Elizabeth Leister, BS, Dan Ding, PhD, Rosemarie Cooper, MPT, ATP, Annmarie Kelleher, OTR/L, ATP, Rory A. Cooper, PhD, Shirley Fitzgerald, PhD, Michael L. Boninger, MD
Human Engineering Research Laboratories, University of Pittsburgh and VA Pittsburgh Healthcare System, Pittsburgh, PA 15206
ABSTRACT
To help manage pressure ulcers and adjust posture, powered wheelchairs can be equipped with tilt-in-space and/or recline features. Currently clinicians prescribe these features for wheelchair users who are vulnerable to pressure sores or difficulty changing posture, but little data has been collected to determine whether or not, and to what extent, these functions are used. In this study, a datalogger and six sensors including three tilt and three pressure sensors were attached to an individual’s power wheelchair for 10 days to gather quantitative data regarding the daily use of tilt-in-space and recline features. The results show that the participant chose small seat tilt and back recline angles for around 80 percent of the time, and the seating positions known to cause a 10% or 20% pressure decrease were accessed.
KEYWORDS
Pressure relief, pressure ulcer prevention, recline, tilt-in-space, wheelchair seating.
BACKGROUND
Pressure ulcers are a common and costly problem for wheelchair users in the United States. It is estimated that more than 1.35 billion dollars are spent each year on pressure sore care [1]. Back pain and poor posture are also common problems for wheelchair users; a recent study found that over 50% of wheelchair users experience back pain and that a majority of these individuals reported pain severe enough to visit a physician and limit their activities. For both of these conditions it is thought that tilt-in-space and recline wheelchair features may be of benefit. Tilt-in-space can significantly reduce static seating pressure, a key factor in the development of pressure sores [2]. In addition, using tilt-in-space and recline can allow for a change in position in the wheelchair and thus improve comfort. Based on these arguments, clinicians usually prescribe tilt-in-space and recline accessories for powered wheelchair users who have difficulty adjusting their posture, or for whom pressure ulcers are a recurring problem. Despite the fact that these features are so widely prescribed, there is very little research in this important area. Currently it is unclear if, once prescribed, these systems are effectively used, and if the most commonly used angles of the tilt-in-space and recline functions provide adequate pressure relief.
Dataloggers are portable, battery powered devices that can be used for data collection. This silent device travels with the subject in their daily activity settings and collects data independently. We have successfully developed a weather-proof datalogger that unobtrusively attaches to manual or electric powered wheelchairs and records distanced traveled by subjects while in wheelchairs [3, 4]. By using the datalogger, which does not interfere with the subjects’ daily routine, the feeling of “being a research participant” is minimized and the individual can go about their day as usual. Furthermore, in utilizing such a device, individuals who use powered wheelchairs can quantify their use of these features. The datalogger records can generate information such as: the amount of time spent using tilt-in-space and recline functions, and how often these functions are used; and the most common tilt-in-space and recline angles used during the course of the day. Clinicians can utilize the information to quantify the use of tilt-in-space and recline features and examine the effectiveness of using these features.
RESEARCH QUESTION
The purpose of this study is to determine the potential effectiveness of tilt-in-space and/or recline for pressure relief. Data collected over a 10 to 14 day period will provide information including:
- How often wheelchair users access tilt-in-space and/or recline functions per hour or per day;
- The most common tilt and/or recline angles, and the percentage of time spent in these angles;
The collected data will help determine how often and for how long wheelchair users with tilt-in-space and/or recline achieve a position known to cause at least a 10% and 20% decrease in peak pressure in an hour.
It is hypothesized that users will spend more time in a tilted position than in an upright position during the day. In addition, users with tilt-in-space and recline will use tilt-in-space significantly more than recline.
METHOD
Equipment:
Data were collected from six sensors attached to the subject’s wheelchair. Three single-axis analog tilt sensors (Crossbow Technology) measured the angle of the base, the angle of the seat, and the angle of the back. Tilt angles were measured as the angle between the seat and the base of the chair. Recline angles are measured as the angle between the seat and the back of the chair. Three pressure sensors (Interlink Electronics) measured the seat, upper back, and lower back pressures. A TFX-11 Tattletale datalogger (Onset Computer Corp.) collected data from these sensors, and stored the data in its memory. Usage of tilt-in-space and recline features was generated using a custom-written Matlab program.
Subject Testing:
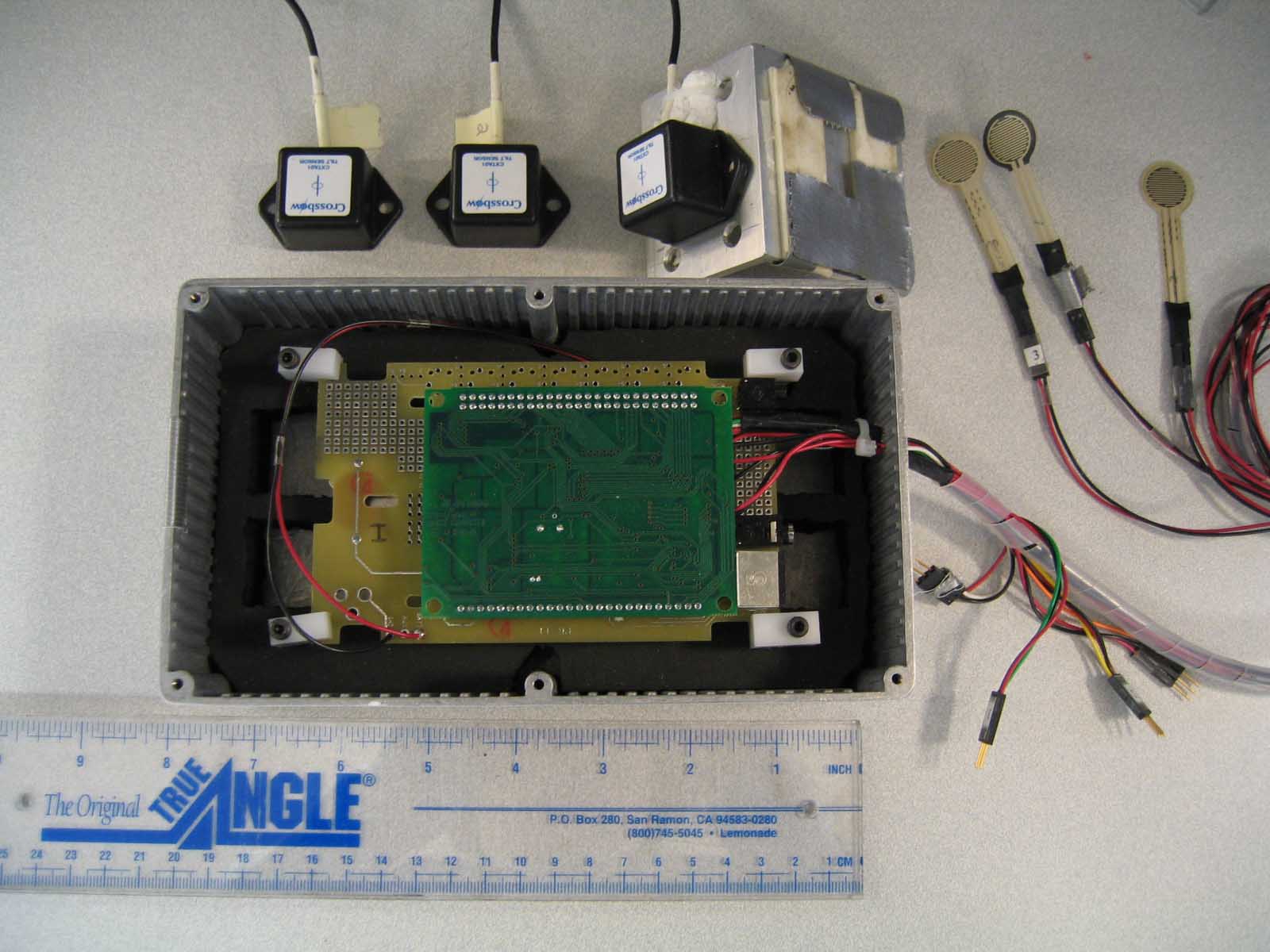 |
Subject testing was conducted at the Human Engineering Research Laboratories, at the Highland Drive VA Pittsburgh Healthcare System. During the first visit, informed consent was obtained, and the datalogger and sensors were attached to the subjects’ wheelchair (see Photo 1). Pressure reading calibration was performed at different seat and back angles using a pressure-mapping device. The subject was first transferred out of his/her chair and the pressure-mapping device was placed on top of cushion. After the subject was transferred back into the chair, pressure-mapping data, with tilt fully upright, was collected for every 5 degrees of recline. The chair was then tilted 5 degrees, and the calibration was repeated through the full range of tilt and recline angles. The participant was then sent home and asked to go about their normal activities for 10 to 14 days. Halfway through the trial data were downloaded and the batteries of the datalogger were replaced. At the end of the study the participant returned to the testing facility and had the datalogger and sensors removed. A questionnaire related to their use of tilt-in-space and recline was completed.
RESULTS
Results for one participant have been obtained at the date of this report, and are shown in Table 1. Time spent in the chair was determined from the pressure sensor underneath the seat cushion. The participant used the wheelchair for an average of 9.4 hours ± 2 hours each day for a total of 10 days. The participant accessed seat tilt fewer times per hour, but for longer periods of time, than back recline. In addition, the participant chose smaller seat tilt angles (≤ 10º) and back recline angles (≤ 95º). From Table 1 it can be inferred that tilt angles greater than 10º were used only 22% of the time and recline angles greater than 95º were used only 12% of the time.
| Average Results | Ranges | |
|---|---|---|
Tilt Access per Hour |
6.5 | 2 – 11 |
Average Time Tilt was Accessed (min) |
9 | 4.7 – 16.5 |
Most Common Tilt Angle |
0º to 5º | -5º – 53º |
% of the Time Spent in Most Common Tilt Angle |
47% | 32% – 63% |
2 nd Most Common Tilt Angle |
5º to 10º | -5º – 53º |
% of the Time Spent in 2 nd Most Common Tilt Angle |
31% | 3% – 62% |
Recline Access per Hour |
18 | 8 – 24 |
Average Time Recline was Accessed (min) |
3.5 | 2 – 6.7 |
Most Common Recline Angle |
Below 90º | 85º – 136º |
% of the Time Spent in Most Common Recline Angle |
56.5% | 33% – 91% |
2 nd Most Common Recline Angle |
90º to 95º | 85º – 136º |
% of the Time Spent in 2 nd Most Common Recline Angle |
31.5% | 9% – 60% |
The highest peak seat pressure recorded was 200 mmHg, thus 10% and 20% decreases in pressure occur at approximately 180 mmHg and 160 mmHg, respectively. During the calibration it was found that several tilt and recline angle combinations achieved such pressure reduction, and two sets of tilt and recline angle combinations were chosen for the analysis, i.e. 4º of tilt and 112º of recline for a 10% decrease, and 4º of tilt and 96º of recline for a 20% decrease. These combinations were chosen because, according to Table 1, the participant frequently used these angles. Table 2 shows that the subject used a seating position that decreased pressure at the seat by 20% more often and for a longer period of time than a position that decreased pressure by only 10%.
| Results | Ranges | |
|---|---|---|
| Number of Times Accessed per day (10% peak pressure decrease) | 1.5 | 0 – 5 |
| Accessed for How long (10%) (seconds) | 12 | 0 – 23 |
| Number of Times Accessed per day (20%) | 54 | 15 – 100 |
| Accessed for How long (20%) (seconds) | 62.5 | 18 – 227 |
DISCUSSION
Previous studies on the effects of seat tilt and back recline have revealed that larger tilt angles (> 25º), in combination with recline, help to reduce seat pressure and shear [5]. The participant only occasionally accesses angles over 25º, and these are accessed for short periods of time (usually a few seconds). On average the participant uses smaller angles of tilt and recline, but generally does not remain in an upright position (no use of tilt and recline) for extended periods of time. Combining the results of Tables 1 and 2, it seems that although the subject chooses smaller angles, they can still provide adequate pressure relief. The frequently used angles of 0º to 5º (tilt) and 90º to 95º (recline) correspond closely to seat position of 4º seat tilt and 96º back recline known to reduce pressure by 20%. Future work will involve data collection from more subjects and testing of the hypothesis. Further analysis to determine if tilt is used in combination with recline will also be conducted.
REFERENCES
- Xakellis GC, Frantz R. (1996). The cost of healing pressure ulcers across multiple health care settings. Adv Wound Care, 9:18–22.
- Sprigle S, Sposato B. (1997). Physiologic effects and design considerations of tilt and recline wheelchairs. Orthopedic Physical Therapy Clinics of North America, 6(1): 99-122.
- Cooper RA, Thorman T, Cooper R, Dvorznak M, Fitzgerald S, Ammer W, Guo S, Boninger M (2000). Driving Characteristics of Electric Powered Wheelchair Users. Ach of Phys. Med. & Rehab.,83:250-255.
- Hoover A, Cooper RA, Ding D et al. (2003). Comparing driving habits of wheelchair users: manual vs. power. RESNA proceedings, CD-ROM.
- Hobson DA (1992). Comparative effects of posture on pressure and shear at the body-seat interface. J Rehabil Res Dev., 29(4):21-31.
ACKNOWLEDGMENTS
This study is sponsored by the Center of Excellence on Wheelchair and Related Technology (WART), and NIDRR H133F040006.
AUTHOR CONTACT INFORMATION
Elizabeth P. Leister, BS
Human Engineering Research Laboratories
VA Pittsburgh Healthcare System
7180 Highland Drive, Building 4
2nd Floor East
Pittsburgh, PA 15206
Office Phone (412) 365-4850.
EMAIL: leisterl@herlpitt.org