrist spacing and torso angle. The Motion Reality software reports the position of body segments based on markers located at relevant anatomical sites. Therefore, buttock height and head height only approximately represent the height above the therapy mat of the sacroiliac and tempromandibular joints respectively. Wrist spacing is measured as the distance between the left and right wrist body segments at the time of mid-transfer. Torso angle represents the angle of a line connecting the shoulders relative to a line connecting the hips. Paired t-tests were used to compare maximum buttock height, minimum head height, wrist spacing and torso angle during transfers to and from the wheelchair.
The portion of the transfer strategy described included the weight-bearing activity from initial lift-off from the starting surface to the final landing on the finish surface. The start and stop times of a transfer are difficult to identify as some subjects have a clear stopping point between preparation activities (such as moving their armrests or adjusting their legs) and the weight-bearing activities, yet others do all this in a continuous motion. In addition to time-based analysis, the data was configured with respect to the subject’s position along the horizontal path between the wheelchair and the mat. To compare strategies and variability, this data was normalized to the maximum waist height of each transfer. Variability was calculated using the average squared distance from the mean path for a subject or transfer direction.
RESULTS
Subjects elevated their buttocks an average of 11 inches above the therapy mat at mid-transfer (Table 1). They lowered their heads maximally to approximately 21 inches above the mat. Subjects did not display a significant difference in buttock and head heights when transferring to the mat versus transferring to the wheelchair. In 75% of transfers to the mat, the lowest head position was reached after mid-transfer. In the remaining 25%, the subjects lowered their heads prior to mid-transfer. On average, though, the two events (mid-transfer or maximum waist height and minimum head height) were only separated by 0.3±0.5 seconds. In 60% of transfers to the wheelchair, the minimum head position was reached after mid-transfer. The time separating mid-transfer and minimum head height for transfers to the wheelchair was only 0.1±0.6 seconds. While not statistically significant, (p=0.0973) the time separating the two events tended to be smaller in the transfer to the wheelchair.
| Transfer To Mat | Transfer To Wheelchair | |||
|---|---|---|---|---|
| Mean ± Stdev | Range | Mean ± Stdev | Range | |
| Max Buttock Height (above therapy mat) | 11.6” ± 1.6” |
8.4”-14.8” |
11.4”±2.0” |
7.7”-17.3” |
| Min Head Height (above therapy mat) | 21.2”±3.4” |
13.9”-28.0” |
21.8”±2.7” |
35.1”-47.5” |
| Wrist Spacing at Mid-Transfer | 25.5”±3.9” |
18.3”±35.5” |
26.2”±4.1” |
19.0”±36.9” |
| Shoulder – Hip Twist Angle | 23º ± 8º |
6º - 38º |
24º ± 8º |
8º - 47º |
 |
|---|
 |
 |
Subjects’ wrists were separated slightly farther apart at mid-transfer in transfers from the chair (25.5”) than in transfers to the chair (21.8”). The amount of torso rotation varied greatly between the subjects. The average angle formed by the shoulders and hips were nearly identical in transfers to and from the wheelchair (24 ° & 23 °).
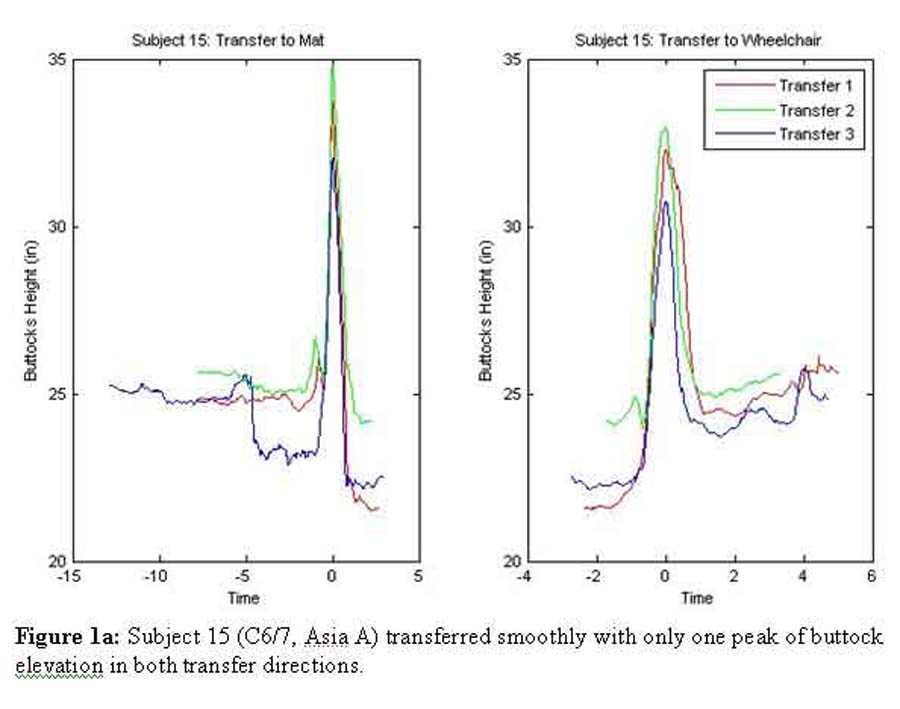
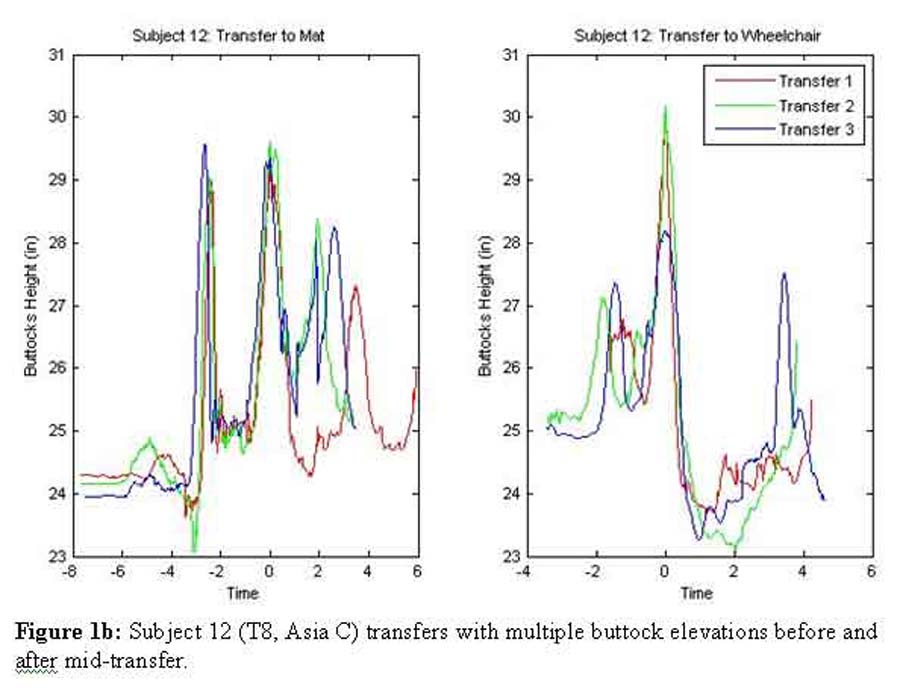
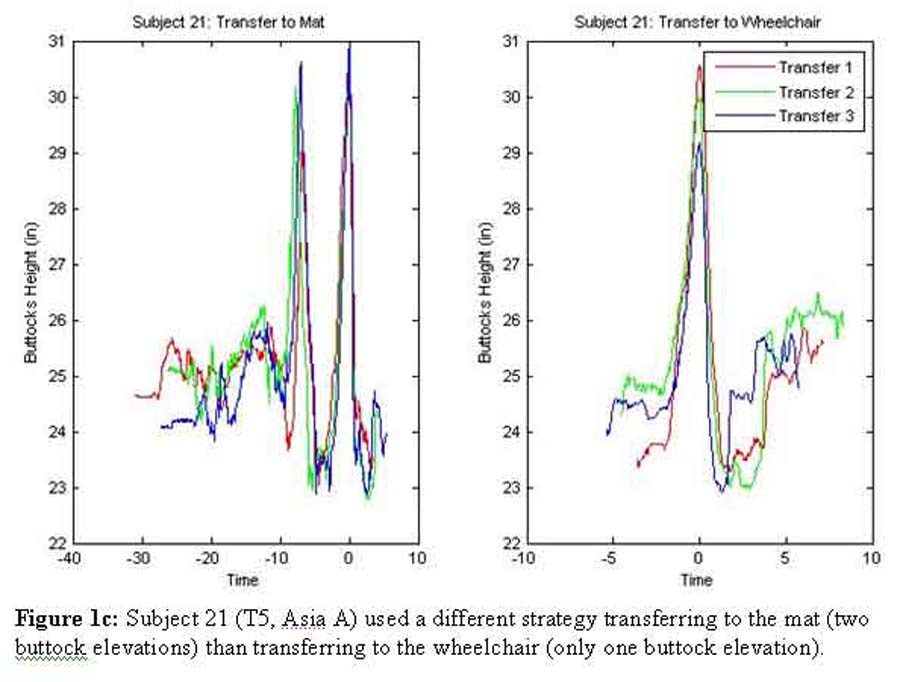
Figure 1 a-c demonstrates the time sequence of three subjects’ transfers. Figure 1a (Subject 15: C6/7, Asia A) shows a smooth transfer with only one peak of buttock elevation in both transfer directions. In contrast, Figure 1b (Subject 12: T8, Asia C) shows transfers that utilized multiple buttock elevations before and after mid-transfer in order to complete the transfer task. Figure 1c (Subject 21: T5, Asia A) highlights a subject who appears to have used a different strategy transferring to the mat (two buttock elevations) than transferring to the wheelchair (only one buttock elevation). These three subjects reached different buttock heights on each transfer, with Subjects 12 and 21’s transfers to the mat being most consistent (Table 2).
Standard Deviation of Maximum Buttock Heights |
Variation between normalized transfers | |||
|---|---|---|---|---|
| Subject # | Transfer to Mat | Transfer to Chair | Transfer to Mat | Transfer to Chair |
| 15 | 1.4 | 1.1 | .03 | .02 |
| 12 | 0.2 | 1.1 | 0.10 | 0.10 |
| 21 | 0.1 | 0.7 | 0.08 | 0.03 |
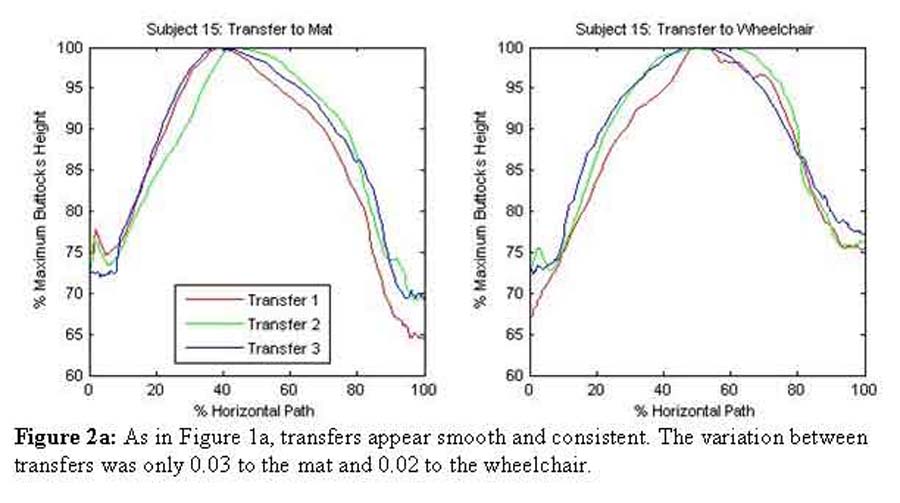
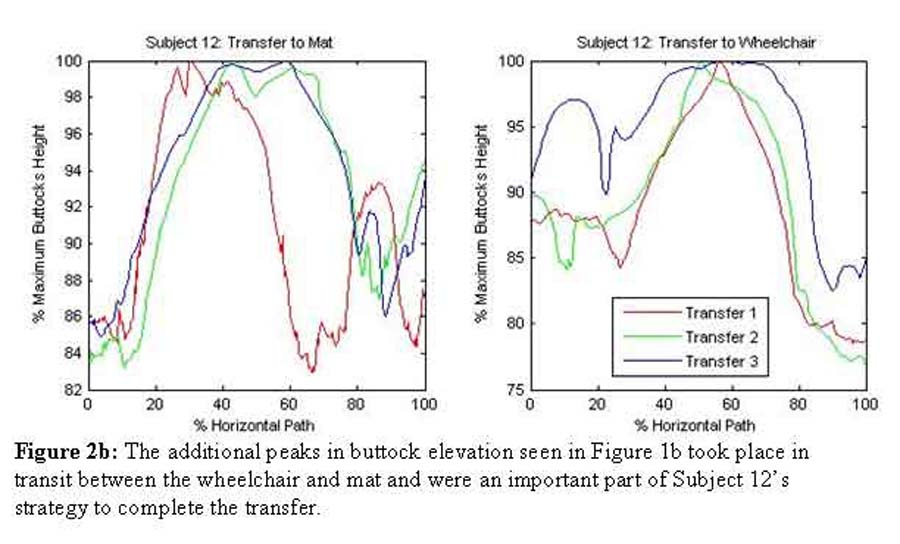
The normalized plots of buttock height over the horizontal path of the buttocks (Figure 2 a-b) provide different information about transfer strategy. For Subject 15, this graph (2a) was similar to his time-based graph and also illustrates a series of smooth and consistent transfers. The variation between transfers was only 0.03 to the mat and 0.02 to the wheelchair. A small difference in strategy between the two transfer surfaces is evident in these graphs. There is a steeper slope in the transfer to the mat which suggests that the subject elevated his buttock mostly over the wheelchair (approx. 40%) and traveled the distance to the mat mostly during the descent (approx 60%). In contrast, the transfer to the wheelchair was symmetrically split between ascent and descent. Figure 2b illustrates that the additional peaks of buttock elevation visible in the time graphs took place in transit between the wheelchair and mat and were an important part of Subject 12’s strategy to complete the transfer. This subject’s transfers were far more variable (0.10 to and from the mat). In both Figures 2 a & b, the maximum buttock height occurred relatively later in the path when transferring to the wheelchair.
 |
|---|
 |
Over all the subjects, the variation between transfers ranged from 0.01 to 0.28 with an average of 0.05±0.04 for transfers to the mat and an average of 0.07±0.06 for transfers to the wheelchair. On average, transfers to the wheelchair had greater variations than transfers to the mat ( p=0.0335).
DISCUSSION
Persons with SCI use a variety of strategies to transfer between two surfaces. The number of times subjects elevated their buttocks varied greatly, while the maximum buttock height was relatively consistent between transfers and subjects (SD 1.6” and 2.0”). While the buttock height does not directly correspond to clearance, it might be inferred that the cause of the consistent buttock heights is that subjects elevate the minimum amount necessary to clear the wheelchair wheel (which is also relatively constant).
The different transfer strategies might be correlated to such factors as injury level, time since injury or body weight. Future work will cluster the transfer strategies in order to determine these relationships. Additionally, it is possible that the repeatability of the transfers might be related to UE pain or safety of transfers. Further work with a greater number of subjects is needed to figure this out.
REFERENCES
- Pentland WE and Twomey LT. (1994). Upper limb function in persons with long term paraplegia and implications for independence: Parts I & II. Paraplegia 32: 211-218.
- Subbarao JV, Klopfstein J, and Turpin R. (1995). Prevalence and impact of wrist and shoulder pain in patients with spinal cord injury. J Spinal Cord Med 18: 9-13.
- Nyland J, Quigley P, Huang C, Lloyd J, Harrow J, and Nelson A. (2000). Preserving transfer independence among individuals with spinal cord injury. Spinal Cord 38: 649-657.
ACKNOWLEDGEMENTS
Funding was provided by NIDRR through the RERC for Wheeled Mobility (H133E030035)
AUTHOR CONTACT INFORMATION
Sharon Eve Sonenblum, MS
CATEA; 490 10 th Street
Atlanta, GA 30318
Phone: (404) 385-0633
Email: Sharon@catea.org