Jongbae Kim, BA and David M. Brienza, PhD
ABSTRACT
A Virtual Reality Telerehabilitation System that enables clinicians to assess the wheelchair accessibility of users’ built environments from a remote location is under development. This system uses commercial software to construct 3D virtualized environments from photographs. Custom screening algorithms and instruments for analyzing accessibility were developed. The characteristics of the camera and the 3D modeling program have significant effects on the overall reliability of the system. We previously performed two reliability analyses on the hardware and software components: The first verified that the commercial software, Photomodeler Pro, can construct sufficient 3D models by analyzing the accuracy of the dimensional measurements in the virtualized environment (1). The second compared the dimensional measurements obtained from models created with photographs from four different camera types. Based on these two analyses, we were able to specify a consumer level digital camera and the Photomodeler Pro software for this system. (2) In this study, we tested the system in the home of a typical wheelchair user to evaluate its ability to assess its accessibility. The field test resulted in an accurate accessibility assessment thus validating our system.
Key Words: 3D Model, Accessibility, Home Modification, Telerehabilitaion, Virtual Reality.
BACKGROUND
 |
The number of wheelchair users of age 15 years and over is estimated at more than 2.2 million in the U.S. (3) For any given limitation in function, the amount of disability that an individual experiences will depend on the quality of the social and physical environment. Consideration of the built environment is especially critical for wheelchair users given the potential limitation that it can impose. The most effective rehabilitation outcomes are realized when programs consider both functional restoration and environmental modification (4). The 1995 American Housing Survey (AHS) asked whether members of households had permanent physical activity limitations and, if so, whether home modifications were performed. Based on the survey, approximately 5.1 million (57.4 percent) of the households in which a member had an activity limitation had no home modifications (5).
 |
Effective home modification requires consultation with skilled professionals who are able to assess the home environment and identify what changes are necessary to meet the wheelchair user’s needs. While there are many building and remodeling contractors able to perform the modifications, the availability of skilled professionals with experience in home modifications for accessibility is limited (6). Providing services in rural areas is particularly difficult. Such service requires long travel times that increase the costs and consume the scarce time of skilled professionals. A system that allows accurate remote assessments to be performed would be an important tool to improve our ability to perform home assessments more easily and at a decreased cost.
 |
Some developmental work has been done using a remote assessment system in rural or under-served areas. A team of clinicians at the Shepherd Center (Atlanta, Georgia) performed a case study of remote home modification evaluation using a videoconference system with a video telephone (7, 8). Another effort was undertaken by Extended Home Living Services in Wheeling, Illinois which developed a remote assessment protocol using a survey instrument, the Comprehensive Assessment Survey Process for Aging Residents (CASPAR TM). The CASPAR instrument can be mailed to residents in remote areas to obtain information about consumer priorities, activities of daily living, ability to participate in home-specific occupations, and the space, layout, and design of the residence so that home modifications can be recommended (9, 10). Both of these studies are limited in that the dimensions obtained are not sufficient for use in specifying modifications. Both methods depend on dimensions obtained using a tape measure by the client. The use of virtual reality technology and telerehabilitation concepts to assess the home built environments of persons with severe mobility impairments was recently proposed by University of Pittsburgh researchers (11) The Virtual Reality Telerehabilitation System (VRTS) described here is under development as part of the proposed project.
 |
Our VRTS is designed to evaluate the accessibility of physical environments of wheelchair users. The VRTS takes advantage of state-of-the-art digital imaging, 3D modeling, and photogrammetry technologies. Accuracy is a critical concern in the virtualized environment (12) and usability is a primary concern for the telerehabilitation system (13). Accuracy and usability are important for developing a successful system.
To verify that Photomodeler Pro can produce a sufficiently accurate 3D model of the physical environment of wheelchair user’s built environment, we analyzed the accuracy of the dimensional measurements in the virtualized environment of a wheelchair user’s office space. This trial showed an average precision value of 200:1 (0.51%). This precision would result in a measurement error of 4 mm (0.16″) for a typical 800 mm (32″) door opening. Photomodeler Pro was determined to be able to produce sufficiently accurate 3D models to make an assessment of the accessibility of a wheelchair user’s home (1). Usability was a primary consideration for the VRTS design. We compared the modeling accuracies for four different cameras/camera settings including a disposable camera and three digital camera variations. By the comparison of camera systems, we concluded that disposable film camera and consumer grade digital camera can be used in the VRTS (2).
Research Question: Can the VRTS adequately model and evaluate the wheelchair accessibility of a typical users' home built environment?
METHODOLOGY
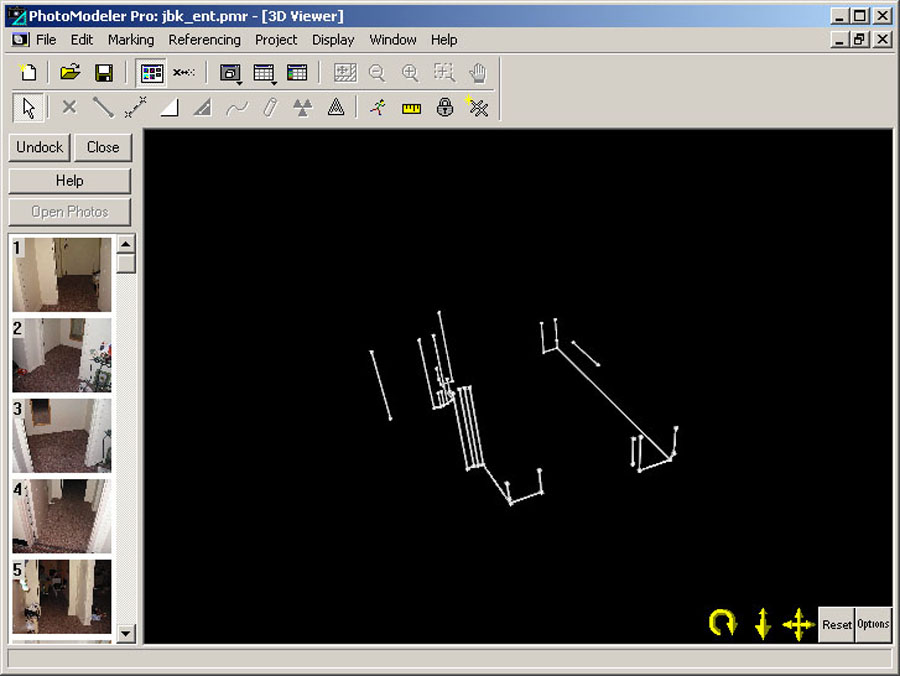
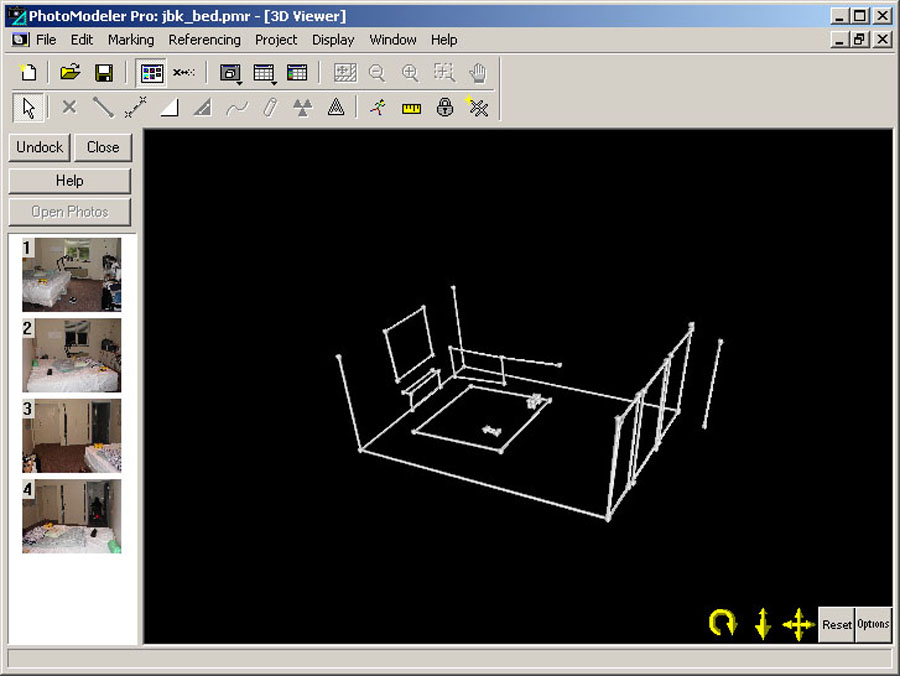
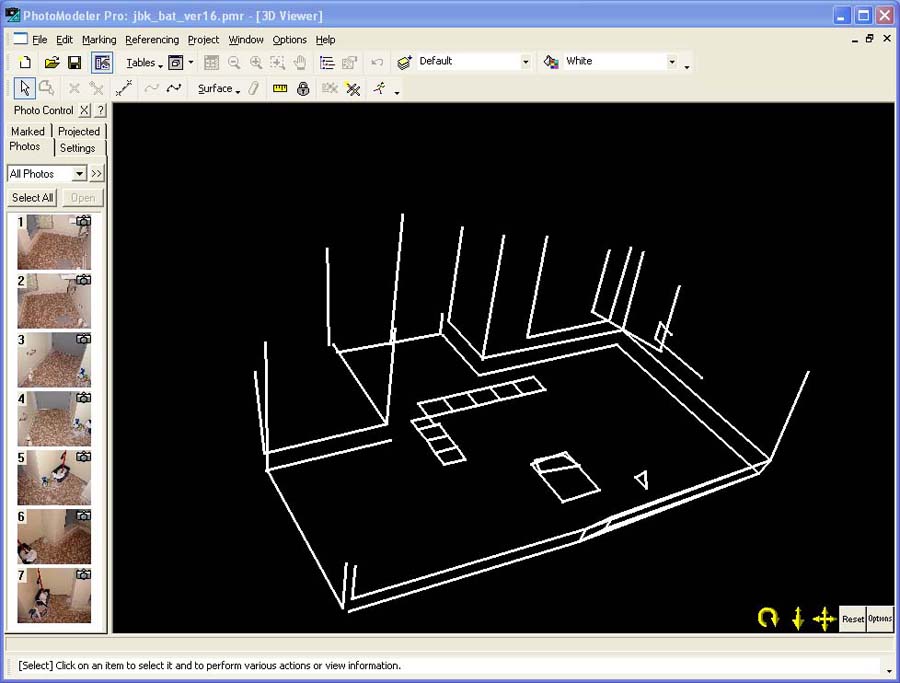
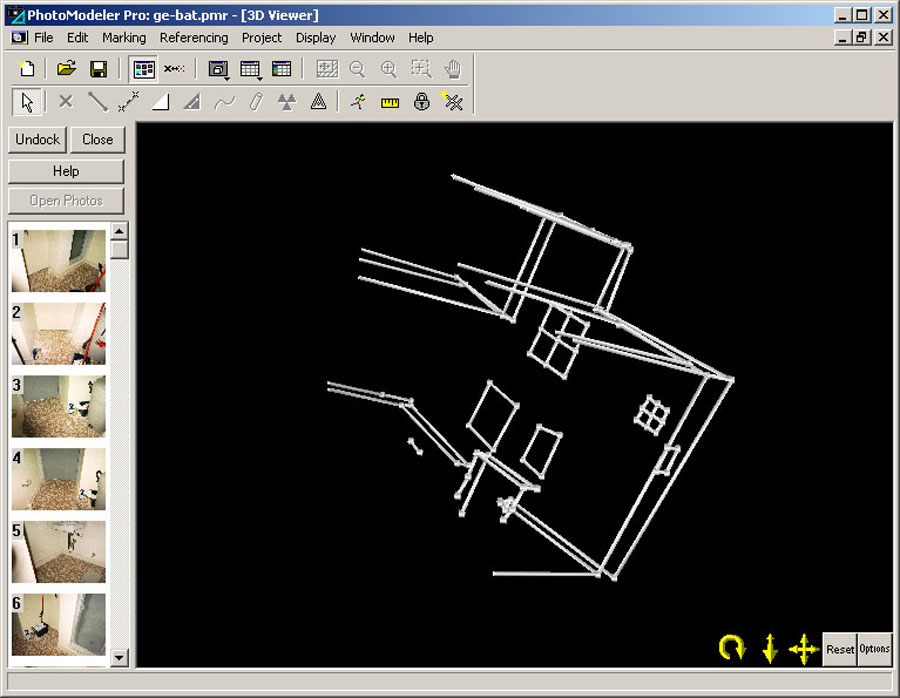
A feasibility test was conducted using the Canon Powershot A10 digital camera with 1.2 mega pixel resolution. The target environment was a client’s apartment unit where one of the occupants uses a standard powered wheelchair. One wheelchair user’s friends was instructed on how to take the pictures. He took about 60 pictures, 15 pictures each per four subparts of the apartment: entrance hall way, bedroom, living room, and bathroom. After the camera was calibrated, a 3D model for each of four architectural subparts was made using Photomodeler Pro 4.0 so that the dimension of physical environment could be easily measured in the virtualized environment. These four 3D models can be seen in the figures below (Figure 1 - 4). These 3D models were used to identify the problematic parts for the wheelchair accessibility of the client’s home.
RESULTS
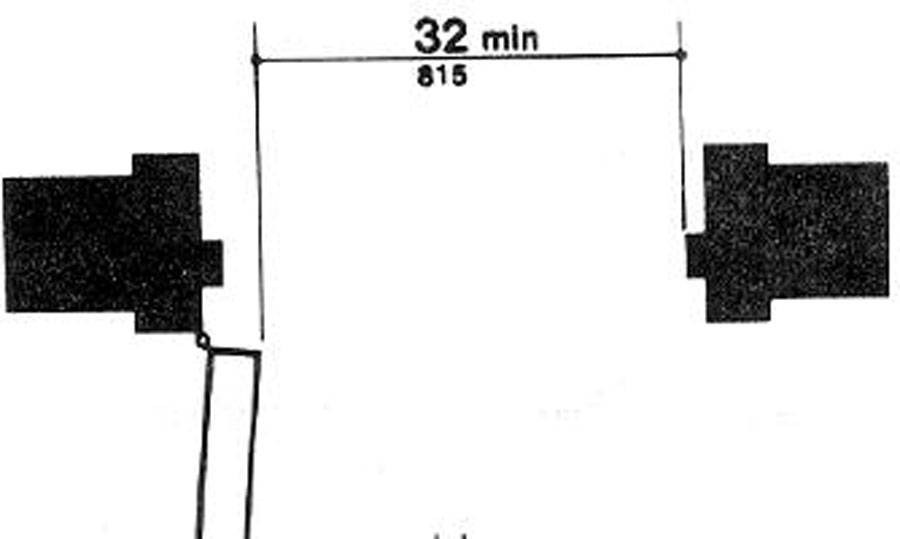 |
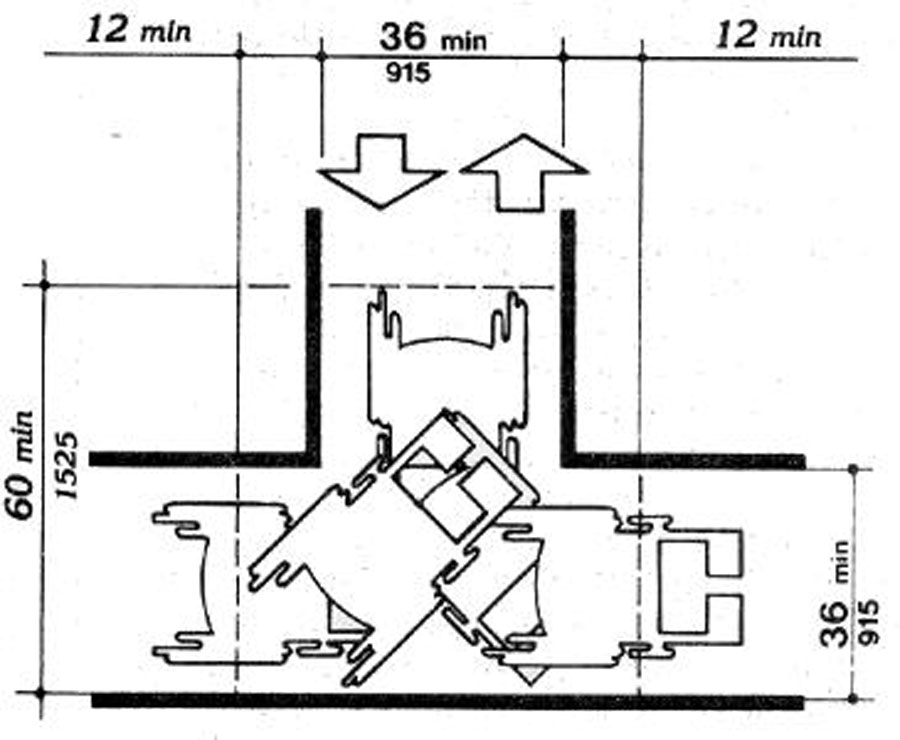
Using the 3D models constructed from 2D photos obtained by the Canon A10 digital camera and the Photomodeler Pro, the investigator discovered that the kitchen’s door should be widened and the curb of the shower booth must be removed. But the width of the bathroom’s door and the height of the sink was enough to accommodate the use’s wheelchair. The doorway of the entrance was too narrow compared to the ADA Accessibility Guideline (ADAAG) (Figure 5, 6). No accessibility problems were found in the living room or bedroom.
DISCUSSION
 |
|---|
Accessibility assessment via the virtualized environment was similar to the in-person assessment of an experienced rehabilitation engineer. That is, an engineer obtained similar measurements and came to the same conclusions. This study will be followed by the development of enhanced algorithms and several new instruments: a guide book on how to take pictures, a survey form, a measurement form, and an evaluation form. A second field evaluation with more data will be designed and performed to assess the value of the VRTS compared to the conventional in person method.
CONCLUSION
The field feasibility test of the hardware and software instruments adapted through first and second analyses showed these instruments were appropriate. If we are successful in developing a Virtual Reality Telerehabilitation System for analyzing accessibility of the built environment, the system could improve rehabilitation outcomes by making accessibility assessments and modifications available to a larger potion of the population of wheelchair users.
REFERENCES
- Kim J. Brienza DM. Development of a Virtual Reality Telerehabilitation System for Analyzing Accessibility of the Built Environment , submitted to the JRRD
- Kim J. Brienza DM. The Virtual Reality Telerehabilitation System for Analyzing Accessibility of the Physical Environment: A Comparison of Camera Systems ; Proceeding of RESNA 26 th International Conference, June 2003
- McNeil, JM. Americans With Disabilities : 1997 U.S. Department of Commerce, Economics and Statistics Administration, Bureau of the Census. 2001
- Brandt E., Jr. and Pope A. (eds.), Enabling America, National Academy Press, 1997.
- U.S. Department of Housing and Urban Development and U.S. Census Bureau, American Housing Survey for the United States, Supplement: 1995, Current Housing Reports, Series H151/95, U.S. Government Printing Office, Washington, D.C., forthcoming.
- Extended Home Living Services ., Comprehensive Assessment and Solution Process for Aging Residents ( http://www.ehls.com/caspar/caspar.html ) 2002
- Burns RB , Crislip D , Daviou P , Temkin A , Vesmarovich S , Anshutz J , Furbish C , Jones ML. Using telerehabilitation to support assistive technology. Assistive Technology. 10(2):126-33, 1998.
- Sanford JA , Jones M , Daviou P, Grogg K, Butterfield T . Using Telerehabilitation to Identify Home Modification Needs, Assistive Technology. 16(1), 2004.
- Pynoos J, Sanford J, Rosenfelt T . A Team Approach for Home Modification AOT Practice, 15-19, April 8, 2002.
- Sanford JA, Pynoos J, Tejral A, Brown A. (2002) Development of comprehensive assessment for delivery of home modifications Physical and Occupational Therapy in Geriatrics 20(2), 43-55
- Cooper RA , Fitzgerald SG , Boninger ML, Brienza DM, Shapcott N, Cooper R, and Flood K. Telerehabilitation: Expanding Access to Rehabilitation Expertise, Proceedings Of The IEEE, VOL. 89, NO. 8, AUGUST 2001
- Durlach NI, Mavor AM , Virtual Reality: Scientific and Technological Challenges, Computer Science and Telecommunications Board, (1994), Ch8 : 247-303
- Lathan CE, Kinsella A, Rosen MJ, Winters J, Trepagnier C. Aspects of human factors engineering in home telemedicine and telerehabilitation systems. Telemed J. 1999;5:169–175.
Acknowledgements:
This work was funded by the Department of Veterans Affairs and the University of Pittsburgh. Opinions expressed are those of the authors and do not necessarily reflect those of the funding agencies.
Jongbae Kim
University of Pittsburgh
Department of Rehabilitation Science and Technology
5044 Forbes Tower
Pittsburgh, PA 15260
412-383-6581
jbkim @pitt.edu