Kelly M. Baker, MS1, Lucy Lu 4, Kathy Reiners3, Sahar Hassani, MS3, Jeffrey D. Ackman, MD3, Jeffrey P. Schwab, MD2 , Gerald F. Harris, PhD, PE1,2,3
1Orthopaedic and Rehabilitation Engineering Center (OREC), Milwaukee, WI
2Department of Orthopaedic Surgery, Medical College of Wisconsin, Milwaukee, WI
3Motion Analysis Laboratory, Shriners Hospital for Children, Chicago, IL
4Department of Biostatistics, Medical College of Wisconsin, Milwaukee, WI
ABSTRACT
Anterior walkers are a rehabilitative aid prescribed to children with cerebral palsy. These assistive devices are placed in front of the patient and repeatedly advanced during the gait cycle. Analysis of the kinematics of patients using anterior walkers may lead to improved rehabilitation. The purpose of this study is to characterize upper extremity (UE) motion in 20 children with spastic diplegic cerebral palsy (CP) who use anterior walkers for ambulation. Results indicate that such patients exhibit an increased heart rate and decreased walking speed with anterior walker usage. The Gross Motor Function Measure results correspond to those reported by other researchers. The unique morphology of the shoulder, elbow, and wrist joint kinematics is described.
KEYWORDS
Cerebral palsy; kinematics; rehabilitation; upper extremity; walker
BACKGROUND
Cerebral palsy (CP) is a movement disorder produced by an insult to the brain (1). It has symptoms including postural instability, muscle weakness, and spasticity. The Centers for Disease Control and Prevention (CDC) estimate that 2.8 per 1,000 children in the United States develop CP each year (2). The lower extremities are frequently affected, with walkers commonly prescribed to help overcome ambulatory difficulties. The walker allows the upper extremities to become more involved in the movement process. Currently, it is difficult to prescribe a walker for a patient with cerebral palsy because each patient’s condition is variable and it is not known or understood how a walker affects a patient biomechanically. Analysis of the kinematics of patients using anterior walkers may lead to improved rehabilitation efforts.
As a precursor to this study, our group developed an upper extremity (UE) motion analysis system (3). This study, utilizing that system, reports quantitative measures of UE kinematics in 20 children with CP who use anterior walkers for ambulation. By eventually comparing these results to our previous analysis of posterior walker results, we hope to develop a more universal method for prescribing walkers to children with CP (4).
RESEARCH QUESTION
To date, there is no quantitative characterization of UE kinematics in subjects using anterior walkers. This study reports quantitative measures of UE kinematics in 20 children with cerebral palsy, who routinely utilize an anterior walker for ambulation.
METHODOLOGY
The study takes place at two institutions (Shriners Hospital for Children, Chicago, and the Medical College of Wisconsin, Milwaukee). Testing included use of a Vicon motion analysis system and an internally developed UE kinematic model (3).
Patient visits included an initial screening visit and a testing visit. The visits have a one month separation period to allow patients to become acclimated to the anterior walker if they do not already use one. Following informed consent patients undergo gait analysis and physical examination, which involves a heart rate monitor test, and Gross Motor Function Measure (GMFM). An acceptable gait cycle is defined by foot strike to ipsilateral foot strike (5) with no marker dropout.
Twenty patients (aged: 12.6 ± 3.1 years) have been tested. To characterize motion, the method of fitting a Fourier series to the kinematic data was used (6). By use of the least squares method, we fit our data to the linear model:

where ![]() Yij = the data for the ith % of a cycle and the jth trial, f = max no. of terms for the model set by R
Yij = the data for the ith % of a cycle and the jth trial, f = max no. of terms for the model set by R 2 analysis, a
2 analysis, a![]() O, a
O, a![]() l , b
l , b![]() l= constants, and error has a mean of zero.
l= constants, and error has a mean of zero.
From this model, predicted values at each percentage of the gait cycle were determined for each patient.
RESULTS
Physical Examination
Heart Rate Monitor: Heart rate monitor results indicate that the average resting heart rate is 92.7 beats/min and the average walking heart rate is 137.7 beats/min. The average walking speed is 19.1 meters/min, with an average energy expenditure index value 4.2 beats/meter.
| Units | Mean | Std. Dev. | |
|---|---|---|---|
| Resting Heart Rate | beats/min | 92.7 | 10.7 |
| Walking Heart Rate | beats/min | 137.7 | 18.0 |
| Walking Speed* | m/min | 19.1 | 11.7 |
| Energy Expenditure Index* | beats/m | 4.2 | 4.3 |
GMFM: The GMFM results indicate that the average Standing Assessment Score is 75.5 ± 21.3% and the average Walking, Running, and Jumping Assessment Score is 51.2 ± 15.8%.
| Mean | Std. Dev. | |
|---|---|---|
| Standing Assessment (D) (%) | 75.5 | 21.3 |
| Walking, Runnin, Jumping Assessment (E) (%) | 51.2 | 15.8 |
Gait Analysis
Shoulder : Joint kinematic and statistical model results indicate that during walker usage, both the right and left shoulders are in extension. The shoulder angle averages between 20.5-24.5º on the right side with a 95% confidence interval (CI) ranging between 9.1-35.2º. On the left side, the shoulder angle is between 17.7-23.0º with a 95% CI ranging between 7.5-32.5º.
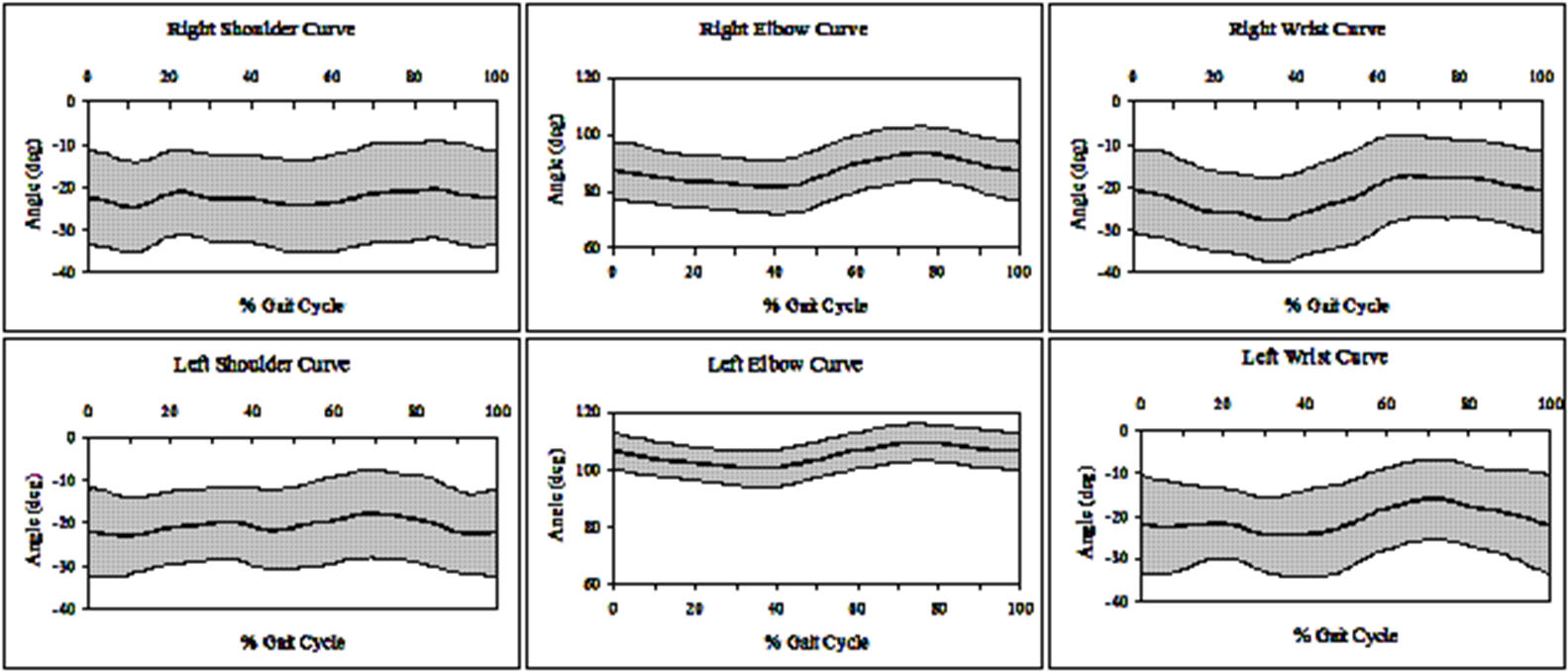 |
Elbow :Both the right and left elbows for an anterior walker user are in flexion.The right elbow angle averages between 81.5-93.2º with a 95% CI ranging between 71.9-102.4º.The left elbow angle averages between 100.6-109.6º with a 95% CI ranging between 94.3-116.0º.
Wrist :Right and left wrists are in extension. The wrist angle averages between 17.3-27.6º on the right side with a 95% CI ranging between 7.4-37.7º. On the left side, the wrist angle averages between 16.1-24.5º with a 95% CI ranging between 6.9-34.1º. The sagittal plane data (mean ± 95%CI) is shown in Fig. 1.
DISCUSSION
Physical Examination
The American Heart Association cites normal resting heart rate for an average 12 year old as 60-80 beats/min and the target heart rate (while exercising) between 104 and 156 beats/min (7,8). The normal walking speed for a child between 7 and 13 years old is 68.4 m/min (8). Our patients have a higher resting heart rate and a much lower walking speed. The GMFM showed results that were similar to those found by other researchers (9,10). Our D score finding was higher than that reported by Damiano and Abel (65.5±28.2%) and McCarthy et al (50.5±40.1), but it was still within their standard deviations. Our E score result was very close to Damiano and Abel (52.5±33.6%) and within a standard deviation of McCarthy et al (44.5±37.1%) (9,10).
Gait Analysis
Shoulder motion exhibits six peaks (P 1-P 6) during each gait cycle (GC). Greatest extension is seen at 11, 33, and 52% of the GC during loading/mid stance, terminal stance, and pre-swing on the right side, and at 11, 48, and 96% of the GC during loading/mid stance, terminal stance, and terminal swing on the left side. Least extension is seen at 23, 38, and 85% of the GC during mid stance, terminal stance, and mid swing on the right side, and at 0, 36, and 71% of the GC during initial contact, terminal stance, and initial swing on the left side. Elbow and wrist motion exhibits two peaks (P 1, P 2). Patients have greatest elbow flexion at 77% of the GC during mid swing on both right and left sides and least elbow flexion at 39 and 38% of the GC during terminal stance on the right and left sides, respectively. Patients have the greatest wrist extension at 34 and 36% of the GC during terminal stance on the right and left sides, respectively, and the least wrist extension at 70 and 74% during initial swing on the right and left sides, respectively.
REFERENCES
- Albright, L., et al. (2004). Spasticity Reduction in The Treatment of Gait Problems in Cerebral Palsy, J.R. Gage, Editor. Mac Keith Press: London.
- http://www.cdc.gov/ncbddd/dd/ddsurv.htm#cp, 12/04.
- Baker, K. M., et al. (2003, June). Rehabilitation Analysis of Walker Assisted Gait in Spastic Diplegic Cerebral Palsy Children. Proc RESNA, 26.
- Baker, K.M., et al. (2004, June). Upper Extremity Rehabilitation Analysis of children with Cerebral Palsy Using Posterior Walkers. Proc RESNA, 27.
- Perry, J. (1992). Gait Analysis: Normal and Pathological Function. Slack Inc. New York: NY. pp. 11-16.
- Klein, J.P. (1997). Statistical Issues in Randomized Trials in Motion Analysis. Proc of IEEE Eng Med Biol Soc, 19.
- http://www.americanheart.org, 1/04.
- Rose, J., & Gamble, J. (1994). Human Walking. Williams and Wilkens. Baltimore: MD.
- Damiano, D.L., & Abel, M.F. (1996) Relation of gait analysis to gross motor function in cerebral palsy. Dev Med Child Neurol 38(5): 389-396.
- McCarthy, M.L., et al. (2002). Comparing reliability and validity of pediatric instruments for measuring health and well-being of children with spastic cerebral palsy. Dev Med Child Neurol 44(7):468-476.
ACKNOWLEDGMENTS
This project is supported by NIDRR grant H133G010069.
Author Contact Information:
Kelly M. Baker
Academic Support Facility
105 OREC, P.O. Box 1881
Milwaukee, WI 53201-1881
Office Phone (414) 805-7456
EMAIL: kelly.baker@mu.edu